Chondromyxoid Fibroma of Phalanges
Lubna S. Khan, Sifa Farheen, Vijay K. Pandey, Vinay P. Singh, Manoj G. Madakshira

TL;DR
A rare bone tumor called chondromyxoid fibroma was diagnosed in a 47-year-old woman's finger through imaging and histopathology.
Contribution
The paper presents a new clinical case of chondromyxoid fibroma in an unusual location and emphasizes the importance of histopathology for accurate diagnosis.
Findings
CMF was diagnosed in the left little finger of a 47-year-old female through imaging and histopathology.
Histopathology revealed a lobulated tumor with spindle to stellate cells in a myxoid and chondroid matrix.
Complete local excision is recommended to prevent recurrence, as local curettage may lead to tumor regrowth.
Abstract
Chondromyxoid fibroma (CMF) is a rare, benign metaphyseal bone tumour characterised by a combination of chondroid, myxoid, and fibrous elements. It can affect any bone at any age, with no gender predilection. We report a case of CMF in a 47-year-old female patient who presented with swelling of the left little finger at a tertiary care hospital in Kolkata, India, in 2024. Imaging revealed a lobulated lesion originating from the middle phalanx of the left little finger, extending to involve the base of the distal phalanx. Fine needle aspiration cytology indicated a moderately cellular myxoid lesion. Histopathology, which remains crucial for diagnosis, showed a lobulated tumour with zones of spindle to stellate cells, associated with an abundant myxoid and chondroid matrix in the intercellular spaces. Treatment involves complete local excision with tumour-free margins, as recurrence may…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
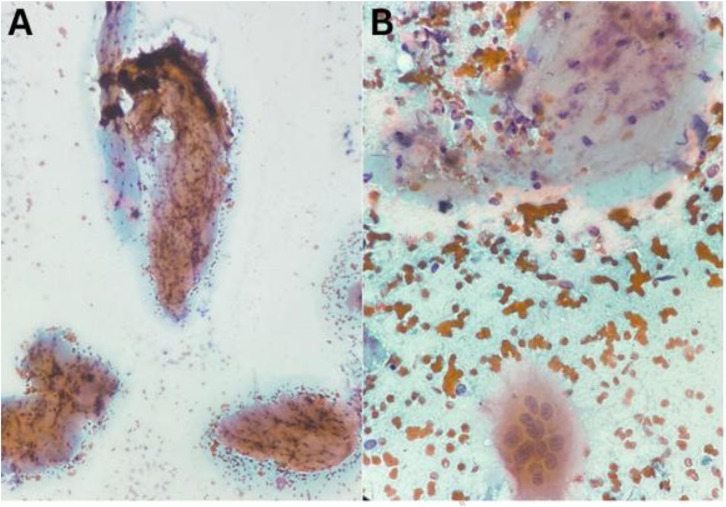 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3| S. NO | Author | Age | Gender | Site | Size | Nuclear pleomorphism on histology | Treatment | Follow-up | Recurrence |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Gupta | N/A | N/A | Phalanx of toe | N/A | Absent | N/A | N/A | N/A |
| 2 | Anderson | N/A | Female | Proximal phalanx of left ring finger | N/A | Absent | Curettage | 42 months | No recurrence |
| 3 | Zillmer | 3rd decade | N/A | Phalanx of hand | N/A | Absent | Curettage | N/A | Recurrence present |
| 4 | 3rd decade | N/A | Phalanx of foot | N/A | Absent | Curettage | N/A | No recurrence | |
| 5 | Bahk | 19 | Male | Distal phalanx of great toe | 4 cm | Present | Disarticulated at interphalangeal joint | 2 years | No recurrence |
| 6 | Kim | 53 | Female | Distal phalanx of left great toe | 3 cm | Present | Disarticulation at metatarsophalangeal joint | N/A | N/A |
| 7 | Yamamoto | N/A | N/A | Middle phalanx of index finger | N/A | Absent | N/A | N/A | N/A |
| 8 | Atalar | 8 | Male | Phalanx of great toe | N/A | Absent | Curettage | 46 months | No recurrence |
| 9 | Daghfous | N/A | N/A | Phalanx of thumb | N/A | Absent | Curettage | 9 months | Recurrence |
| 10 | Stotcavage | 29 | Female | Metacarpophalangeal joint of right ring finger | N/A | Absent | Curettage and synovectomy | 15 months | No recurrence |
| 11 | Bill Chang | 40 | Female | Distal phalanx of great toe | 2.3 cm | Absent | Amputation at the level of base of proximal phalanx | 6 years | No recurrence |
| 12 | Khan and Bandyopadhyay7 (2012) | 21 | Male | Middle phalanx of left middle finger | N/A | Present | Curettage | 2 months | No recurrence |
| 13 | Vasudeva | 11 | Female | Distal phalanx of great toe | N/A | Absent | Curettage | 6 months | No recurrence |
| 14 | Present case (2024) | 47 | Female | Middle phalanx of left fifth finger | 2 cm | Absent | Curettage | 6 months | No recurrence |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Sarcoma Diagnosis and Treatment · Oral and Maxillofacial Pathology
1. Introduction
Chondromyxoid fibroma (CMF) is a rare benign bone tumour of chondrogenic origin, accounting for less than 1% of all histologically confirmed primary bone tumours. CMF typically occurs in the metaphysis of long bones, with the distal femur and proximal tibia being common sites. While it is more prevalent in younger individuals, older patients may present with involvement of flat bones.^12^ Initially recognised as a distinct entity by Jaffe and Lichtenstein, CMF is both locally aggressive and benign. Clinically and radiologically, it can closely mimic chondrosarcoma, making accurate diagnosis challenging.^3^ Cytopathological evaluation, though difficult, remains a useful initial investigation when combined with clinical and radiological findings.^4^ In the 2020 WHO classification of bone tumours, CMF is now categorised as a benign chondrogenic tumour, having previously been considered an intermediate locally aggressive tumour.^5^ Although the exact cause remains unclear, the glutamate receptor GRM1 gene fusion, leading to promoter swapping and GRM1 upregulation, has been implicated in CMF.^6^ An analysis of the index case, alongside the existing literature on CMF involving the phalanx, will enhance our understanding of this rare condition.
2. Case report
A 47-year-old female patient was referred to a tertiary care hospital in Kolkata, India, in 2024, with a 2-year history of swelling in her left little finger. Over the past 3 months, she had experienced intermittent, vague pain and restricted movement. There was no history of trauma or signs of infection. Physical examination revealed an eccentric swelling, approximately 2 × 1 cm in size, located on the radial aspect of the distal left little finger. The overlying skin appeared normal. The lesion was fixed, tender, and firm, with the overlying tendons feeling free. Fine needle aspiration cytology revealed ill-defined fragments of myxoid stroma with oval to spindle-shaped cells having bipolar to stellate cytoplasmic processes, scattered singly alongside a few multinucleated giant cells, against a haemorrhagic background [Fig. 1A and B]. A provisional diagnosis of an “unclassified myxoid lesion” was made.
Papanicolau stained aspirate smears at magnification (A) ×100 and (B) ×400 show ill-defined moderately cellular fragments of myxoid stroma with oval to spindle-shaped cells having bipolar to stellate cytoplasmic processes, scattered alongside a multinucleated giant cell against a haemorrhagic background.
An X-ray of the little finger revealed an osteolytic, radiolucent, eccentric lesion in the metaphysis at the extensor aspect of the radial border of the middle phalanx and the proximal part of the distal phalanx of the left fifth finger [Fig. 2A]. Magnetic resonance imaging (MRI) showed a well-defined lobulated lesion involving the middle phalanx, arising from the underlying bone, with the adjoining distal phalanx showing pressure changes [Fig. 2B]. The lesion appeared isointense on T1 and heterogeneously hyperintense on T2/Proton-density weighted fat-suppressed (PDFS)/Short tau inversion recovery (STIR) sequences.
A: Radiograph (dorso-ventral view) showing an osteolytic, radiolucent, eccentric lesion in the metaphysis at the extensor aspect of the radial border of the middle phalanx and the proximal part of the distal phalanx of the left fifth finger. B: Magnetic resonance imaging (lateral view) showing a well-defined lobulated lesion involving the middle phalanx of the distal phalanx, arising from the underlying bone with the distal phalanx showing pressure changes.
The patient underwent local excision of the lesion through a curved incision over the dorsal aspect of the middle phalanx. Following reflection of the skin, the extensor tendon was identified and retracted to expose the lesion. Intraoperatively, the lesion was observed to arise from the middle phalanx, abutting the base of the distal phalanx, with no evidence of infiltration. The lesion was excised, and the underlying bone of the middle phalanx was curetted. The specimen measured 2 × 1 cm. The outer surface was smooth, and the cut surface revealed a grey-white, lobulated, heterogeneous lesion that felt gritty on cutting [Fig. 3A].
Haematoxylin and eosin-stained sections revealed a lobulated lesion with central bony trabeculae and marrow spaces, extending into variously sized lobules composed of chondromyxoid stroma [Fig. 3B]. These lobules exhibited peripheral hypercellular areas and inner hypocellular regions [Fig. 3C]. The cellularity mainly consisted of stellate to spindle cells with bland chromatin and pale eosinophilic cytoplasmic processes [Fig. 3D]. Grungy calcification was observed in some areas, along with a few peripherally located multinucleated giant cells [Fig. 3E]. There was no evidence of nuclear pleomorphism, necrosis, or mitosis. Alcian blue staining highlighted the acidic ground substance of the stroma. Immunohistochemistry with S100p (Clone Beta EP-32, ready to use, Pathnsitu) showed patchy nucleocytoplasmic expression in some of the stellate to spindle-shaped stromal cells [Fig. 3F].
A diagnosis of ‘chondromyxoid fibroma of the left little finger’ was made. The patient is currently on a 3-month follow-up schedule and has been without signs of recurrence for the past 9 months.
3. Discussion
Chondromyxoid fibroma is a rare bone tumour of chondrogenic origin, accounting for less than 1% of all bone tumours and less than 2% of all benign bone tumours. It is more commonly seen in long tubular bones around the knees, most frequently the proximal tibia.^125^ Involvement of the bones of the hands is extremely rare. The diagnosis is challenging and often requires clinico-radiological correlation with histopathological diagnosis. As Jaffe emphasized, “its recognition is of some importance in that pathologically it may be mistaken for sarcoma and, as such, treated more radically than necessary.”^2^
A literature search using MeSH terms ‘Chondromyxoid fibroma’ and ‘Phalanx’ revealed a total of 13 cases of CMF [Table 1]. Of these, 7 involved the phalanges of the foot, and 7 (including the index case) involved the phalanges of the hand. CMF of the phalanges shows a female preponderance. The age range was from 8 to 53 years, with the second and third decades being the most commonly involved. Clinical diagnosis is challenging, and misdiagnosis is not uncommon due to the varied symptoms presented by patients with CMF.^3^ Pain and swelling are the most consistent complaints, with or without mild to moderate tenderness, restriction of movement, and sometimes pressure symptoms, such as carpal tunnel syndrome or neurovascular deficits.^145^
Khan and Bandopadhyay reported a case of CMF in the middle phalanx of the left hand, misdiagnosed as Spina Ventosa, which was initially worked up as tubercular dactylitis.^7^ Clinical misdiagnosis of CMF as chondrosarcoma is also well documented.^28^ The differential diagnosis of CMF includes chondrosarcoma, chondroblastoma, fibrous dysplasia, non-ossifying fibroma, giant cell tumour, aneurysmal bone cyst, and simple bone cysts.^359^ On radiology, CMF is likely if there is a focal bone lesion showing geographic bone destruction, a sclerotic rim, lobulated margins, and septation.^39^ On MRI, chondromyxoid fibroma typically features a peripheral intermediate signal band and a central hyperintense signal on T2-weighted images, which generally correspond to the peripheral nodular enhancement and central non-enhancing portion on contrast-enhanced T1-weighted images.^3^
A: Excised specimen with a lobulated appearance and smooth surface. B: Haematoxylin and eosin stain (magnification at ×40) An encapsulated lobulated lesion. C: Haematoxylin and eosin stain (magnification at ×100) Peripheral hypercellularity with central hypocellularity. D: Haematoxylin and eosin stain (magnification at ×400) Spindle to stellate shaped cells in a myxoid stroma. E: Haematoxylin and eosin stain (magnification at ×400) Multinucleated giant cells in the periphery. F: Immunohistochemistry with S100p (Clone Beta EP-32, Ready to use, Pathnsitu) with nucleocytoplasmic expression in few spindle cells.
Because CMF can mimic many other bone lesions clinically and radiologically, histopathological confirmation of the biopsied specimen is essential for diagnosis. Fine needle aspiration cytology reveals the presence of spindle or stellate cells embedded in a chondroid matrix, essentially without hyaline material. The presence of hyaline material should raise suspicion of enchondroma or low-grade chondrosarcoma.^4^ Grossly, the lesion has a white lobulated appearance with a heterogeneous cut surface. Histopathological features typically show the lesion arranged in lobules, which may be prominent (macro lobular) or somewhat indistinct (micro lobular).^15^ On haematoxylin and eosin-stained sections, these lobules are composed of chondromyxoid stroma, with peripheral hypercellular areas and inner hypocellular regions. The cellularity is predominantly composed of stellate to spindle cells with bland chromatin and pale eosinophilic cytoplasm. Calcification may be present, along with osteoclastic giant cells.^15^
Bizarre nuclei have been reported in some cases without mitosis, which is likely a degenerative change in long-standing cases.^7810^ Bony permeation is not uncommon.^11^ However, the lack of infiltrative margins and the preservation of the zonation pattern are crucial for differentiating CMF from the more sinister chondrosarcoma.^2^ Chondroblastoma will typically show characteristic peri-cellular chicken-wire calcification, which is absent in CMF. Fibrous dysplasia and ossifying fibroma are medullary lesions that exhibit typical fibrous stroma associated with woven bone and calcification, respectively, which are absent in CMF.^3^ Giant cell tumour and aneurysmal bone cysts tend to have a greater number of osteoclastic giant cells scattered evenly and along vascular spaces, respectively.^359^ Simple bone cysts, on the other hand, are distinguished by their simple epithelial lining.^35^
Treatment options, based on careful patient selection, include curettage with or without cementation, wide local excision, and en-bloc resection. Approximately 9–15% of cases show recurrence following local resection.^5^ Recurrence is least likely with en-bloc resection; however, this approach often results in functional deficits and cosmetic concerns. Curettage alone has been associated with relatively high recurrence rates, up to 80%.^12^ Among phalangeal CMF cases, two managed by curettage showed recurrence.^1314^
The exact cause of CMF pathogenesis remains unclear. A study by Nord et al. provides substantial evidence that aberrant glutamate signalling plays a key role in the development of CMF. It shows that direct targeting of the glutamate metabotropic receptor 1 (GRM1) is a necessary and highly specific driver event for CMF development. The GRM1 gene recombines with several partner genes through promoter swapping and gene fusion events, leading to upregulation of GRM1, which has been implicated in the pathogenesis of chondromyxoid fibroma.^6^
There have been no known syndromic associations with CMF to date, and its co-existence as part of other pathological processes is rare. No malignant conversion of CMF has been reported in the literature. Reports of malignancy in cases of CMF, if any, have been attributed to instances where a chondrosarcoma was initially misdiagnosed as chondromyxoid fibroma.^78^
4. Conclusion
This case presents a rare instance of chondromyxoid fibroma involving the phalanges of the hand. While CMF can affect any bone in the body, involvement of the phalanges is extremely rare. It is often misdiagnosed clinically due to its rarity and the overlap of symptoms with other bone tumours. In such cases, histopathological examination remains the mainstay of diagnosis. Treatment options include local resection, wide local excision with free margins, and en-bloc removal. The recurrence rate is higher with local curettage, and en-bloc resection is considered the treatment of choice. A careful clinico-radiological evaluation, coupled with histopathological confirmation, ensures a correct, timely diagnosis and comprehensive treatment in cases of CMF.
Ethics Statement
The authors obtained written informed consent for publication from the patient and the manuscript is in accordance with the Institutional Ethics committee requirements.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contribution
SF conducted the cytopathological evaluation of the case. The surgery was performed by VKP and VPS. LSK and MGM handled the histopathological workup. The manuscript was prepared by LSK and MGM and subsequently reviewed and amended by SF, VKP and VPS. All authors approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zillmer DA Dorfman HD. Chondromyxoid fibroma of bone: Thirty-six cases with clinicopathologic correlation. Hum Pathol 1989; 20:952–64. https://doi.org/10.1016/0046-8177(89)90267-0.10.1016/0046-8177(89)90267-02793160 · doi ↗ · pubmed ↗
- 2Jaffe HL Lichtenstein L. Chondromyxoid fibroma of bone: A distinctive benign tumor likely to be mistaken especially for chondrosarcoma. Arch Pathol 1948; 45:541–51.18891025 · pubmed ↗
- 3Cappelle S Pans S Sciot R. Imaging features of chondromyxoid fibroma: Report of 15 cases and literature review. Br J Radiol 2016; 89:20160088. https://doi.org/10.1259/bjr.20160088.10.1259/bjr.2016008827226218 PMC 5124884 · doi ↗ · pubmed ↗
- 4Wangsiricharoen S Wakely PE Jr,Siddiqui MT Ali SZ. Cytopathology of chondromyxoid fibroma: A case series and review of the literature. J Am Soc Cytopathol 2021; 10:366–81. https://doi.org/10.1016/j.jasc.2021.04.001.10.1016/j.jasc.2021.04.00133958292 · doi ↗ · pubmed ↗
- 5WHO Classification of Tumours Editorial Board. Soft tissue and bone tumours. 5th ed. Lyon, France: International Agency for Research on Cancer. 2020. P. 362
- 6Nord KH Lilljebjörn H Vezzi F Nilsson J Magnusson L Tayebwa J. GRM 1 is upregulated through gene fusion and promoter swapping in chondromyxoid fibroma. Nat Genet 2014; 46:474–7. https://doi.org/10.1038/ng.2927.10.1038/ng.292724658000 · doi ↗ · pubmed ↗
- 7Khan K Bandyopadhyay A. A rare case of chondromyxoid fibroma mimicking spina ventosa. J Surg Tech Case Rep 2012; 4:43–5. https://doi.org/10.4103/2006-8808.100354.10.4103/2006-8808.10035423066464 PMC 3461778 · doi ↗ · pubmed ↗
- 8Bahk WJ Mirra JM Sohn KR Shin DS. Pseudoanaplastic chondromyxoid fibroma. Ann Diagn Pathol 1998; 2:241–6. https://doi.org/10.1016/s 1092-9134(98)80013-0.10.1016/s 1092-9134(98)80013-09845744 · doi ↗ · pubmed ↗