Mpox in the Gulf Cooperation Council Countries: Addressing a new challenge to regional health security
Salah Al Awaidy, Jaffar A. Al-Tawfiq, Faryal Khamis, Muna Al Maslamani, Jameela Al Salman, Sk Md Mamunur Rahman Malik

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
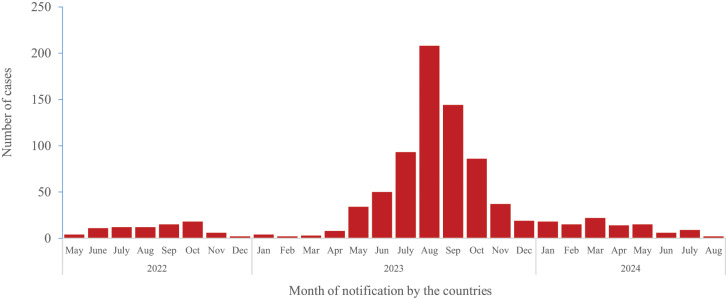 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Zoonotic diseases and public health · Bacillus and Francisella bacterial research
1. Introduction
Mpox (previously known as Monkeypox) is a zoonotic infectious disease caused by the monkeypox virus (MPXV), originally detected in 1970 in rural settlements inside the rainforest regions of Central and West Africa, when smallpox was in its final stages of eradication. The natural reservoir of this virus and how its circulation in nature is maintained remains unknown but it is common in primates.^1^
Mpox is endemic in Central and West Africa, and since its emergence in 1970, human cases have been reported in 11 African countries.^23^ In endemic countries, transmission primarily occurs from animals to humans through direct contact with infected animals, or their parts and secretions.^1^ Human-to-human transmission through prolonged and close physical contact with symptomatic induviduals, including sexual activity, is a significant factor that can trigger outbreaks.^1^
In May 2022, a cluster of cases was detected in the UK, with the index case having a travel history to Nigeria where an outbreak was ongoing.^4^ Subsequently, several countries in the European Union, and others in historically non-endemic regions reported, for the first time, multiple cases of mpox associated with significant human–human transmission across over 100 non-endemic and 7 historically endemic countries between 2022 and 2023.^5^
On 14 August 2024, WHO declared the upsurge of mpox outbreak in the Democratic Republic of the Congo (DRC) and in a growing number of countries in Africa as a public health emergency of international concern (PHEIC) under the International Health Regulations.^6^ While between 1 January 2022 to 9 November 2024, 109,699 clinically compatible cases of mpox including 236 deaths were reported from 123 countries and territories across the world, and total of 11,148 laboratory-confirmed cases of mpox including 53 deaths were reported from at-least 19 countries which includes 11 African countries.^7^ This was the second time that an outbreak of mpox has been declared as a PHEIC, after an earlier multi-country outbreak of mpox from July 2022 to May 2023.^7^ It appears that the WHO's determination in 2023, that the multi-country epidemic of mpox no longer represents a PHEIC, was premature.^8^ The recent upsurge of mpox cases in the DRC and other countries of Africa have been driven by outbreaks associated with clade Ib MPXV. Previously, clade Ia MPXV was responsible for a number of outbreaks in DRC and other countries in Africa and it was also the cause of the first outbreak of mpox in Africa in the 1970s, which had a fatality rate of more than 10% with most of the deaths occurred in children.^8^ The epidemiology of MPXV clade 1 continues to evolve and until recently it was mainly of zoonotic origin and only sporadic human-to-human transmission occurred within households.^9^
MPXV clade Ib, a novel clade of MPXV, was initially identified in the South Kivu province in DRC in September 2023, primarily affecting adults it is transmitted between individuals but not through sexual contact exclusively.^10^ The new subclade Ib was detected in DRC when the country was concurrently facing outbreaks of mpox caused by clade Ia MPXV since 2023.^10^ This shifting transmission pattern of the disease and the plausible lack of population immunity against the new clade of MPXV have raised global concern as infections are rapidly mounting and deaths occurring among all age groups. Cases linked epidemiologically and phylogenetically to the outbreak in the DRC, have also been detected in at-least 4 neighboring countries, which had not reported any mpox cases previously including Burundi, Kenya, Rwanda and Uganda. During the current 2024 outbreak, cases of mpox associated with MPXV clade Ia have been reported in the Central African Republic and the Republic of Congo. Cameroon, Cote d'Ivoire, Liberia, Nigeria, and South Africa have reported cases of mpox associated with MPXV clade II.^11^
1.1. Threat of mpox in the Gulf Cooperation Council countries and necessary measures to prevent and mitigate the spread
The United Arab Emirates (UAE) was the first Gulf Cooperation Council (GCC) country to report a case of mpox on 24 May 2023.^12^ In 2024, Saudi Arabia, reported 9 laboratory-confirmed cases with no deaths, mostly linked with travel history to endemic areas.^7^ Additionally, 3 cases of mpox were detected in Pakistan that were associated with a travel history to Saudi Arabia and the UAE.^13^
This indicates that MPXV has probably been circulating in the GCC countries but remained undiagnosed owing to lack of early detection for MPXV as well as unrecognised owing to failure of the current surveillance system to detect clinically compatible cases. Since May 2023, when the first case of mpox was reported in UAE, cases have continued to be detected across the GCC countries. Out of 869 laboratory-confirmed cases of mpox reported in the WHO Eastern Mediterranean Region, a total of 802 (over 92%) cases were reported from 5 GCC countries. These countries include Bahrain (2 cases), Saudi Arabia (764 cases), Oman (3 cases), Qatar (3 cases) and United Arab Emirates (28 cases). In 2024, only Saudi Arabia and United Arab Emirates, amongst the GCC countries, reported mpox cases.
Majority of the cases were reported during May to November 2023 even after the closure of WHO declaration of mpox as PHEIC [Fig. 1].
Number of laboratory-confirmed cases of mpox reported from the countries of World Health Organization Eastern Mediterranean Region.The epidemic curve is based on the data of mpox cases shared by the countries officially with the World Health Organization (WHO) in accordance with the International Health Regulations between May 2022 to August 2024. Data are extracted from WHO. 2022–24 mpox (Monkeypox) Outbreak: Global Trends. From: https://worldhealthorg.shinyapps.io/mpx_global/ Accessed: Dec 2024.
There is a reasonable possibility that as the virus circulating silently without being diagnosed, individuals with mild or asymptomatic infections of MPXV may transmit the virus to vulnerable populations, thereby perpetuating the human-to-human transmission chain and ultimately leading to an explosive outbreak if this transmission remains undetected. The available literature has also addressed the potential of non sexual transmission of MPXV through respiratory mode.^14^
Although the initial phase of the mpox outbreak was most likely caused by international travel, other modes of transmission that have not been linked to secondary cases have been reported in Saudi Arabia causing sustained human-to-human transmission.^15^ Currently, genomic data regarding the circulation of clade IIb MPXV is exclusively available from Saudi Arabia, while there is no information on the circulating clade and sub-clade types of MPXV from other GCC countries. This lack of data complicates the assessment of mpox risk in the GCC countries, particularly for vulnerable populations such as sex workers, pregnant women, children and immunocompromised individuals. More information is required to fully understand the dynamics of transmission, high-risk populations and the risk of exposure to mpox.
Recent evidence suggested that mpox can also be transmitted through respiratory droplets and through sexual contact, which increases the risk of human-to-human transmission^111^ In this regard, a mathematical model that examined the possibility of spread of mpox at the FIFA World Cup 2022 in Qatar estimated that 3.6 (95% confidence interval: 3.2–4.1) travel-associated mpox cases may be imported into Qatar and the surrounding Gulf countries.^16^
Despite the ongoing reporting of mpox cases within the GCC countries, and the potential for a significant rise in certain countries, the implementation of necessary public health measures to prevent further transmission and mitigate the risk of sustained human-to-human transmission has not been prioritised. The necessary public health measures include enhancing surveillance and laboratory testing for rapid detection of cases, targeted risk communication among the high-risk groups as well as in health workers for early identification of suspected cases and integrating genomic sequence into routine public health surveillance system. Complacency may allow the virus to persist and proliferate, as testing remains insufficient, cross-country surveillance and information sharing are sub-optimal, and public awareness of the risk of infection is low. We are not aware of the circulating clad of MPXV in the GCC countries except in Saudi Arabia and recent evidence has shown that significant rise in number of cases and deaths in all age groups may occur rapidly in case of the more transmissible form of the virus such as clade Ib MPXV continue to circulate unabated.
The GCC countries are renowned global tourist and economic hubs, and they also host significant populations of migrant workers living in communal housing; all these factors could potentially facilitate the rapid transmission of mpox. A major outbreak of MPXV in the GCC countries may strain the GCC's health-care system as they recover from the COVID-19 pandemic. Owing to the potential of the MPXV to spread widely through travel, tourism and trade with implications for mass gatherings and long-term economic consequences, there is a heightened need for increasing public health vigilance and readiness for early detection and response in the GCC countries despite the current risk assessment indicates that the countries are at low risk.^111516^
To address the challenges caused by mpox in the GCC countries, it is essential to place a multi-sectoral approach beginning with political commitment to prioritise mpox as a public health emergency, along with preparedness, targeted research efforts and vaccination.
1.1.1 Political attention through multi-sectoral approach
Prevention and control of mpox require a comprehensive approach that involves public health authorities, healthcare providers and the public. GCC countries should prioritise mpox similar to COVID-19 outbreak and Middle East Respiratory Syndrome.^1^ The health authorities must be vigilant and establish collaborative regional committees for coordination, risk communication and building capacities for effective control.
1.1.2. Readiness of health systems and preparedness of case management in health facilities
Preparedness and readiness for mpox requires capacity enhancement, medical supplies availability and training of healthcare workers. Enhancing surveillance systems and an effective contact tracing system for identifying close contacts of cases are important for stopping the transmission chain in an ongoing outbreak. The surveillance systems need to employ sentinel, syndromic, and event-based methods to detect cases early and track the spread of the disease.^1^ Each GCC country's preparedness and response capabilities level can influence the potential impact of mpox transmission. A one health approach is critical to address the zoonotic nature of mpox.^4^ Another strategy for readiness includes education and awareness programmes particularly about the spread of the disease, incubation period and isolation measures. Conducting knowledge, attitudes and practices surveys can provide valuable insights into public perceptions and behaviours regarding mpox, guiding more effective communication strategies. These activities should be provided in multiple languages as GCC countries have large population of immigrant workers.
Case management protocols must be developed or updated to reflect the latest knowledge about mpox, with a focus on clinical care pathways for the management of mild and severe cases of mpox in healthcare facilities and at home and the readiness of health facilities to handle potential surges in cases.
1.1.3. Vaccination
WHO does not endorse any form of mass vaccination for the prevention and management of mpox. Nevertheless, WHO, has granted emergency use listing for use of 2 ‘third-generation’ mpox vaccine in humans so far. On 8 October 2024, the WHO authorised the use of Modified Vaccinia Ankara–Bavaria Nordic (also known as Imanvex, Imvamune or Jynneos) in an outbreak setting, administered as a 2-dose subcutaneous injection to individuals aged 12 years and older, given 4 weeks apart. On 19 November 2024, the WHO authorised the use of LC16m8 mpox manufactured by KM Biologics in Japan for use in an outbreak setting for individuals over 1 year of age as a single dose vaccine via a multiple puncture techniques using a bifurcated needle.^17^
The Centre for Disease Control recommends 2 doses of Jynneos vaccine to be taken 28 days apart for high-risk population of getting the mpox.^17^ In GCC countries, mpox vaccination strategies are not robust as there have not been many detected cases so far. However, countries in the region should ensure the availability and accessibility of a vaccine for at-risk populations. In Saudi Arabia during the 2022 outbreak, individuals in a high-risk population such as healthcare professionals, laboratory workers and those who have close contact with an affected person were offered post-exposure vaccination with the smallpox/mpox vaccine (Jynneos), with 2 doses 1 month apart as soon as possible and within 4 days after exposure.^12^ In Bahrain, as per the Ministry of Health, the mpox vaccines are available, and a comprehensive preventive plan for combating mpox is assured to its citizens.^13^
The GCC countries may devise a strategy for the deployment of mpox vaccines if the need arises as part of response to an outbreak. The list of high-risk population groups as well as other groups such as health workers should be prioritised based on epidemiological data who should be offered vaccination if the outbreak situation worsens, considering the limited supply of vaccinations globally scale.
1.1.4. Data sharing and research collaboration
Addressing the knowledge gaps through research is essential.^56^ Increased collaboration across different nations in terms of clinical research trials to develop viable vaccines and treatments is necessary in preventing a potential pandemic.
Information and data on mpox should be shared among the GCC countries to understand the epidemiology, determine the priority groups for vaccination against MPXV and enable the development of appropriate clinical management pathways for mpox cases and immune-compromised individuals. The GCC Centre for Disease Control could adopt a more proactive approach to enhance coordination among the GCC countries, particularly in the context of data sharing. However, the GCC Centre for Disease Control had reported a risk assessment of the current mpox outbreak and felt that the risk is low in GCC countries.
1.2. The way forward
GCC countries should increase their capacity for laboratory testing and implement a behavioural change intervention programme aimed at the high-risk groups. Free and abundant access to mpox diagnostics would ensure that individuals can access testing without facing stigma or prejudice. Since the majority of mpox infections are mild and self-limiting, it is crucial to increase public awareness via social and electronic media for voluntary testing and reporting among the general public and among high-risk populations.
Simultaneously, the GCC should improve surveillance by syndromic monitoring for skin rashes and sexual transmitted infections, with access to prompt diagnostics and contact tracing. Enhancing genomic surveillance for MPXV, including clade and strain identification, would be especially important so that changes in the disease's shifting epidemiology and transmission patterns could be tracked and detected.
To effectively manage an outbreak, GCC countries should improve public awareness, strengthen surveillance as well as early screening especially for identified LGBT groups. The current mpox threat provides an opportunity to improve infection prevention and control strategies in healthcare settings, which will benefit the control of a wide range of other zoonotic diseases.
2. Conclusion
The current worldwide epidemic of mpox is neither the first nor the final significant global health security threat that the GCC countries have faced in the past or will face in the future; these threats warrant the attention of the highest political leadership in these countries. The health systems of GCC countries, in the post COVID-19 era, are better equipped and more prepared to confront the ‘disease X’ or any future pandemic than before. Due to the rapid urbanisation and mobility of individuals within the GCC countries, as well as changes in environmental, climate and ecological factors, international travel and interconnectivity, diseases with epidemic potential will emerge, evolve, rapidly spread and eventually, test the GCC countries’ capacity to identify, respond to and prevent such health security threats effectively. Failure to do so is not an option, as it will have devastating consequences for the economy, sustainable development and the welfare of the population in the GCC countries.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
SA, FK, JA, MM, JAL and SMRM conceptualised the idea. All authors were involved in the information extraction and literature review for this manuscript. All authors were also involved in designing, structuring and revising this manuscript. All authors approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Branda F Romano C Ciccozzi M Giovanetti M Scarpa F Ciccozzi A. Mpox: An overview of pathogenesis, diagnosis, and public health implications. J Clin Med 2024; 13:2234. https://doi.org/10.3390/jcm 13082234.10.3390/jcm 1308223438673507 PMC 11050819 · doi ↗ · pubmed ↗
- 2Jezek Z Grab B Szczeniowski MV Paluku KM Mutombo M. Human monkeypox: Secondary attack rates. Bull World Health Organ 1988; 66:465–70.2844429 PMC 2491159 · pubmed ↗
- 3Al Awaidy ST Khamis F Sallam M Ghazy RM Zaraket H. Monkeypox (mpox) Outbreak: More queries posed as cases soar globally. Sultan Qaboos Univ Med J 2023; 23:1–4. https://doi.org/10.18295/squmj.8.2022.046.10.18295/squmj.8.2022.04636865422 PMC 9974023 · doi ↗ · pubmed ↗
- 4Hraib M Jouni S Albitar MM Alaidi S Alshehabi Z. The outbreak of monkeypox 2022: An overview. Ann Med Surg (Lond) 2022; 79:104069. https://doi.org/10.1016/j.amsu.2022.104069.10.1016/j.amsu.2022.10406935860140 PMC 9289401 · doi ↗ · pubmed ↗
- 5Laurenson-Schafer H Sklenovská N Hoxha A Kerr SM Ndumbi P Finer J. Description of the first global outbreak of mpox: An analysis of global surveillance data. Lancet Glob Health 2023; 11:e 1012–23. https://doi.org/10.1016/S 2214-109X(23)00198-5.10.1016/S 2214-109X(23)00198-537349031 PMC 10281644 · doi ↗ · pubmed ↗
- 6World Health Organization. WHO Director-General declares mpox outbreak a public health emergency of international concern. https://www.who.int/news/item/14-08-2024-who-director-general-declares-mpox-outbreak-a-public-health-emergency-of-international-concern Accessed: Dec 2024.PMC 1137670039218470 · pubmed ↗
- 7Lee SS Bockarie MJ Al-Tawfiq JA. Was the public health emergency status of mpox ended too soon? Int J Infect Dis 2023; 134:301–2. https://doi.org/10.1016/j.ijid.2023.06.024.10.1016/j.ijid.2023.06.02437550010 · doi ↗ · pubmed ↗
- 8World Health Organization. WHO Director-General's statement at the press conference following IHR Emergency Committee regarding the multi-country outbreak of monkeypox. From: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-the-press-conference-following-IHR-emergency-committee-regarding-the-multi–country-outbreak-of-monkeypox–23-july-2022 Accessed: Dec 2024.