Ischiopubic Osteochondrosis (Van Neck-Odelberg Disease) as a Rare Cause of Pediatric Hip Pain: A Systematic Review
Cameron Gerhold, Renish N Contractor, Matthew McGee, Jacob Myhre, Michael Sweeney

TL;DR
Van Neck-Odelberg disease is a rare cause of hip pain in children that is often misdiagnosed, but can resolve within weeks with proper recognition.
Contribution
This systematic review compiles and analyzes case reports to highlight diagnostic challenges and clinical features of Van Neck-Odelberg disease.
Findings
Most patients were male with a median age of 12 years and presented with groin pain.
Common misdiagnoses included fractures, ischial ramus tumors, and osteomyelitis.
Symptoms typically resolved within eight weeks without invasive treatments.
Abstract
Overgrowth of the ischiopubic synchondrosis, a junction between the inferior pubic ramus and ischium, leads to the development of Van Neck-Odelberg disease. This condition is a rare cause of pediatric hip pain and limping that is often misdiagnosed due to its rarity and non-specific presentation. A review of the literature was conducted on PubMed, Cochrane, Embase, and Web of Science to identify case reports and case series of Van Neck-Odelberg disease using the keywords “Van Neck-Odelberg Disease” and “Ischiopubic Osteochondrosis.” A total of 115 studies were identified. After applying exclusion criteria, 15 studies remained. Most patients were male (n = 16; 84.2%), and the median age was 12 years (range = 5.5-17 years). The most common presenting symptoms were groin pain (n = 16; 84.2%), limping and gait limitation (n = 9; 47.4%), and restricted hip range of motion (n = 4; 21.1%). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
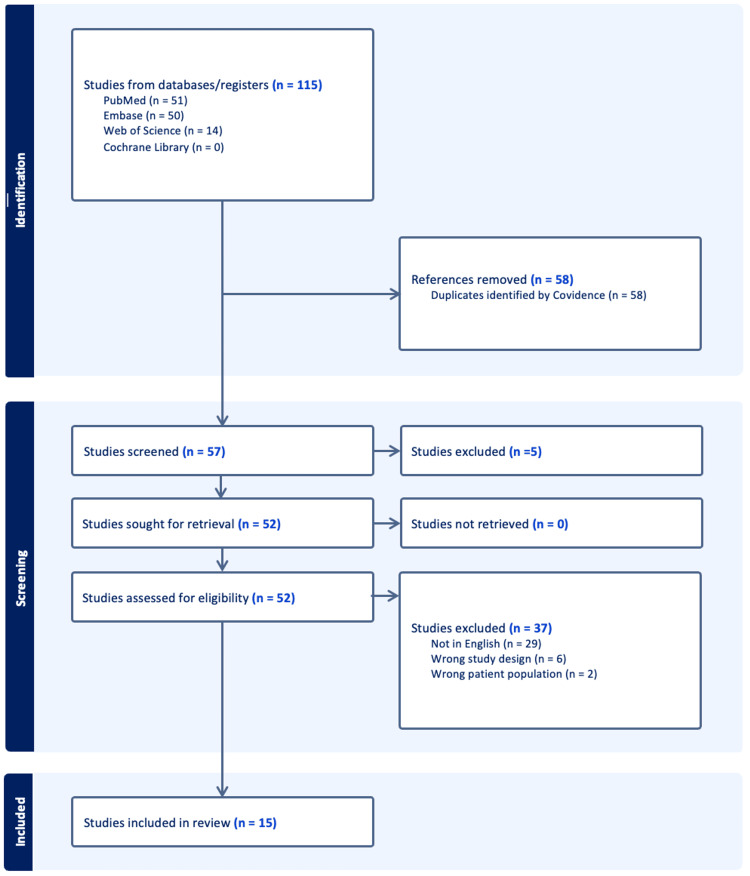 Figure 1
Figure 1| Author (year) | Article type | Age (years) | Sex | Activities | Presenting symptoms | Time to presentation | DDx | Treatment plan | F/u and results |
| Beyitler and Kavukcu (2016) [ | Case report | 7 | Male | - | Radiating groin pain; NWB on affected side; tender hip adductors; restricted hip ROM | Immediate presentation | Subacute fracture | Rest; analgesics | 3-week f/u revealed complete resolution of symptoms |
| Camacho et al. (2020) [ | Case report | 15 | Nale | - | Non-radiating, sharp pain in iliac fossa and hypogastrium; gait limitation | 3 months | Ischiopubic ramus fracture | - | - |
| Ceri and Sperati (2020) [ | Case report | 8 | Male | - | Groin pain to palpation; limping; restricted leg ROM | 20 days | - | Rest; NSAIDs; abstain from sports until symptoms resolution | 30-day f/u revealed complete resolution of symptoms |
| Ceroni et al. (2004) [ | Case report | 5.5 | male | - | Gluteal pain, limping, no hx of trauma, tender IPS; no local swelling; contracture of adductor muscles; limited hip ROM | 4 days | Osteomyelitis; tumor of the ischial ramus | Rest; NSAIDs | Complete resolution of symptoms within 48 hours |
| Chaudhari et al. (2017) [ | Case report | 12 | Male | - | Groin pain; limping; no local swelling | 2 months | Stress fracture; osteomyelitis; tuberculosis; post-traumatic osteolysis; neoplasia | Rest for 3 weeks; NSAIDs | 3-month f/u revealed complete resolution of symptoms |
| Fonseca et al. (2022) [ | Case report | 6 | Male | Futsal | Inguinal pain; limping; bilateral valgus knees; dynamic flat foot; tender ischiopubic area and adductors; limited hip ROM; reduced adductor and rotator muscle strength | - | - | Rest; abstain from sports for 6 weeks | 8-week f/u revealed minimal improvement, continued pain, and a limp. A rehabilitation program was prescribed. |
| Laliotis et al. (2022) [ | Case series | 13 | Male | Football | Hip pain; limping; normal ROM and mobility; tender ischium | 3 weeks | SCFE | Rest; PWB with crutches for 1 month | 3-month f/u revealed complete resolution of symptoms |
| Laliotis et al. (2022) [ | 14 | Male | Sports | Tender ischial tuberosity | 3 months | PWB with crutches for 1 month; abstain from sports | 4-month f/u revealed complete resolution of symptoms | ||
| Laliotis et al. (2022) [ | 11 | Male | sports | Tender ischial tuberosity | 3 months | PWB with crutches for 1 month; abstain from sports | 5-month f/u revealed complete resolution of symptoms | ||
| Laliotis et al. (2022) [ | 10 | Female | Dancing | Hip pain | 2 months | Subacute osteomyelitis | Conservative management | 4-week f/u revealed complete resolution of symptoms | |
| Macarini et al. (2011) [ | Case series | 8 | Male | Ischiopubic pain; limping; no adductor muscle contracture | 1 month | Rest; NSAIDs | 3-week f/u showed drastic symptom improvement; 4-week f/u MRI revealed decreased perilesional edema | ||
| Macarini et al. (2011) [ | 12 | Male | Football | Hip pain; inability to ambulate | Immediate presentation | Rest; NSAIDs | 2-week f/u revealed complete resolution of symptoms | ||
| Mixa et al. (2017) [ | Case report | 15 | Female | Groin pain | Immediate presentation | - | Conservative management | 3-month f/u revealed complete resolution of symptoms | |
| Morse and Lin (2016) [ | Case report | 17 | Female | Soccer, cheerleading | Groin and thigh pain; no hx of trauma; mild pain in the ischial tuberosity region with resisted knee flexion | 2 years | Acute hematogenous osteomyelitis; stress fracture; enchondroma; Ewings sarcoma or osteosarcoma; fibrous dysplasia; eosinophilic granuloma; bone cyst; osteochondrosis | Conservative; abstain from sports until symptom resolution | 4-month f/u revealed worsening symptoms; 1-year f/u revealed complete resolution of symptoms |
| Pirimoglu and Sade (2019) [ | Case report | 8 | Male | - | Groin pain; no hx of trauma | Immediate presentation | Fracture, infection, or bone tumor | Rest; NSAID for 3 weeks | - |
| Sabir et al. (2021) [ | Case report | 14 | male | - | Gluteal, groin, and perineal pain; restricted physical activity; no hx of trauma | 1 year | Stress fractures, osteomyelitis, neoplastic processes, and enthesitis-related arthritis | Rest; 3-week course of NSAIDs | 3-year f/u revealed complete resolution of symptoms |
| Schneider et al. (2020) [ | Case report | 12 | Male | Sports | Inguinal pain | 3 months | Bone tumor | Conservative management | 6-month follow-up revealed complete resolution of symptoms |
| Tam et al. (2021) [ | Case report | 12 | Male | - | Bilateral groin pain; limping | 18 months | VND | Conservative management | Symptoms resolved with skeletal maturity |
| Walter et al. (2020) [ | Case report | 10 | Male | - | Radiating groin pain; no hx of trauma | 4 months | Pathological pubic ramus fracture | Pain-adapted FWB | 4-month f/u revealed no disease progression |
| Author (year) | Laboratory values | CT findings | MRI findings | X-ray findings |
|
Beyitler and Kavukcu (2016) [ | Increased leukocytes; normal CRP and ESR | - | Hypointense sclerotic discontinuity of anterior pubic ramus; perilesional edema | Enlarged right IPS with osteolytic areas |
|
Camacho et al. (2020) [ | WNL | Focal increased uptake at IPS; expansion of medial ischiopubic ramus; adjacent soft tissue edema | - | - |
|
Ceri and Sperati (2020) [ | WNL | - | VND of the left ischiopubic ramus | - |
|
Ceroni et al. (2004) [ | Elevated CRP and ESR; blood exam normal | - | Bone marrow of the right IPS as well as adjacent muscles had a hyperintense signal alteration; hypointense band centered the right ischiopubic bone marrow | Anteroposterior radiographs of pelvis revealed a normal appearance of the IPS; right-sided radiolucent swelling noted |
|
Chaudhari et al. (2017) [ | WBC WNL; ESR raised with positive CRP ratio | Enlarged non-fused IPS containing lytic lesions | Hyperintense signal on T2; hypointense signal on T1 | Sclerotic shadow seen in IPS extending towards the obturator foramen |
|
Fonseca et al. (2022) [ | WNL | - | - | Demineralization and hypertrophy of the right IPS |
|
Laliotis et al. (2022) [ | - | - | Calcified osteochondral mass | Irregular calcification of right ischium |
|
Laliotis et al. (2022) [ | - | - | Edema of the ischium | Irregular cortex of the left ischium; line of calcification |
|
Laliotis et al. (2022) [ | - | - | Bilateral edema of the IPS | Enlargement and diastasis of the IPS |
|
Laliotis et al. (2022) [ | WNL | - | Ischial edema | Diastasis and enlargement of the IPS |
|
Macarini et al. (2011) [ | Increased CRP and ESR; normal ASO titer | Demineralization and sclerosis at edges of the synchondrosis | Hypointense band perpendicular to pubic axis; edema of tissue and muscles surrounding lesions | Right IPS was enlarged with osteolytic regions |
|
Macarini et al. (2011) [ | Increased CRP; normal ASO titer | Left IPS shows delayed closure and irregular bone margins | Left IPS fusiform enlargement | Left IPS enlargement with radiolucency |
|
Mixa et al. (2017) [ | - | - | Completed | Completed |
|
Morse and Lin (2016) [ | WNL | Calcifications within the lesion; cortices appeared focally incomplete anteriorly and posteriorly; areas of endosteal scalloping | Lesion had relatively low signal intensity on T1-weighted images but mirrored that of red marrow making it hyperintense to muscle | Well-marginated expansile lesion of the left inferior pubic ramus |
|
Pirimoglu and Sade (2019) [ | - | - | Hyperintense edema, swelling, corticomedullary discontinuity and slightly contrast enhancement pattern at left IPS | Enlarged left IPS characterized by focal osteolytic area |
|
Sabir et al. (2021) [ | WNL | - | Transverse hypointense fibrous band surrounded with edema in the region of the right IPS seen at low signal intensity on T1-weighted MRI | Expansion of the right IPS; epiphyses were open |
|
Schneider et al. (2020) [ | - | - | - | Extensive, partly demineralized geographic lesion with no periosteal reaction at the junction of the pubic bone and the ischium |
|
Tam et al. (2021) [ | - | - | Left fusiform IPS expansion with increased signal intensity in the bone and adjacent soft tissue; and absence of synovitis, soft tissue mass, or collections | Expansion of IPS bilaterally (left > right) with normal hips |
|
Walter et al. (2020) [ | - | - | Completed | Completed |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip disorders and treatments · Sports injuries and prevention · Injury Epidemiology and Prevention
Introduction and background
Van Neck-Odelberg disease (VND) is a skeletal abnormality consisting of an overgrowth of the ischiopubic synchondrosis (IPS), which serves as the junction between the inferior pubic ramus and ischium [1]. The condition was termed Van Neck-Odelberg after it was first described in the early 1920s by Odelberg and Van Neck and was described as “osteochondritis ischiopubica” [2,3]. VND is a rare condition that typically occurs in adolescents during skeletal maturation and can occur unilaterally or bilaterally. Patients typically present with groin or gluteal pain and difficulty ambulating.
The ischiopubic area of the pelvis is formed by the superomedial aspect of the pubis and the posterolateral aspect of the ischium. There is cartilaginous tissue that forms a joint where these two bones meet, called the IPS, and an overgrowth of this tissue causes VND [4]. This area forms embryologically at five to six months of fetal life, and fusion of the cartilage is complete at term. Ossification of the cartilage occurs during puberty. In rare instances, asymmetrical growth of the IPS can lead to increased stress on the pelvis, leading to VND [5]. This leads to an inflammatory response, which can subsequently delay ossification of the IPS [6].
The condition is self-limiting and can occur until ossification of the IPS occurs [7]. Once ossification occurs during puberty, no residual deformity is found. This condition can mimic fracture, infection such as osteomyelitis, trauma, tumors, or enthesitis-related arthritis. Clinically, pain in the pelvic region with the absence of fever and normal laboratory results helps narrow down the differential diagnosis. We present a systematic review of all published reports of VND, including details on presenting symptoms, diagnostic imaging results, treatments, and other details about the cases. The purpose of this review is to provide the most comprehensive overview of this rare disease with the aim of determining if there is an optimal treatment option.
Review
Methodology
This systematic review on VND adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [8]. Additionally, it was registered on PROSPERO (ID: 1040621). This review aims to review the various presentations of VND and determine is there is an optimal treatment option for this rare diagnosis.
Eligibility Criteria
This review included all studies that were either a case report or a case series on VND. Studies were excluded if (1) VND was not the final diagnosis, (2) important details regarding diagnostic workup and treatment were not included, (3) they were designed as cross-sectional, cohort, case-control, and clinical trials; or (4) meta-analyses or systematic reviews.
Search Strategy
A literature search was conducted on PubMed, Cochrane, Embase, and Web of Science to identify case reports and case series of VND, also known as ischiopubic osteochondrosis, up to October 1, 2023. Keywords utilized in the database searches were “Van Neck-Odelberg Disease” and “Ischiopubic Osteochondrosis.” Manual citation searches and citation tracking were also performed to ensure inclusion of all relevant studies.
Selection Process
All search results from each database were imported into Covidence, a management software used to organize systematic review data, which automatically screened for duplicates [9]. Titles and abstracts were independently screened by two authors (CJG and RNC), who excluded irrelevant studies. Full-text articles were then independently screened for inclusion eligibility by two authors (CJG and RNC). A third author (MDM) mediated any conflicts in consensus between the first two article screeners (CJG and RNC).
Data Extraction and Items Collected
After the final set of articles was collected, data extraction was accomplished by two authors (CJG and RNC) and subsequently verified for completeness and correctness by a third author (MDM). Data extracted from each case report or case series included the last name of the first author, year of publication, article type, patient age (years), sex of the patient, patient activities, Extracted information on the clinical course consisted of (1) details of the initial presentation; (2) time to presentation or referral; (3) differential diagnoses; (4) laboratory values: erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), white blood cell (WBC) count, and red blood cell (RBC) count; (4) diagnostic imaging: CT, MRI, and X-ray; (5) treatment regimens; and (6) information about symptom resolution as well as follow-up data.
Bias Assessments of Included Studies
The Joanna Briggs Institute (JBI) critical appraisal checklist for case reports and case series was used to dictate the quality of the included case reports and case series [10,11]. The JBI critical appraisal checklist for case reports consists of an eight-question checklist. This checklist was used to evaluate the comprehensiveness of the data included within each case report, including patient demographics, patient’s past medical history, presenting symptoms, diagnostic tests and assessment methods, interventions and treatments, post-intervention clinical condition, adverse or unanticipated events, and summarized takeaway lessons [10]. The JBI critical appraisal checklist for case series consists of a 10-question checklist. This checklist allowed for proper evaluated of the data included within each case series, including the inclusion criteria for the case series, the method of condition standardization for all patients included in the case series, condition identification methods, patient demographics and clinical information, outcomes and results of cases, clarity of reporting of presenting site or clinic demographic information, and whether statistical analysis was appropriate [11].
Results
Study Selection
In total, 115 articles were identified utilizing search terms in four databases: PubMed (n = 51), Embase (n = 50), Web of Science (n = 14), and Cochrane (n = 0). Covidence automatically removed 58 duplicate articles, leaving 115 articles to screen titles and abstracts for eligibility. Five studies were deemed irrelevant while performing a title and abstract screening, leaving 52 articles to be screened during a full-text review. Of these 52 articles, 37 were excluded (29 studies were excluded for not being written in English, six studies were excluded for having the wrong study design, and two studies were excluded for having the wrong patient population). The resulting 15 studies were included in this study (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart detailing the literature search and data selection process.
Study Characteristics, Patient Characteristics, and Clinical Assessment of VND
The 15 studies included in this systematic review described 19 cases of VND. The baseline characteristics of each study, the study participants, and clinical course are shown in Table 1. Of the 19 cases, 16 were male (84.2%). The median age was 12 years (range = 5.5-17 years). The median time to presentation was 60 days (range = immediate presentation to 2 years). The most common presenting symptoms were hip and groin pain (n = 16; 84.2%), limping and gait limitation (n = 9; 47.4%), restricted hip range of motion (n = 4; 21.1%), a tender ischial tuberosity (n = 3; 15.8%), a tender IPS (n= 3; 15.8), and tender hip adductors (n = 2; 10.5%). Other presenting symptoms include inability to bear weight on the affected side (n = 1; 5.3%), dynamic flat foot (n = 1; 5.3%), bilateral valgus knees (n = 1; 5.3%), and reduced hip rotator and adductor strength (n = 1; 5.3%). The most common treatments were rest (n = 11; 57.9%), analgesics (n = 10; 52.6%), abstinence from sports (n = 6; 31.6%), conservative management (n = 6; 31.6%), partial weight bearing with crutches (n = 3; 15.8%), and one individual experienced symptom resolution with pain-adapted full weight bearing. The most common differential diagnoses were fractures (n = 7; 36.8%), tumor of the ischial ramus (n = 6; 31.6%), and osteomyelitis (n = 5; 26.3%). Other differentials included fibrous dysplasia (n = 1; 5.3%), post-traumatic osteolysis (n = 1; 5.3%), tuberculosis (n = 1; 5.3%), slipped capital femoral epiphysis (n = 1; 5.3%), eosinophilic granuloma (n = 1; 5.3%), bone cyst (n = 1; 5.3%), osteochondrosis (n = 1; 5.3%), infection (n = 1; 5.3%), and enthesitis-related arthritis (n = 1; 5.3%). The median time to resolution was eight weeks (range = 2 days to 3 years). Overall, 15 of the 19 individuals included in this study experienced complete resolution of symptoms.
Diagnostic Workup of VND
Laboratory values, CT findings, MRI findings, and X-ray findings of the cases included in this study are described in Table 2. Laboratory findings included elevated CRP (n = 4; 21.1%), elevated ESR (n = 3; 15.8%), and increased leukocytes (n = 1; 5.3%). CT findings included irregular IPS margins (n = 3; 15.8%), an enlarged ischiopubic ramus (n = 2; 10.5%), adjacent soft tissue edema (n = 1; 5.3%), focal increased uptake at the IPS (n = 1; 5.3%), and delayed IPS closure (n = 1; 5.3%). While there are currently no known pathognomonic CT findings for this disease, these are the most commonly reported.
Risk of Bias Assessment
The risk of bias assessment was assessed for all 15 included studies (2 case series and 13 case reports) using the JBI critical appraisal tool. One case report received “yes” to only six of the eight questions found on the JBI critical appraisal tool, while the remaining 12 case reports had a score of either 7 or 8. The average risk bias assessment score for all 13 included case reports was 7.15/8. Both case series included in this study received a JBI critical appraisal tool score of 9.
Discussion
Ischiopubic osteochondrosis is a cause of pediatric hip pain that is often misdiagnosed due to its rarity. Delaying proper diagnosis causes prolonged pain and impaired movement for individuals suffering from this disease, who are pediatric patients and often are unable to participate in activities, such as sports, until this disease is fully resolved.
Analysis of all published cases of VND reveals an interesting correlation between time until full symptom resolution and time to treatment from the initial onset of symptoms. While most patients received treatment upon presentation for the immediate onset of symptoms, some patients waited months or years before seeking professional help from clinicians. One case described a patient who waited two years after the initial onset of symptoms to see a pediatric orthopedic specialist and received a formal diagnosis of VND [19]. This patient was also the oldest of all published cases of VND (17 years old) and had one of the longest times to complete recovery (one year). This patient’s four-month follow-up suggested that the lesion had grown on subsequent imaging studies, but the study did not note any changes in her symptoms. At the sixth-month follow-up, her symptoms were improving, and she progressed in her activities. A subsequent follow-up at one year, the patient was asymptomatic and made a full return to athletic activities, along with the disappearance of the lesion on imaging studies. Another patient presented one year after the onset of symptoms and saw a prolonged time to full symptom resolution (three years) [5]. There could also be a correlation between age at symptom onset and time to symptom resolution based on a review of all cases included in this study. There is a general pattern of older individuals having a prolonged time to full symptom resolution. The two aforementioned individuals are among the oldest included in this study, at 14 and 17 years of age. These individuals experienced the longest time to recovery of any individuals included in this study. Although patients older than 12 years old did have a longer time from the initial onset of symptoms to diagnosis and treatment of VND. This may be attributed to VND being lower on the differential diagnosis in this age group and the rarity of the condition itself compared to other conditions on the differential diagnosis. In the oldest reported patient, a 17-year-old female, the presentation was unusual in that the pain only occurred after activity such as playing soccer or cheerleading and resolved after 24-48 hours.
One issue commonly encountered with individuals enduring VND pain is an incorrect initial diagnosis. These misdiagnoses result in delayed care, extending the duration of pain suffered by children with VND. VND frequently presents similarly and initially may be misinterpreted as other pathologies, including stress fractures, bone tumors, osteomyelitis, and post-traumatic osteolysis [12]. In this systematic review of the literature, 11 of the 19 patients were initially misdiagnosed with a wide array of pathologies, as previously mentioned, with stress, subacute, or pathological fractures being the most common. Stress fractures can be differentiated on MRI, which shows an irregular fracture line [19]. Avulsion fractures occur acutely during activity and present as pain and difficulty jumping and displacement of the fracture and muscle edema on MRI [17]. Additional differential diagnoses included slipped capital femoral epiphysis, fibrous dysplasia, eosinophilic granulomas, and bone cysts. Malignant neoplasms would show bone marrow, irregular bone cortex, and surrounding tissue edema early and abscess formation on MRI as a late finding in osteosarcoma or Ewing’s sarcoma. Enthesitis-related juvenile idiopathic arthritis would present as enthesitis and arthritis, along with sacroiliac pain, positive laboratory testing, other autoimmune conditions, or a family history of autoimmune conditions [5]. Two patients were given the diagnosis of VND and were not initially misdiagnosed, while there were six without any listed differentials mentioned on presentation.
An additional consideration for the resolution of VND in the pediatric population is the activity levels of the patient with VND before diagnosis. Research shows adequate activity levels are important not only for managing chronic diseases, preventing disease, and preventing premature death, but activity is extremely important for overcoming acute illness [24]. Of the patients included in this study, eight were athletes and participated in activities, including futsal, football, dancing, soccer, and cheerleading. Of these eight, six were found to have complete resolution of symptoms upon their initial follow-up visit. One athlete at eight weeks had minimal improvement, and with prescribed rehabilitation, had improvement of symptoms [16]. The other patient was found to have an increasing size of their lesion, and with continued therapy and rehabilitation, was able to succeed in activities of daily living at six months and returned to sporting events after one year [19]. Comparing athletes versus non-athletes, there was no uniform follow-up time among patients. Follow-up times ranged from 48 hours and two weeks on the shorter end up to six months.
While most patients achieved full recovery after initial treatment, one case involved a six-year-old boy diagnosed with VND and treated with relative rest, suspension of sports practice for six weeks, moderation in running activities, and follow-up at eight weeks [16]. The patient, despite recommendations, resumed futsal practice two weeks after the diagnosis with no change in training intensity. This led to symptom recurrence and impairment. On follow-up, the patient still reported groin pain and a slight limp, and a rehabilitation program was recommended. Following rehabilitation, re-evaluation after six months showed a complete resolution of symptoms and gait improvement.
Limitations
This study was not without limitations. In this systematic review, only English-language publications were included. Therefore, some of the earlier texts regarding this disease process were excluded. Additionally, the data provided across all studies were not homogeneous. However, all available data were extracted from the studies to provide readers with the most comprehensive overview of VND to date. Lastly, due to the limitation of including English-only studies, there may be several relevant cases omitted, particularly from Europe or Asia.
Conclusions
VND, or IPS, is a rare and difficult-to-diagnose pediatric condition due to its nonspecific presentation. Common differential diagnoses include fractures, osteomyelitis, benign or malignant tumors, slipped capital femoral epiphysis, and autoimmune disorders. Recognizing the clinical characteristics of VND, such as its associated imaging, physical examination findings, and laboratory findings, can help make an accurate diagnosis and prevent delayed treatments. It is particularly important when conducting the clinical work-up for older pediatric individuals to always keep VND in the differential when similar nonspecific symptoms are present to prevent longer recovery times in this demographic. Even though this pathology is treated with conservative management and typically has a good prognosis, making the correct initial diagnosis is imperative to preventing unnecessary invasive management. Understanding the anatomy and physiology of this normal, temporary joint and being able to recognize common diagnostic features will allow physicians to accurately identify this disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van Neck-Odelberg disease: a 3.5-year follow-up case report and systematic review Surg Technol Int Mixa PJ Segreto FA Luigi-Martinez H Diebo BG Naziri Q Kolla S Maheshwari AV 365373312017 https://pubmed.ncbi.nlm.nih.gov/29316596/29316596 · pubmed ↗
- 2Some cases of destruction in the ischium of doubtful etiology Acta Chir Scand Odelberg A 273284561923 https://numerabilis.u-paris.fr/ressources/pdf/medica/bibnum/epo 0962/epo 0962.pdf
- 3Osteochondrite du pubis Arch Franco-Belg Chir Van Neck M 238240271924
- 4A rare disease of the pediatric pelvis: Van Neck-Odelberg disease JDRS Case Rep Korkmazer S Yigit Kaptan A Kagan Eren T 151812022
- 5Osteochondrosis of ischiopubic synchondrosis: van Neck-Odelberg disease J Pediatr Sabir N Çakmak P Yılmaz N Yüksel S 30730822920213294184310.1016/j.jpeds.2020.09.027 · doi ↗ · pubmed ↗
- 6Van Neck-Odelberg disease: a rare case report J Orthop Case Rep Chaudhari AP Shah G Patil SS Ghodke AB Kelkar SB 24277201710.13107/jocr.2250-0685.672PMC 545869128630834 · doi ↗ · pubmed ↗
- 7Van neck disease: osteochondrosis of the ischiopubic synchondrosis J Pediatr Orthop Wait A Gaskill T Sarwar Z Busch M 5205243120112165445910.1097/BPO.0b 013e 31821 f 9040 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗