A Vanishing Polyp: A Large Ileal Lipoma Causing Ileocolic Intussusception
Chiaw Yuan Tan, Kosasih Sumitro, Amy Thien, Kian Chai Lim, Aye Aye Tun, Vui H Chong

TL;DR
A 55-year-old man had a large lipoma in his ileum that caused intussusception, a rare condition where part of the intestine folds into another part.
Contribution
This case uniquely describes an ileal lipoma causing intussusception observed and reduced during colonoscopy.
Findings
A large ileal lipoma was identified as the cause of ileocolic intussusception in an adult.
The intussusception was observed and reduced during colonoscopy, a unique clinical observation.
Histology confirmed the lesion as a submucosal lipoma, a rare cause of intussusception in adults.
Abstract
Intussusception is defined as invagination of a proximal segment of gastrointestinal tract into distal segment and is an uncommon pathology. It is more common in children. In the adult population, it is often due to a polyp or tumor. We report an interesting case of a vanishing colonic polyp in a 55-year-old man who presented with a three-month history of intermittent right abdominal pain, altered bowel habit, and weight loss. Colonoscopy demonstrated a large, elongated polyp in the ascending colon, which vanished during attempts to intubate proximally. A computed tomography scan showed a lipomatous polyp in the distal ileum confirmed on a repeat colonoscopy. The patient proceeded with surgical resection, and histology confirmed the polyp to be an ileal submucosal lipoma. There is literature on ileocolic intussusceptions secondary to ileal submucosal lipoma; however, our case is…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
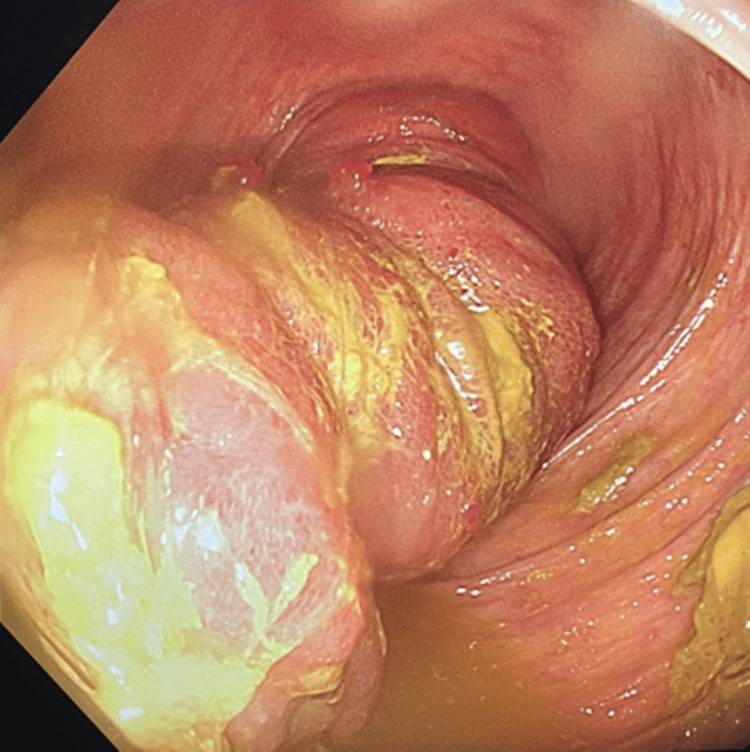 Figure 1
Figure 1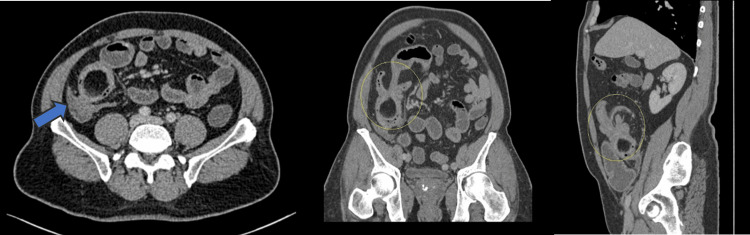 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment
Introduction
Intussusception is generally uncommon and is reported more in the pediatric population. In the adult population, intussusception accounts for up to 1% of intestinal obstruction, and carcinoma and polyps are identified during perioperative as the lead point of intussusception in at least 90% of cases [1]. Small bowel lipomas, which are typically benign, are mostly located at the distal ileum and are submucosal mesenchymal tumors. They are usually asymptomatic, but lesions that are ≥ 2 cm may cause nonspecific symptoms, such as abdominal pain, diarrhea, bleeding, and obstruction [2]. We report an interesting case of a vanishing elongated polyp in the proximal colon encountered during colonoscopy, which was later found to be due to an ileal lipoma that intussuscepted. He was successfully treated with surgical resection.
Case presentation
A 55-year-old man presented without any significant past medical history with intermittent right abdominal pain that radiates to the right flank, altered bowel habit, and weight loss of up to 10 kg over a month's duration. This was interposed with a period of no symptoms until they reoccurred suddenly. He denies experiencing any upper gastrointestinal (GI) symptoms, abdominal distention, fever, or any bleeding, altered blood, or fresh bleeding. There was no family history of GI malignancy, and he was a non-smoker. Abdominal examination revealed mild mid-abdominal tenderness but without any mass. Per rectal examination showed no mass and normal stool. Initial laboratory investigation revealed iron deficiency anemia with a level of 8.1 gr/dL (normal > 13 gr/dL), ferritin 10 ng/mL (normal: 30-400 ng/mL); otherwise, renal and liver function and inflammatory markers were unremarkable.
In view of the symptoms and anemia, GI neoplasm was suspected. He underwent bidirectional endoscopies. Upper GI endoscopy showed only gastritis, and testing was negative for Helicobacter pylori infection. Colonoscopy interestingly showed a large, elongated polyp in the proximal colon (Figure 1) on initial intubation. It was not possible to visualize the ileocecal valve and the cecum. Interestingly, while inspecting the ascending colon and during withdrawal of the endoscope, the polyp became smaller and suddenly vanished.
A colonoscopy view in the ascending colon showing a large, elongated polyp.
The patient remained stable and proceeded with a computed tomography (CT) scan of the abdomen and pelvis. This showed a fat density round mass in the ileum and invagination of the ileal loops in the distal ileum, proximal-to-ileocecal valve, with mild proximal small bowel dilation (Figure 2).
Axial (left), coronal oblique (middle), and sagittal (right) contrast-enhanced CT images showing a round fat-density mass in the distal ileum, with invagination of the ileum and resultant proximal small bowel distension, due to intussusception of ileal lipoma.
The patient was referred to the surgical department; as his symptoms settled with the spontaneous resolution of the intussusception, the patient was discharged for follow-up. A repeat colonoscopy done two weeks later showed a patulous ileocecal valve, and assessment of the terminal ileum revealed a large polypoidal lesion with friable mucosal surface located at ~15 cm from the ileocecal valve (Figure 3).
A repeat colonoscopy with ileoscopy showing the polyp with a friable mucosa.
The patient subsequently underwent surgical resection with primary anastomosis. Intraoperative findings confirmed a 5 x 4 cm mass, located 15 cm from the ileocecal junction (Figure 4). Histopathology findings confirmed the mass to be a lipoma.
Intraoperative and post-resection images of the pathology.
He recovered well post-operatively without further bowel symptoms, and his hemoglobin level normalized after four months post-surgery.
Discussion
We report an interesting case of a vanishing polyp in the ascending colon due to ileo-colic intussusception with a large ileal submucosal lipoma as the leading point. The initial polyp encountered was unusual as it was long and tubular with a very thick stalk. Interestingly, with attempts to get beyond the polyp, the intussusception was inadvertently reduced - the polyp had vanished. Air insufflation and scope manipulations led to the reduction of the intussusceptions, principles used for the management of intussusception - contrast reduction. It was only after the polyp had vanished with a resultant patulous ileocecal valve that intussusception was suspected. There are numerous reports of ileocolic intussusceptions secondary to ileal submucosal lipoma reported in the literature [3,4]. However, our case is interesting in that the intussusception was seen and reduced during the colonoscopy. A lesson from this case is to consider an intussusception when a long tubular polyp is encountered in colonoscopy.
Intussusceptions can be considered uncommon and can be classified according to their location: entero-enteric, ileo-cecal, ileo-colic, and colo-colic, with ileo-colic intussusception being the most common. The most common cause of intussusception in adults is a malignant lesion (65%-75%), followed by a benign lesion such as lipoma, polyp, or lymphangioma (15-20%) [5].
GI lipomas are the second most common type of benign GI neoplasm, followed by adenomas. It is most frequently found between 50 and 70 years old, with an incidence ranging between 0.15% and 4.4%, more commonly in the colon. A vast majority (90-95%) are sub-mucosal, only a small percentage sub-serosal, and can be sessile or pedunculated [2,6]. Colonic lipoma mainly right-sided colon is the most common location, followed by the small intestine (mainly ileal), stomach, and oesophagus [1,7].
Most lipomas are asymptomatic and are found incidentally during endoscopic examination. Typically, these lesions are small. The larger the lipoma, the more likely it is to cause symptoms such as nonspecific abdominal pain, colic, and bowel obstruction, which can be intermittent due to obstruction or intussusception. Large lipomas are more likely to cause intussusception as they can form a leading point. There has also been a case reported for colonic lipoma that had caused intussusception and prolapse out of the rectum.
GI submucosal lipomas larger than 2 cm may develop mucosal ulceration and can present with iron deficiency anaemia [7,8]. As in our case, the patient presented with non-specific abdominal pain with iron deficiency anemia, and no overt GI bleeding. With these symptoms, GI lipoma is diagnosed by barium enema, abdominal CT, or colonoscopy.
Lipoma is managed according to size and symptoms. Small submucosal lipomas not big enough to cause lumen compromise and symptoms are typically left behind and do not require surveillance. Large lipomas can be resected endoscopically, depending on the side and presence of a stalk. However, lipomas larger than 5 cm, as in our case, may act as a leading point for intussusception, causing subacute small bowel obstruction, and surgical intervention is often required. For cases presenting with intussusception, management can be non-surgical at the initial presentation. More commonly reported in the paediatric population, barium enema or air insufflation is often first-line management of intussusception [9,10]. For those with polyps or tumors as leading points, surgery is often required.
Conclusions
Although lipomas are mostly asymptomatic, but, if large, they may act as a leading point for intussusception in the GI tract; ulceration may also occur, leading to iron deficiency anemia. In cases where a small bowel lipoma becomes symptomatic, resection is the preferred treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Submucosal lipoma: a rare cause of recurrent intestinal obstruction and intestinal intussusception J Gastrointest Surg Jiang RD Zhi XT Zhang B Chen ZQ Li T 173317351920152589598010.1007/s 11605-015-2824-1 · doi ↗ · pubmed ↗
- 2Imaging and findings of lipomas of the gastrointestinal tract AJR Am J Roentgenol Thompson WM 1163117118420051578858810.2214/ajr.184.4.01841163 · doi ↗ · pubmed ↗
- 3Terminal ileum lipoma causing ileocolic intussusception: a case report and literature review Cureus Dogra S Wei J Wadowski B Devi-Chou V Krowsoski L Shah RR 015202310.7759/cureus.49562 PMC 1075402738156183 · doi ↗ · pubmed ↗
- 4Ileocolic intussusception caused by giant submucosal colonic lipoma: a rare case report Int J Surg Case Rep Park N Kuk JC Shin EJ Chin SS Lim DR 1074519720223593271210.1016/j.ijscr.2022.107451 PMC 9403280 · doi ↗ · pubmed ↗
- 5Adult colocolic intussusception and literature review Case Rep Gastroenterol Wilson A Elias G Dupiton R 381387720132416364910.1159/000355155 PMC 3806710 · doi ↗ · pubmed ↗
- 6Gastrointestinal lipomas: a radiologic and pathologic review AJR Am J Roentgenol Taylor AJ Stewart ET Dodds WJ 120512101551990212266610.2214/ajr.155.6.2122666 · doi ↗ · pubmed ↗
- 7Adult ileocolic intussusception secondary to cecal lipoma: a case report Cureus Angelakakis G Fish S Katz KD 016202410.7759/cureus.59986 PMC 1116226938854263 · doi ↗ · pubmed ↗
- 8Colo-colonic intussusception due to large submucous lipoma: a case report Int J Surg Case Rep de Figueiredo LO Garcia DP Alberti LR Paiva RA Petroianu A Paolucci LB Costa MR 1071102820162769386910.1016/j.ijscr.2016.09.006PMC 5048079 · doi ↗ · pubmed ↗