Managing Psychosis in Acute Intermittent Porphyria: A Case Report on Olanzapine Use
Chwee Fern Ooi, Chao Tian Tang, Sing Qin Ting, Iris Rawtaer, Ho Teck Tan

TL;DR
A case report shows olanzapine effectively treated psychosis in a patient with acute intermittent porphyria, highlighting the need for early diagnosis and careful monitoring.
Contribution
Demonstrates olanzapine's safety and efficacy in treating AIP-related psychosis, offering clinical guidance for similar cases.
Findings
Psychotic symptoms in AIP resolved completely with olanzapine within eight days.
Olanzapine showed no adverse effects in treating AIP-related psychosis.
Early recognition of AIP in psychiatric presentations can prevent diagnostic delays.
Abstract
Acute intermittent porphyria (AIP) is the most common type of acute porphyria, caused by reduced porphobilinogen deaminase activity, leading to accumulations of neurotoxic compounds. Symptoms usually include abdominal pain, autonomic dysfunction, neurological involvement, and psychiatric symptoms. Neuropsychiatric symptoms such as psychosis are common and may contribute to diagnostic delays. We report a case of a middle-aged woman presenting with psychiatric and neurovisceral symptoms of AIP. This report discusses the case of a 41-year-old woman with no prior psychiatric history presenting with an acute onset of psychotic symptoms, including persecutory, erotomanic, and Capgras delusions, disorganized behavior, and agitation, along with physical symptoms of acute abdominal pain and autonomic disturbances. An extensive organic workup revealed elevated urinary porphobilinogen, which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
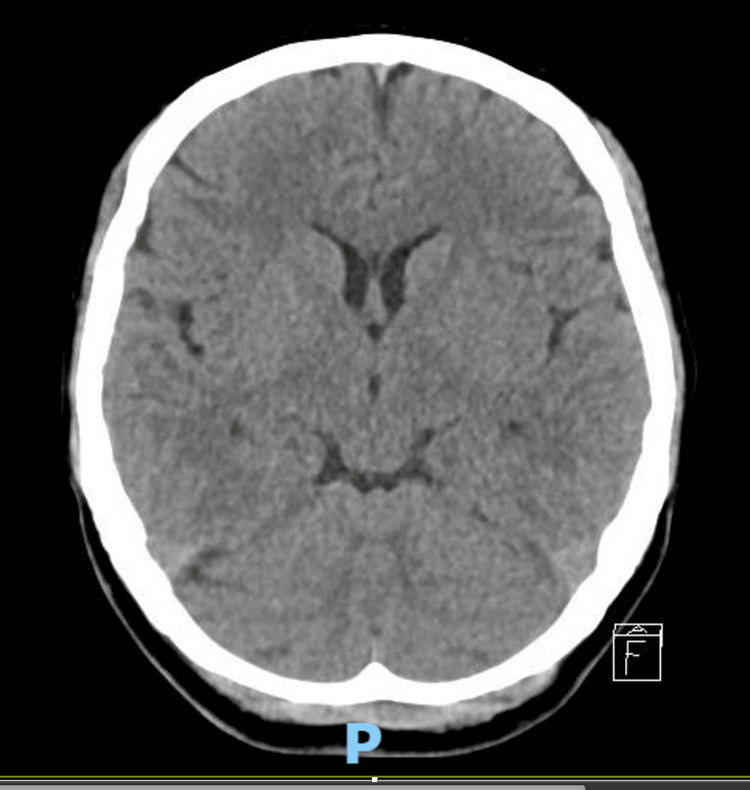 Figure 1
Figure 1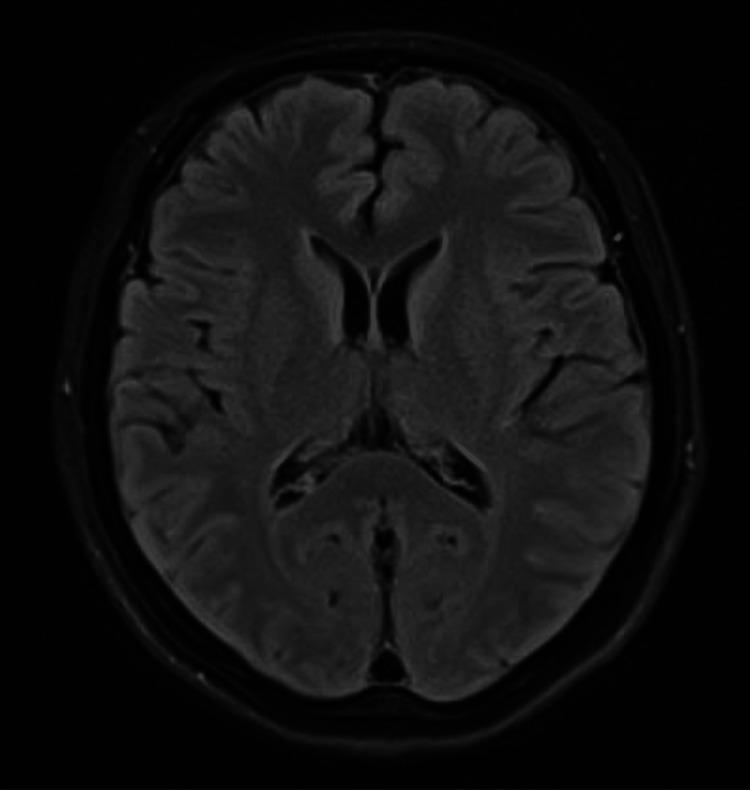 Figure 2
Figure 2| Parameters | Result | Reference range |
| Hemoglobin | 13.3 | 12-16 g/dL |
| WBC count | 7.99 | 4-10 × 109/L |
| Platelet count | 304 | 140-440 × 109/L |
| Urea | 3.3 | 2.5-7.8 mmol/L |
| Sodium | 138 | 133-146 mmol/L |
| Potassium | 4.0 | 3.5-5.1 mmol/L |
| Creatinine | 44 | 45-84 umol/L |
| Glucose | 5.9 | 3.9-11.0 mmol/L |
| Magnesium | 0.87 | 0.7-1.0 mmol/L |
| Corrected calcium | 2.18 | 2.1-2.6 mmol/L |
| Inorganic phosphate | 1.30 | 0.8-1.5 mmol/L |
| Free T4 | 17.8 | 11.9-21.6 pmol/L |
| Thyroid-stimulating hormone | 2.05 | 0.270-4.200 mIU/L |
| Total protein | 61 | 68-85 g/L |
| Albumin | 40 | 35-50 g/L |
| Total bilirubin | 9 | ≤21 umol/L |
| Alkaline phosphatase | 51 | 35-104 U/L |
| Alanine transaminase | 21 | ≤35 umol/L |
| Aspartate transaminase | 21 | ≤35 umol/L |
| Beta-hCG | <0.6 | ≤5.0 IU/L: nonpregnant |
| Lactate | 0.9 | 0.5-2.2 mmol/L |
| Ammonia | 14 | 1.6-53 umol/L |
| C-reactive protein | <0.6 | ≤4.9 mg/L |
| HIV | Nonreactive | Nonreactive |
| VDRL (syphilis) | Nonreactive | Nonreactive |
| Opioids | Negative | Negative |
| Tricyclic antidepressants | Negative | Negative |
| Amphetamine | Negative | Negative |
| Methamphetamine | Negative | Negative |
| Ketamine | Negative | Negative |
| MDMA | Negative | Negative |
| LSD | Negative | Negative |
| Parameter | Results | Reference range |
| Glucose | Negative | Negative |
| Ketones | 1+ | Negative |
| RBC | 25 | 0-3/uL |
| WBC | 5 | 0-6/uL |
| Epithelial cells | 0 | 0-4/uL |
| Cast, crystals, microorganisms | Negative | Negative |
| Bilirubin | Negative | Negative |
| Specific gravity | 1.015 | 1.02-1.035 |
| pH | 6.5 | 4.6-8.0 |
| Protein | Negative | Negative |
| Urobilinogen | 1.0 | 0.2-1.0 EU/dL |
| Nitrite, leucocytes | Negative | Negative |
| Parameter | Results | Reference range |
| Appearance | Colorless | Colorless |
| WBC count | 0 | 0-5/uL |
| RBC count | 0 | 0-5/uL |
| Glucose | 3.2 | 2.2-3.9 mmol/L |
| Total protein | 0.35 | 0.15-0.45 g/L |
| Cytology, culture | Negative | Negative |
| AFB, TB tests | Negative | Negative |
| Meningitis/encephalitis PCR | Negative | Negative |
| Antibody tests | Result |
| NMDAR | Negative |
| CASPR2 | Negative |
| AMPAR1/2 | Negative |
| LGI1 | Negative |
| DPPX/DPP6 | Negative |
| GABABR | Negative |
| Antibodies tested | Result |
| Amphiphysin | Negative |
| CV2/CRMP5 | Negative |
| PNMA2/Ta | Negative |
| Ri (ANNA-2) | Negative |
| Yo (PCA-1) | Negative |
| Hu (ANNA-1) | Negative |
| Recoverin | Negative |
| SOX1 | Negative |
| Titin | Negative |
| Zic4 | Negative |
| GAD65 | Negative |
| Tr (DNER) | Negative |
| Parameters | Results | Reference range |
| Antineutrophil cytoplasmic antibody (IIF) | Negative | Negative |
| Anti-double-stranded DNA antibody | <0.6 | <10 IU/mL: negative |
| Smith antibody, ribonucleoprotein antibody, Ro (SSA) antibody, La (SSB) antibody, Scl 70 antibody, Jo-1 antibody | <1.0 | <1.0: negative |
| Urine porphobilinogen | Positive | Negative |
| Study | Treatment | Outcome | Side effects |
|
Holroyd and Seward [ | Olanzapine, trifluoperazine, and risperidone | Poor response | Trifluoperazine: drug-induced Parkinsonism |
|
Bautista et al. [ | Olanzapine, aripiprazole, and clozapine | Poor response | Aripiprazole: akathisia olanzapine: muscle cramping |
|
Horgan and Jones [ | Olanzapine | Good response | Elevated liver enzymes (ALT/AST) |
|
Strauss and DiMartini [ | Olanzapine | Good response | None reported |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPorphyrin Metabolism and Disorders · Folate and B Vitamins Research · Heme Oxygenase-1 and Carbon Monoxide
Introduction
Acute porphyrias are a rare group of metabolic disorders caused by enzymatic defects in the heme biosynthesis pathway, resulting in toxic metabolite buildup [1,2]. Acute intermittent porphyria (AIP) is the most common form of acute porphyria, with a prevalence of five to ten individuals per 100,000 [3] and one in 2,000 across Europe. However, in Sweden, the incidence is higher, affecting approximately one in 1,000 individuals due to the founder effect [4].
AIP is inherited in an autosomal dominant pattern with variable expressivity and results from mutations that decrease the activity of porphobilinogen deaminase, also known as hydroxymethylbilane synthase. This enzyme deficiency leads to the accumulation of toxic compounds such as porphobilinogen (PBG) and δ-aminolevulinic acid (ALA), which causes neurological damage [2,5], manifesting as peripheral or autonomic neuropathies and psychiatric manifestations [6].
AIP manifests with a broad range of symptoms, often causing diagnostic delays [7]. It disproportionately affects women, with a female-to-male ratio of 1.5 to 2:1, and typically manifests between ages 18 and 40 [6].
This report presents a case of AIP with acute neurovisceral and psychiatric manifestations. Notably, the patient responded well to olanzapine, achieving rapid symptom resolution without signs of liver dysfunction, highlighting a potential role for this atypical antipsychotic in managing AIP-associated psychosis.
Case presentation
A 41-year-old Chinese woman with no prior medical or psychiatric history presented with a one-week history of abrupt behavioral changes. She presented with persecutory, erotomanic, and Capgras delusions involving her parents. She believed that her colleagues and parents were trying to harm her and was convinced that she was in a romantic relationship with a male colleague. Additionally, she held the fixed belief that her parents were not her biological parents and had been replaced by impostors. She denied experiencing auditory or visual hallucinations, thought interference, or passivity symptoms. There was no significant decline in her daily functioning; she worked as an engineer and had been performing well at work before symptom onset. These psychiatric issues were preceded by transient, nonspecific abdominal pain several months earlier, which had resolved spontaneously.
The patient was born in China and relocated to Singapore in her 20s. She reported no family history of mental illness but described childhood adversity, including physical punishment by her mother at the age of seven due to academic difficulties. She denied alcohol or substance use, recent lifestyle changes, significant psychosocial stressors, or any dietary modification, such as dieting or reduced carbohydrate intake, before the onset of her illness. Her premorbid personality was described as introverted and calm. There was no family history of autoimmune diseases.
During hospitalization, she developed recurrent abdominal pain and fever. Her paranoia intensified, leading to her food refusal. She became increasingly restless, disorganized, and irritable, resulting in episodes of agitation, during which she attempted to dash out of her ward cubicle and climb out of bed. These behaviors necessitated the use of rapid tranquillization (oral and intramuscular lorazepam) and brief physical restraints to ensure her safety and that of others.
Physical examination revealed no overt neurological deficits or other abnormalities. However, she had episodes of low-grade fever (ranging from 37.6°C to 37.9°C) and tachycardia (up to 114 bpm) but no hypertension.
Given the acute onset of psychotic symptoms alongside physical and autonomic disturbances with tachycardia and fever, exclusion of organic causes was prioritized. Brief psychotic disorder was considered in the differential diagnosis based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria, given the presence of delusions and disorganized behavior lasting more than one day but less than a month (approximately one week for this case). The diagnosis was further supported by the absence of mood symptoms or substance use. However, investigations for underlying medical conditions were still ongoing at that time.
Basic laboratory tests, including complete blood count, renal and liver function, thyroid and pregnancy tests, infectious screening, and urinalysis, showed no significant abnormalities or evidence of infection (Tables 1, 2). The toxicology screen was negative (Table 1). Brain imaging studies, including both a computed tomography scan (Figure 1) and a contrast-enhanced magnetic resonance imaging (Figure 2), were unremarkable. An EEG showed normal findings. Additionally, a lumbar puncture was performed, revealing normal cerebrospinal fluid analysis (Table 3). Tests for paraneoplastic antibodies, autoimmune encephalitis, and autoimmune panel were also negative (Tables 4-6).
Noncontrasted CT brain revealed no evidence of acute intracranial abnormalities such as infarct, hemorrhage, or mass effect. The ventricular system appeared normal in size and configurationCT: computed tomography
Contrasted MRI brain showed no evidence of intracranial pathology, such as infarct, hemorrhage, mass lesion, or parenchymal enhancing lesion. The ventricles, sulci, and cisterns are age-appropriate in size and configuration. The basal cisterns are preservedMRI: magnetic resonance imaging
The neurology team was consulted and recommended a thorough organic workup, including urine PBG testing as part of a broader workup for unexplained autonomic and abdominal symptoms, given clinical suspicion of a metabolic etiology such as AIP. This test subsequently yielded a positive result (Table 6).
Treatment was initiated with olanzapine orodispersible tablets at 5 mg nightly on the sixth day of admission due to persistent psychotic symptoms, prior to confirmation of a porphyria diagnosis. Within three days, the patient exhibited clinical improvement, becoming calmer, less confused, and more communicative.
Urine PBG testing was performed on the seventh day of admission, and a positive result was received on the 11th day of admission, confirming a diagnosis of AIP with neurovisceral and neuropsychiatric symptoms. In response, the hematologist recommended two days of intravenous dextrose saline, which was initiated on the same day. Concurrently, the patient was referred to a dietitian for carbohydrate loading. As she continued to improve with existing psychiatric and medical treatment, intravenous hemin was not administered. She was advised to avoid alcohol and hormonal medications, and genetic counseling was provided to her parents.
The dose of olanzapine was gradually increased to 10 mg nightly. By the 13th day of admission (the eighth day of antipsychotic treatment), she achieved complete resolution of psychotic symptoms. Her family noted a return to her baseline personality. Liver function tests were checked twice during treatment and remained normal throughout.
A follow-up urine porphyrin test on October 3, 2024, was normal. At discharge, she reported no residual psychotic symptoms and was discharged into the care of her family. Follow-up appointments with psychiatry and hematology were scheduled for ongoing monitoring.
Discussion
Acute AIP attacks are typically triggered by factors such as medications, infections, alcohol use, steroid hormones, and dietary factors such as fasting or reduced carbohydrate intake. AIP affects women more frequently than men. Symptoms typically manifest postpuberty, between the ages of 18 and 40 years [6]. Sex hormones like estrogen and progesterone are thought to increase ALA synthase activity, leading to a rise in porphyrin precursors [8]. Notably, these findings align with our case, as the patient is a woman within the expected age range.
Acute attacks typically present with severe abdominal pain, gastrointestinal symptoms (nausea and constipation), autonomic dysfunction (palpitations, tachycardia, sweating, and hypertension), and neurological manifestations such as confusion, peripheral neuropathy, paresis, or seizure [7]. Acute abdominal pain is the most common cause of admission in acute porphyria [9]. Patients may also report urine darkening to a reddish hue, especially upon light exposure [1]. Similarly, our patient experienced transient, nonspecific abdominal pain before presentation, a common initial symptom, accompanied by tachycardia and hypertension.
Psychiatric manifestations occur in 24%-80% of AIP cases. Psychiatric symptoms such as psychosis, anxiety, depression, and agitation further complicate diagnosis [1,10]. Depression and delirium were the most frequent neuropsychiatric manifestations [11]. In our case report, our patient presented with psychosis (with persecutory, erotomanic, and Capgras delusions) with episodes of agitation, which is in line with the common psychiatric manifestations of AIP.
According to the drugs safe list produced by Welsh Medicines Information Centre and Cardiff Porphyria Service in 2014 [12] and is supported by the National Acute Porphyria Service, the antipsychotics that are considered to be safe for use in the acute porphyria are haloperidol, chlorpromazine, fluphenazine trifluoperazine, amisulpiride, sulpiride, clozapine, and olanzapine. Meanwhile, chlorpromazine and trifluoperazine are typically recommended for use in porphyria, holding the longest record of safe use in this illness (Table 7).
The variability in response to antipsychotics in AIP remains an area of clinical uncertainty, with reported cases demonstrating mixed efficacy. Olanzapine, which was effective in our patient, has previously been associated with positive outcomes [15,16] but has also been linked with liver enzyme elevation [15] and poor symptom control [13,14]. One possible explanation is variability in drug metabolism, as olanzapine is primarily metabolized by CYP1A2 and CYP2D6 [17], enzymes that may be impacted by hepatic dysfunction in AIP. Patients with altered CYP1A2 activity may experience reduced clearance of olanzapine, leading to increased side effects or treatment failure.
In our case report, olanzapine was chosen for its efficacy in treating positive symptoms, favorable tolerability, and low risk of extrapyramidal side effects. It was also considered appropriate given the absence of preexisting metabolic conditions in this patient. While olanzapine is associated with potential metabolic side effects such as weight gain and impaired glucose tolerance [18], the patient did not exhibit any metabolic derangements during the course of treatment. The patient showed rapid improvement in the resolution of psychotic symptoms within eight days of psychiatric treatment. In contrast to the case reported by Horgan and Jones, our patient has shown stability in liver enzymes after treatment, providing further evidence for the safe use of olanzapine in acute porphyria.
Given the limited evidence and mixed reported case outcomes, careful selection of antipsychotics in AIP should consider both efficacy and safety. While olanzapine was well-tolerated in our case, clinicians should monitor for hepatic effects and treatment response on an individual basis. Future studies should investigate the role of CYP polymorphisms and receptor-binding properties in antipsychotic selection for AIP-associated psychosis.
This case highlights the complexity of managing psychiatric symptoms in AIP and emphasizes the importance of early recognition of symptoms and individualized treatment strategies. The decision to test for urinary PBG was crucial in clinching the diagnosis, particularly as AIP often presents with a mix of psychiatric and neurovisceral symptoms that can mimic primary psychiatric disorders. In patients presenting with acute psychosis alongside abdominal pain or autonomic instability, screening for porphyria, especially AIP, should be part of the differential workup. While olanzapine demonstrated good efficacy and tolerability in this patient, variability in drug response remains a challenge. Future research should focus on refining antipsychotic selection based on pharmacogenetic factors and long-term safety data. These insights are essential for developing standardized guidelines for the treatment of AIP-related neuropsychiatric manifestations.
Conclusions
This case highlights the diagnostic and therapeutic challenges of neuropsychiatric symptoms in AIP. It was essential to consider AIP in patients with acute psychosis and coexisting autonomic or visceral symptoms. Prompt urine PBG can aid early diagnosis and appropriate management, potentially averting complications and reducing diagnostic delay. The patient’s positive response to olanzapine supports its potential safety and efficacy in AIP-associated psychosis. However, given mixed responses and reports of hepatic adverse effects in other cases, clinicians should monitor liver function closely when prescribing olanzapine for AIP. Further research is needed to establish standardized treatment guidelines, assess long-term safety, and investigate the role of genetic factors (e.g., CYP enzyme polymorphisms) in antipsychotic metabolism and efficacy in AIP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute Porphyria 3 2025 Gounden V Jialal I Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 537352/30726037 · pubmed ↗
- 2A case report of acute intermittent porphyria leading to severe disability Front Neurol Lin J Liu J Wang A Si Z 13347431420233827488310.3389/fneur.2023.1334743 PMC 10808997 · doi ↗ · pubmed ↗
- 3Acute hepatic porphyria J Clin Transl Hepatol Bissell DM Wang B 1726320152635763110.14218/JCTH.2014.00039 PMC 4542079 · doi ↗ · pubmed ↗
- 4Acute intermittent porphyria's symptoms and management: a narrative review Cureus Kizilaslan EZ Ghadge NM Martinez A 015202310.7759/cureus.36058 PMC 1009675137065381 · doi ↗ · pubmed ↗
- 5Acute intermittent porphyria: current perspectives and case presentation Ther Clin Risk Manag Spiritos Z Salvador S Mosquera D Wilder J 144314511520193190846410.2147/TCRM.S 180161 PMC 6930514 · doi ↗ · pubmed ↗
- 6Acute Intermittent Porphyria Gonzalez-Mosquera LF Sonthalia S Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 547665/31613445 · pubmed ↗
- 7Acute hepatic porphyrias: recommendations for evaluation and long-term management Hepatology Balwani M Wang B Anderson KE 131413226620172860504010.1002/hep.29313 PMC 5605422 · doi ↗ · pubmed ↗
- 8Acute intermittent porphyria in women: clinical expression, use and experience of exogenous sex hormones. A population-based study in northern Sweden J Intern Med Andersson C Innala E Bäckström T 17618325420031285969910.1046/j.1365-2796.2003.01172.x · doi ↗ · pubmed ↗