Post‐Axial Polydactyly and Postnatal Pulmonary Stenosis Observed With a SPRED1 Pathogenic Variant
Alexander Gibbs, Muriel Holder‐Espinasse, Vijaya Ramachandran, Natalie J. Chandler

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
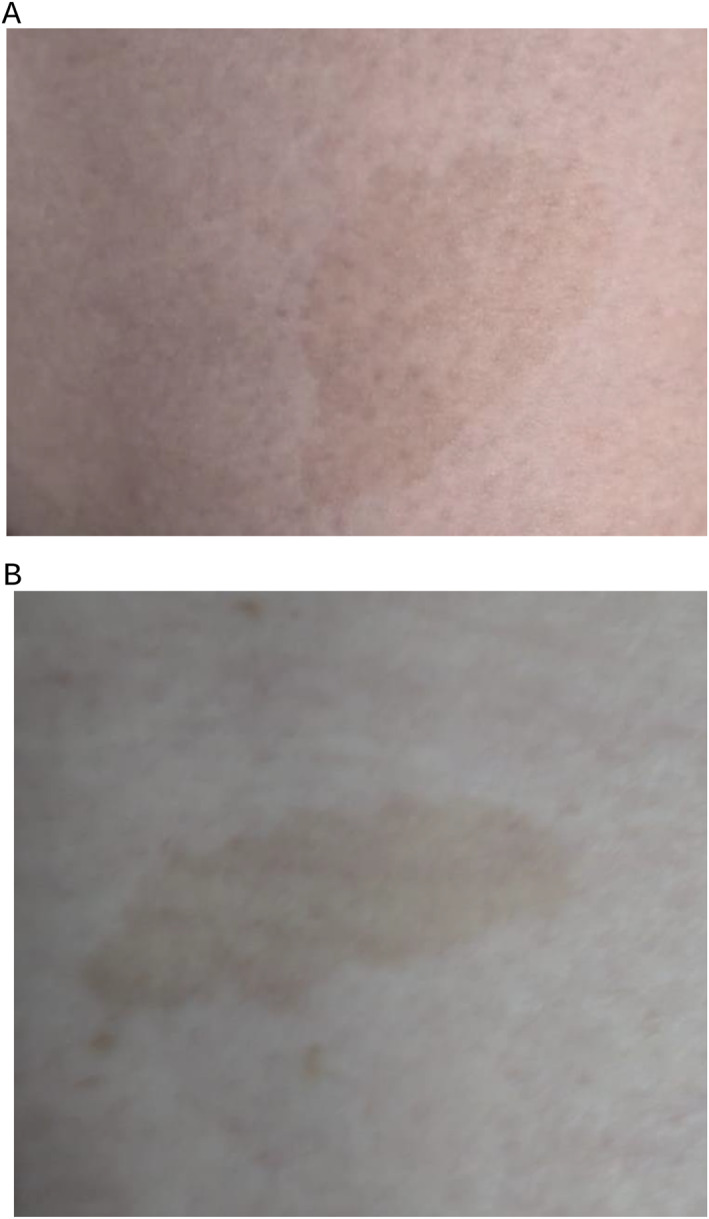 FIGURE 1
FIGURE 1| Case | Parental details | Gestation at diagnosis | Phenotypes (HPO terms) | Obstetric history | Family history | Outcome | ||
|---|---|---|---|---|---|---|---|---|
| 1 | Maternal | Age | 37 | 29 + 3 |
Polydactyly (HP: 0010442) Valvular pulmonary stenosis (HP:0034350) | Pre‐eclampsia | Undiagnosed skin pigmentation disorder | Delivery at 32 + 4 WG via Caesarean section |
| Ethnicity | White British | |||||||
| Paternal | Age | 39 | ||||||
| Ethnicity | White British | |||||||
| Procedure (gest age) | Direct/culture? | Performed test | Secondary confirmatory test | Gene (name; REFSEQ) | Known disease (OMIM) | Variant | ACMG classification | Criteria applied | Inheritance & zygosity | Interpretation |
|---|---|---|---|---|---|---|---|---|---|---|
| 29 + 3 | Direct | Trio exome. Fetal anomalies panel applied | Sanger sequencing |
| Legius syndrome (611431) | c.1149_1152delp | 4 |
| AD, maternal | Consistent with diagnosis |
| (Gly385IlefsTer20) | ||||||||||
| Heterozygous |
- —NIHR Biomedical Research Center at Great Ormond Street Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Connective tissue disorders research · Cancer and Skin Lesions
Summary
- What's already known about this topic?
- ◦Heterozygous variants in SPRED1 are associated with Legius syndrome, characterized by multiple cafe‐au‐lait spots and variable dysmorphic features.
- ◦Post‐axial polydactyly is a rarely reported feature and cardiac abnormalities are not currently known to be associated with Legius syndrome.
- What does this study add?
- ◦Further weight to the association between post‐axial polydactyly and Legius syndrome.
- ◦Further evidence that a postnatal diagnosis of pulmonary stenosis is in keeping with Legius syndrome.
Introduction
1
A White British couple spontaneously conceived their first pregnancy. The female partner reported no medical history. However, her brother and mother (who had died of pancreatic cancer) both had abnormal areas of skin pigmentation and were suspected of having Neurofibromatosis Type 1 (NF1) without ever undergoing genetic testing.
Fetal Phenotype
2
Routine anatomy scan at 20 + 3 weeks' gestation was unremarkable except for the head circumference being on the 10th centile. An additional growth scan was performed at 29 + 1 week' gestation, identifying early onset fetal growth restriction: head circumference, femur length and estimated fetal weight all below the 2^nd^ centile. Lower limb bilateral post‐axial polydactyly was also detected (see Table 1A). Fetal dopplers were abnormal with raised uterine and umbilical artery pulsatility indices.
Diagnostic Method
3
Fetal DNA was extracted from cultured amniocytes. Initial QF‐PCR for common trisomies and microarray were unremarkable. Antenatal trio exome sequencing and analysis using a fetal anomaly gene panel was carried out as previously described [1].
Diagnostic Results and Interpretation
4
This identified a heterozygous maternally inherited likely pathogenic variant in SPRED1: NM_152594.3:c.1149_1152del p.(Gly385IlefsTer20) (see Table 1B). Monoallelic pathogenic variants in the SPRED1 gene are known to cause Legius syndrome. The variant caused a frameshift resulting in a premature truncating codon within the last exon and is therefore expected to escape nonsense mediated decay. There are multiple truncating variants 3′ of this variant classified as pathogenic in the ClinVar database LOVD [2] and the variant is predicted to destroy the sprouty‐related domain necessary to anchor SPRED1 in the membrane (PVS1_strong). The variant itself had been classified as pathogenic by five different laboratories in the ClinVar database (Variation ID 646826) and has been reported in multiple individuals in the literature (PS4_moderate). The variant is present in three individuals in the gnomADv4.1 population database consistent with the variable expressivity associated with Legius syndrome.
Pregnancy Outcomes and Neonatal Findings
5
The mother developed rapidly progressing pre‐eclampsia (hypertension alongside the fetal growth restriction) during her third trimester, which evolved into HELLP syndrome. Consequently, a male baby was delivered by emergency Caesarean Section at 32 + 4 weeks' gestation. Birthweight was 1.27 kg. Post‐axial polydactyly was confirmed on both feet and identified in the hands. The baby was admitted to SCBU for 4 weeks, requiring Oxygen for 2 days and NG feeding for 3 weeks. Postnatally, the baby was diagnosed with pulmonary stenosis during an admission for bronchiolitis. At 12 months, there were no concerns regarding his development but growth remained below average: weight 2nd–9th centile, head circumference 0.4th–2nd centile. Detailed inspection of the mother elicited five cafe‐au‐lait spots on her abdomen and lower back (see Figure 1A,B), findings significantly less prominent than in her mother and brother.
(A, B) Images of areas of skin pigmentation on mother. Key: (A) Cafe‐au‐lait spot on anterior lower abdomen of mother. (B) Cafe‐au‐lait spot on lower back of mother.
Discussion
6
Legius syndrome (LGSS) is an autosomal dominant disorder displaying similarities with the more severe NF1 (NF1; 162200) [3]. Individuals with Legius syndrome typically have multiple cafe‐au‐lait spots, dysmorphic features such as hypertelorism, lipomas, and mild learning disabilities. NF1, caused by variants in the neurofibromin gene (613113), also involves café‐au‐lait spots. However, Legius syndrome is not associated with the neurofibromas or tumor predisposition seen with NF1.
Published literature already associates Legius syndrome with post‐axial polydactyly [4, 5]. Interestingly, Messiaen et al. reported a case of postaxial polydactyly with the same pathogenicity as seen in this fetus [4]. Another reported post‐axial polydactyly case was also born prematurely at 32 weeks' gestation due to placental dysfunction [5].
Associating the pulmonary stenosis observed in our case with Legius syndrome is more controversial given that prematurity is itself a risk factor for pulmonary stenosis. However, Messiaen et al. reported another case of Legius Syndrome where mild pulmonary artery stenosis was observed [4]. Furthermore, a publicly available database of patients with SPRED1 variants records a child affected with a “heart murmur” [2], but further information on the nature of the cardiac condition was unavailable. The SPRED1 gene encodes a negative regulator of the RAS‐MAPK pathway, like neurofibromin, and thus may be considered a RASopathy [3]. Other RASopathies have been associated with pulmonary stenosis, including NF1 [6]. This case provides further evidence that post‐axial polydactyly identified on fetal imaging can be indicative of a SPRED1 variant, whilst also suggesting that cardiac abnormalities may need to be looked for with SPRED1 variants, representing a new feature of Legius syndrome.
Ethics Statement
The authors have nothing to report.
Consent
Written parental consent was obtained to share the details of this case.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. J. Chandler , E. Scotchman , R. Mellis , V. Ramachandran , R. Roberts , and L. S. Chitty , “Lessons Learnt From Prenatal Exome Sequencing,” Prenatal Diagnosis 42, no. 7 (2022): 831–844, 10.1002/pd.6165.35506549 PMC 9325487 · doi ↗ · pubmed ↗
- 2Leiden Open Variation Database . accessed March 4, 2025, https://databases.lovd.nl/shared/individuals/00205930.
- 3H. Brems and E. Legius , “Legius Syndrome, an Update. Molecular Pathology of Mutations in SPRED 1,” Keio Journal of Medicine 62, no. 4 (2013): 107–112, 10.2302/kjm.2013-0002-re.24334617 · doi ↗ · pubmed ↗
- 4L. Messiaen , S. Yao , H. Brems , et al., “Clinical and Mutational Spectrum of Neurofibromatosis Type 1‐like Syndrome,” JAMA 302, no. 19 (2009): 2111–2118, 10.1001/jama.2009.1663.19920235 · doi ↗ · pubmed ↗
- 5E. Denayer , M. Chmara , H. Brems , et al., “Legius Syndrome in Fourteen Families,” Human Mutation 32, no. 1 (2011): E 1985–E 1998, 10.1002/humu.21404.21089071 PMC 3038325 · doi ↗ · pubmed ↗
- 6N. Hilal , Z. Chen , M. H. Chen , and S. Choudhury , “RA Sopathies and Cardiac Manifestations,” Frontiers in Cardiovascular Medicine 10 (July 17, 2023): 1176828, 10.3389/fcvm.2023.1176828.37529712 PMC 10387527 · doi ↗ · pubmed ↗