Epidural Arteriovenous Fistula After Endoscopic Lumbar Laminectomy: A Rare Postoperative Presentation
Hideki Hayashi, Hirokuni Hashikata, Ryohei Goda, Yoshinori Maki, Hiroki Toda

TL;DR
A rare case of an epidural arteriovenous fistula (AVF) developing after endoscopic lumbar surgery is reported, highlighting its unusual postoperative presentation and successful treatment.
Contribution
This paper presents a rare case of epidural AVF following endoscopic lumbar laminectomy, expanding understanding of postoperative spinal vascular complications.
Findings
An epidural AVF was identified four months after endoscopic lumbar laminectomy in a 58-year-old patient.
The AVF was successfully treated surgically, leading to resolution of motor weakness and dysuria.
No recurrence was observed seven months post-surgery.
Abstract
Spinal dural and epidural arteriovenous fistulas (AVFs) are rare. However, the presentation of epidural AVFs after endoscopic surgery has rarely been described. This article reports a rare case of an epidural AVF that presented after an endoscopic lumbar laminectomy. A 58-year-old man underwent endoscopic lumbar laminectomy at the L2-L4 level with 50 ml of intraoperative blood loss and no intraoperative complications, including bleeding, dural injury, or cerebrospinal fluid (CSF) leakage. He presented with recurrent motor and sensory disturbances in the right lower extremity. Follow-up magnetic resonance imaging (MRI) examination four months after endoscopic surgery revealed a hyperintense lesion in the lower thoracic spinal cord. Steroid pulse therapy and plasma exchange for possible myelitis failed to improve neurological deficits. During this period, motor and sensory disturbances in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
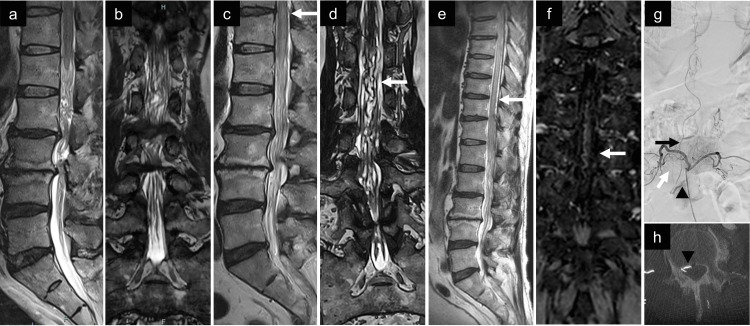 Figure 1
Figure 1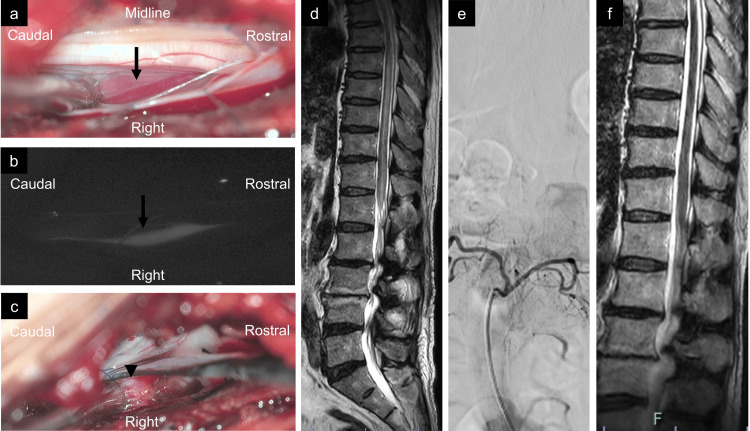 Figure 2
Figure 2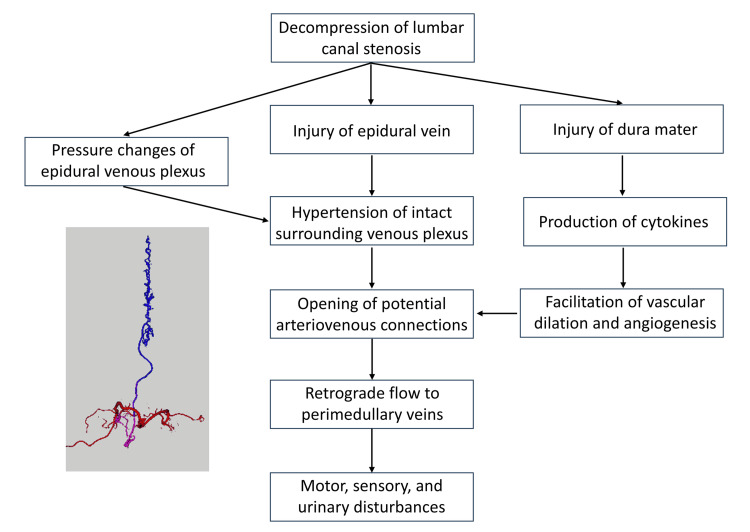 Figure 3
Figure 3| Author | Year | Age (years), Sex | Type of AVF | Previous lumbar surgery | Duration after lumbar surgery | Duration between treatment and symptom | Feeder on DSA | Symptoms | Treatment | Proposed Pathogenesis | Follow-up | Outcome |
| Yoshino et al. [ | 1998 | 27, Male | Dural AVM | L4-5 ALIF, L5-S discectomy | 7 years | Not mentioned | Left iliolumbar artery | Motor and sensory | TAE + Surgery | Thrombus or thrombophlebitis | Not mentioned | Partial relief |
| Asakuno et al. [ | 2002 | 60, Male | Dural AVF | L5-S discectomy | 2 years | 1 year | Left lateral sacral artery | Motor, sensory, and urinary dysfunction | Surgery | Thick fibrous tissue | Not mentioned | Good recovery |
| Cho et al. [ | 2008 | 49, Male | Extradural AVF | L3-5 PLIF | 3 years | 3 months | Left iliolumbar artery | Motor, sensory, and urinary dysfunction | TAE | Vascular injury or dural tearing | 6 months | Partial relief, persistent bladder dysfunction |
| Khaldi et al. [ | 2009 | 68, Male | Epidural AVF | L3-4 discectomy | 2 years | 2 months | Left L3 | Motor, sensory, and urinary dysfunction | Surgery | Disturbance of venous drainage by epidural manipulation | 6 weeks | Improving |
| Lim et al. [ | 2009 | 65, Male | Epidural AVF | L2-4 laminectomy | 4 years | 1 day | Right L3 | Motor, sensory, and urinary dysfunction | TAE | Injury of epidural veins, predisposing to venous thrombosis | Not mentioned | Good recovery |
| Rangel-Castilla et al. [ | 2011 | 37, Male | Epidural AVF | L4-5 laminectomy | 4 months | Not mentioned | Left L3-5 | Motor, sensory, and urinary dysfunction | TAE | Not mentioned | 1 year | Good recovery |
| Murakami et al. [ | 2015 | 69, Male | Epidural AVF | L4-5 endoscopic discectomy | 8 years | 10 months | Bilateral L4 | Motor, sensory, and urinary dysfunction | TAE | Occlusion of epidural venous plexus and local venous hypertension | 1 year | Good recovery |
| Elswick et al. [ | 2020 | 74, Female | Dural AVF | T11-Pelvis PLF | 5 years | 6 months | Left T12 | Motor, sensory, and urinary dysfunction | Surgery | Traumatic or inflammatory mechanism | 5 months | Partial relief, persistent bladder dysfunction |
| Ouyang et al. [ | 2021 | 54, Male | Dural AVF | L3-5 PLIF | 8 years | 7 months | Left T10 | Motor, sensory, and urinary dysfunction | Surgery | Reopening of the radicular vein | 14 months | Partial relief, persistent bladder dysfunction |
| Present case | 2025 | 58, Male | Epidural AVF | L2-4 endoscopic discectomy | 5 months | 3 months | Right L2 | Motor, sensory, and urinary dysfunction | Surgery | 7 months | Good recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Spinal Hematomas and Complications · Intracranial Aneurysms: Treatment and Complications
Introduction
Endoscopic lumbar spinal surgery has emerged as a safe and effective technique for treating various spinal conditions, including lumbar disc herniation, stenosis, and foraminal stenosis. A comprehensive literature review identified dural tears, perioperative hematoma, transient dysesthesia, nerve root injury, and recurrence as the most common complications across different endoscopic approaches [1]. However, spinal epidural arteriovenous fistula (AVF) has rarely been reported as a complication of lumbar spine surgery [2-10]. The initial misdiagnosis rate of spinal dural AVF is 81%, while the erroneous treatment rate is 62% [10]. It is difficult to suspect dural AVF after lumbar spine surgery because of nonspecific manifestations. Common mimickers, such as transverse myelitis, multiple sclerosis, chronic inflammatory demyelinating polyneuropathy, postoperative scar tissue, and discitis, may present with overlapping symptoms, making early recognition of vascular lesions more challenging. It is imperative to acknowledge the potential of diagnostic delays as a contributing factor to permanent motor, sensory, and sphincter dysfunction. Therefore, it is crucial to establish a differential diagnosis to ensure comprehensive patient management.
Spinal arteriovenous shunts are typically classified based on their anatomical locations and venous drainage patterns. According to the updated classification proposed by Takai et al. [11], these lesions are categorized into five main types: dural AVF (Type I), glomus arteriovenous malformation (AVM) (Type II), juvenile AVM (Type III), perimedullary AVF (Type IV), and epidural AVF (Type V). Type V is further divided into Type Va, which drains into the intradural venous system, and Type Vb, which drains into the epidural venous plexus. This classification system provides a clinically relevant framework for diagnosis and treatment planning.
Herein, we report a rare case of Type Va epidural AVF that occurred after endoscopic lumbar laminectomy and was surgically treated. While a limited number of spinal epidural AVFs following lumbar surgery have been reported, these cases often share common clinical challenges: a highly variable latency period between surgery and symptom onset, insidious progression of motor and sensory deficits, and frequent delays in accurate diagnosis due to nonspecific clinical presentations and misleading imaging findings. Conventional magnetic resonance imaging (MRI) may fail to reveal abnormal vascular structures in the early phase, and the resulting diagnostic ambiguity can lead to delayed treatment and irreversible neurological deterioration. Moreover, the precise pathogenesis of postoperative AVFs remains incompletely understood, although the proposed mechanisms include surgical stress, venous hypertension, and angiogenesis induced by local inflammation [2-10]. In this context, the present case not only contributes to the growing recognition of this rare postoperative complication but also provides an opportunity to synthesize prior reports and highlight critical pitfalls in diagnosis and management.
Case presentation
A 58-year-old man presented with intermittent claudication and underwent endoscopic lumbar laminectomy for L2/3 and L3/4 lumbar spinal canal stenosis at another hospital in March 2024 (Figures 1a-1b). The operation was performed using a tubular retractor without pumped irrigation for 78 minutes, with 50 ml of blood loss and no complications like cerebrospinal fluid (CSF) leakage. The patient's symptoms improved during the first two months postoperatively, but gradually developed weakness and sensory deficits in the right lower extremity in May 2024. Lumbar MRI two months after laminectomy showed improvement in spinal canal stenosis, accompanied by slight hyperintensity and signal voids in the conus medullaris (Figures 1c-1d). Four months after laminectomy, the patient was referred to the neurology department of our hospital (Kitano Hospital) in July 2024 because of the rapid worsening of motor paralysis after caudal epidural block injection at another clinic. The specifics of the injection were not accessible. Lumbar puncture revealed a normal cell profile, normal protein levels, no abnormalities on flow cytometry, and negative CSF oligoclonal bands. Thoracolumbar MRI revealed hyperintensity below the mid-thoracic level on T2-weighted imaging, leading to a diagnosis of myelitis (Figure 1e).
Preoperative radiological findings.(a) Initial sagittal T2-weighted MRI showing lumbar spinal canal stenosis at the L2/L3 and L3/L4 levels, with faint intramedullary hyperintensity. (b) Initial coronal FIESTA MRI showing lumbar spinal canal stenosis at the L2/L3 and L3/L4 levels, without abnormal vessels. (c) Sagittal T2-weighted MRI after laminectomy showing resolution of the spinal canal stenosis, but a slight flow void (white arrow) was observed dorsally to the conus medullaris. Hyperintense lesions in the conus medullaris were also observed compared to the initial image. (d) Coronal FIESTA MRI after showing lumbar spinal canal stenosis at the L2/L3 and L3/L4 levels without abnormal vessels (white arrow). (e) The hyperintense lesion was enlarged longitudinally to the mid-thoracic level. Multiple dorsal flow voids (white arrow) were concurrently observed. (f) Coronal contrast-enhanced MRI demonstrating an abnormal vessel (white arrow) running longitudinally in the thoracic spinal cord. (g) Digital subtraction angiography of the right L2 segmental artery, revealing an epidural arteriovenous fistula fed by the dorsal somatic branch (white arrow). The fistula (black arrowhead) drained into the perimedullary vein (black arrow). (h) The shunt pouch (black arrowhead) was located in the epidural space on the axial image of the rotational three-dimensional angiography.MRI: magnetic resonance image; FIESTA: fast imaging employing steady-state acquisition
The patient was initially treated under the diagnosis of myelitis with intravenous methylprednisolone at a dose of 1000 mg/day for five consecutive days, followed by plasma exchange therapy administered every two to three days. Subsequently, an additional course of intravenous methylprednisolone (1000 mg/day for three days) was administered. These treatments yielded only a transient and mild improvement in motor function and bladder symptoms, which gradually worsened. Contrast-enhanced gadolinium MRI revealed abnormal blood vessels on the anterior and posterior surfaces of the thoracic spinal cord (Figure 1f). Therefore, the patient was referred to our neurosurgery department in August 2024. The patient had bilateral hypoesthesia below the groin, with grade 3 strength on the right side and grade 4 strength on the left lower extremity. Knee and Achilles tendon reflexes were diminished bilaterally. He had difficulty standing and bladder dysfunction. Angiography of the right segmental L2 artery showed an epidural AVF at the right L2/3 level fed by the dorsal somatic branch, draining retrogradely into the perimedullary vein (Figure 1g). Rotational three-dimensional angiography revealed a shunt pouch in the epidural space (Figure 1h).
One day after the epidural AVF was diagnosed, the patient underwent a right L2/3 hemilaminectomy and epidural AVF extraction. Owing to the urgency of the patient’s neurological decline, the surgery was performed emergently without intraoperative neurophysiological monitoring. Because a left unilateral laminectomy for bilateral decompression was performed in the previous endoscopic surgery, the adhesion between the dorsal dura and postoperative granulation needed to be dissected. However, the right lateral and ventral sides of the dura near the epidural shunt fistula were intact and the ligamentum flavum was preserved. After dural opening with an exoscope, a dilated vein emanating from the right L2/3 foramen (Figure 2a) and early retrograde filling were confirmed using indocyanine green angiography (Figure 2b). All exoscopic procedures were conducted under high magnification, and the draining vein was coagulated only after careful inspection to ensure that no critical perimedullary arteries or veins were present in the operative field. After suturing the dura, the epidural shunt pouch ventromedial to the right L3 nerve root was confirmed (Figure 2c) and was removed. Postoperative MRI showed disappearance of the dilated vessels on T2-weighted images (Figure 2d), and contrast-enhanced images and digital subtraction angiography (DSA) revealed disappearance of the epidural AVF (Figure 2e). Three weeks after the surgery, the patient was discharged for inpatient rehabilitation. His lower extremity strength improved at discharge, with grade 4 on the right side and grade 5 on the left side. From the preoperative period to three months postoperatively, Japanese Orthopaedic Association scores improved from 3 to 12 and the Oswestry Disability Index improved from 74 to 48. However, the patient continued to undergo self-catheterization for persistent neurogenic bladder dysfunction. MRI performed four months after surgery showed improvement in edema of the spinal cord (Figure 2f). At an outpatient visit seven months after surgery, motor paralysis, gait disturbance, and dysuria improved. However, numbness persisted in both lower limbs.
Intraoperative and postoperative radiological findings.(a,b) After opening the dura, a dilated reddish vein (black arrow) was identified. Early retrograde flow in the vein was observed with ICG (b). The veins were coagulated and obliterated. (c) The shunting pouch (black arrowhead) of the epidural arteriovenous fistula was ventrally identified after dural retraction. (d) Postoperative sagittal T2-weighted MRI showing disappearance of flow voids but with residual edema of the spinal cord. (e) Postoperative digital subtraction angiography revealing the disappearance of the epidural arteriovenous fistula. (f) Sagittal T2-weighted MRI four months after surgery showing improvement in spinal cord edema.ICG: indocyanine green; MRI: magnetic resonance image
Discussion
Spinal dural and epidural AVFs are rare causes of neurological deterioration after lumbar surgery. In conventional lumbar MRI, the correct diagnosis of vascular malformations is difficult because of the narrow image of the conus medullaris (Figures 1a-1b). In previous reports on AVF after lumbar surgery, almost all patients presented with severe symptoms, including bladder dysfunction (Table 1) [2-10]. Re-examination with MRI, including the midthoracic spinal cord and conus medullaris (Figure 1c), should be considered to detect spinal cord edema and dilated vessels if the patient shows clinical symptoms dissociated from the imaging findings. Given that the initial diagnosis in the present patient was myelitis due to indistinct signal voids, gadolinium contrast enhancement should be considered to reveal vascular malformations [10].
On spinal angiography, all segmental arteries from the upper thoracic to the iliolumbar [2,4] and sacral arteries [3] should be catheterized to accurately evaluate the entire angioarchitecture and to develop a treatment plan. For feeding arteries, the dorsal somatic branches of these segmental arteries mainly supply AVFs and single or multiple branches are important for deciding the approach route for transarterial embolization [12]. Localization of the shunt pouch in association with the vertebrae is often difficult; subsequently, rotational three-dimensional angiography is useful for identifying the dural or epidural shunt, as shown in previous cases [8,12]. Given its ability to provide precise spatial localization and improved visualization of angioarchitecture, rotational three-dimensional angiography should be strongly considered, if not routinely implemented, in the evaluation of suspected spinal vascular anomalies. This is particularly important in patients with a history of prior spinal surgery and ambiguous MRI findings, where conventional angiography alone may be insufficient to distinguish between dural and epidural AVFs or delineate complex shunt anatomy. Understanding the location of the intradural perimedullary drainer associated with the postoperative lumbar vertebrae and instruments is critical for surgical planning, and paravertebral drainage can be a candidate access route for transvenous embolization [12].
The mechanism of AVF is assumed to involve injury of the epidural connective tissue involving the epidural veins, predisposing the patient to venous thrombosis and leading to the formation of an AVF and complex retrograde venous drainage into the perimedullary vein [8]. In the present case, the epidural ligamentum flavum and veins were thought to be free of direct injuries on the opposite side of the surgical approach route from the previous endoscopic laminectomy. Although the duration between lumbar surgery and the onset of AVF was four months to eight years in previous reports (Table 1) [2-10], the present case showed motor and sensory disturbance only two months postoperatively. Venous hypertension caused by damage to the epidural venous plexus may have concentrated on the intact venous drainage route and induced retrograde flow to the perimedullary vein in the relatively early phase (Figure 3). In this case, the venous pressure changes caused by decompressive laminectomy may have revealed a previously existing AVF. Because local inflammation of the dura induced by surgical stress may lead to the production of cytokines, facilitation of vascular dilation and angiogenesis, and opening of potential arteriovenous connections, this mechanism may have also contributed to the development of epidural AVF in our case [13]. In the present case, histopathological analysis of the shunt pouch could not be performed because the lesion was coagulated intraoperatively to achieve complete obliteration, precluding safe tissue sampling. To date, no previous report has included histological confirmation of AVF pathogenesis in similar cases. As a result, the proposed mechanisms, such as venous hypertension, inflammatory changes, and angiogenesis, remain speculative. Further studies incorporating histopathological evaluation are needed to validate these hypotheses. Only a limited number of cases of postoperative epidural AVFs have been described in the literature; therefore, further studies should be conducted to clarify the mechanism underlying the development of postoperative lumbar epidural AVFs.
Diagram illustrating the proposed mechanism of AVF development following lumbar surgery.AVF: arteriovenous fistulaThe figure was created by the authors.
Although the patients underwent treatment after a relatively short duration of symptoms (one day to one year), 50% of the patients experienced partial relief, especially bladder dysfunction (Table 1) [2-10]. Considering the severity of permanent disabilities, prompt diagnosis and treatment are crucial. Surgical extraction of AVF is superior to endovascular treatment in terms of the degree of postoperative neurological recovery, treatment success, and recurrence rates of spinal dural AVFs [14]. According to previous lumbar surgical conditions, the fastest possible treatment is desirable because there are no significant differences between surgery [3,5,9,10] and endovascular treatment [4,6,7].
This study has several limitations. First, it is a single case report, which limits the generalizability of the findings. Second, the mechanisms underlying the development of postoperative vascular abnormalities remain hypothetical and require further investigation. Third, the follow-up period of seven months was relatively short, which is insufficient to assess the long-term outcomes and recurrence risk. In a large multicenter cohort [14], among the neurosurgical (n = 145) and endovascular (n = 50) treatment groups of single dural AVFs (n = 195), the rate of initial treatment failure or recurrence was significantly higher in the index endovascular treatment group (0.68% and 36%). Recurrence after the initial treatment, including cases identified as late as 62 months post-treatment, was documented, particularly in patients who underwent endovascular procedures. Given these findings, we recommend a minimum follow-up duration of two years, with extended surveillance of up to five years in cases treated endovascularly, to adequately monitor for recurrence or delayed complications. To address these limitations, future studies should include a larger number of patients and longer follow-up periods.
Conclusions
Here, we report a rare case of epidural AVF that presented after endoscopic lumbar laminectomy. This case highlights the importance of considering spinal vascular malformations in the differential diagnosis of delayed postoperative neurological decline, even when the initial lumbar imaging appears unremarkable. Early recognition is critical to avoid irreversible deficits. Given the nonspecific symptoms and diagnostic delays commonly associated with AVFs, we recommend that thoracic spinal cord imaging should be considered routinely in patients with progressive neurological deterioration after lumbar surgery. Greater awareness and systematic imaging may lead to earlier diagnosis and improved outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Complications and management of endoscopic spinal surgery Neurospine Ju CI Lee SM 56772020233701685410.14245/ns.2346226.113PMC 10080410 · doi ↗ · pubmed ↗
- 2Acquired dural arteriovenous malformations of the lumbar spine: case report Neurosurgery Yoshino O Matsui H Hirano N Tsuji H 13871389421998963220210.1097/00006123-199806000-00126 · doi ↗ · pubmed ↗
- 3Dural arteriovenous fistula and progressive conus medullaris syndrome as complications of lumbar discectomy J Neurosurg Asakuno K Kim P Kawamoto T Ogino M 3753799720021240839710.3171/spi.2002.97.3.0375 · doi ↗ · pubmed ↗
- 4Acquired spinal extradural arteriovenous fistula after instrumented lumbar surgery J Neurosurg Spine Cho JH Ahn JY Kuh SU Chin DK Yoon YS 9200810.3171/SPI/2008/9/7/08318590416 · doi ↗ · pubmed ↗
- 5Spinal epidural arteriovenous fistula with late onset perimedullary venous hypertension after lumbar surgery: case report and discussion of the pathophysiology Spine (Phila Pa 1976) Khaldi A Hacein-Bey L Origitano TC 77577934200910.1097/BRS.0b 013e 3181 ae 4a 5219934798 · doi ↗ · pubmed ↗
- 6Spinal epidural arteriovenous fistula: a unique pathway into the perimedullary vein: a case report Interv Neuroradiol Lim SM Choi IS 4664691520092046588810.1177/159101990901500417 PMC 3299437 · doi ↗ · pubmed ↗
- 7Spinal extradural arteriovenous fistulas: a clinical and radiological description of different types and their novel treatment with Onyx J Neurosurg Spine Rangel-Castilla L Holman PJ Krishna C Trask TW Klucznik RP Diaz OM 5415491520112180095410.3171/2011.6.SPINE 10695 · doi ↗ · pubmed ↗
- 8Lumbar spinal epidural arteriovenous fistula with perimedullary venous drainage after endoscopic lumbar surgery Interv Neuroradiol Murakami T Nakagawa I Wada T Kichikawa K Nakase H 2492542120152594811410.1177/1591019915583212 PMC 4757241 · doi ↗ · pubmed ↗