Primary Synovial Osteochondromatosis of the Elbow in a Young Adult Complicated by Osteoarthritis: A Case Report
Abdoulrazak Egueh Nour, Chirwa Abdillahi Mahamoud, Chaimae Amrani, Bouknani Nawal, Amal Rami

TL;DR
A 25-year-old man with chronic elbow pain was diagnosed with a rare condition called primary synovial osteochondromatosis complicated by osteoarthritis and successfully treated with surgery.
Contribution
This case report highlights the rare occurrence of primary synovial osteochondromatosis in the elbow complicated by osteoarthritis.
Findings
The patient showed multiple calcified bodies in the elbow joint with arthritic changes confirmed by imaging.
Surgical synovectomy and debridement significantly improved pain and joint function.
Elbow involvement is uncommon and often diagnosed late due to nonspecific symptoms.
Abstract
Primary synovial osteochondromatosis is a benign and uncommon pathology, resulting from metaplasia of the synovial tissue, of unknown cause, leading to the formation of multiple cartilaginous nodules, some of which secondarily detach to form free articular bodies. Its location in the elbow, complicated by osteoarthritis, is poorly described in the literature. We present the case of a 25-year-old man presenting for chronic right elbow pain with joint locking and swelling without a history of trauma. Physical examination revealed an increase in elbow volume compared to the contralateral elbow, with limitation of active or passive joint range of motion. Radiological examinations, including standard radiography (X-rays), CT, and MRI, revealed multiple rounded, floating, and calcified bodies disseminated in the joint associated with arthritic changes, confirming the diagnosis of primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
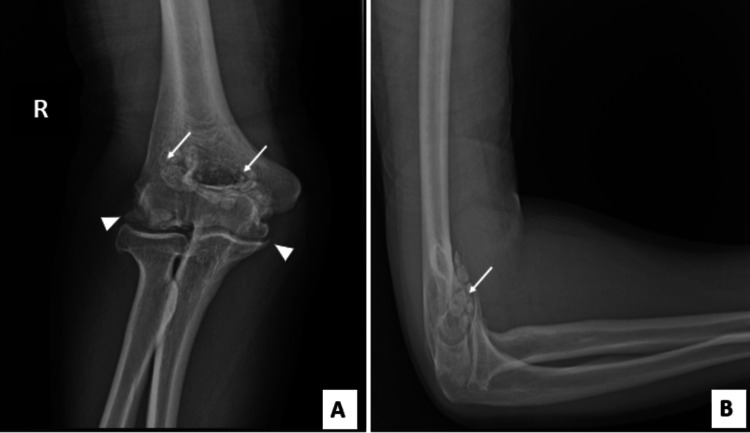 Figure 1
Figure 1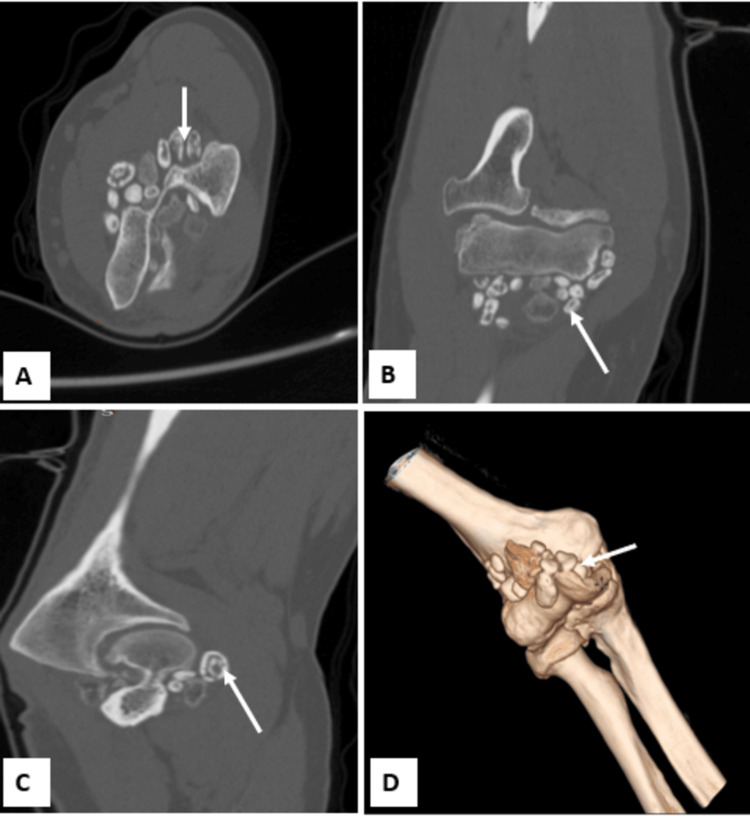 Figure 2
Figure 2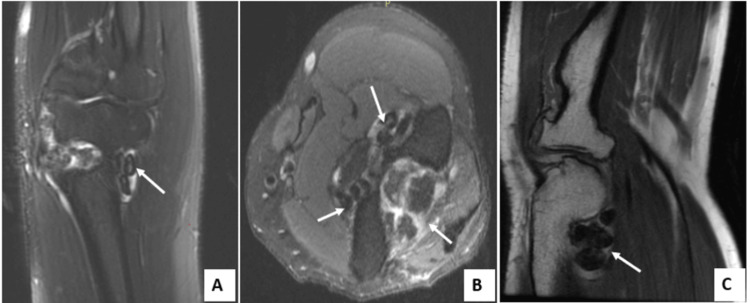 Figure 3
Figure 3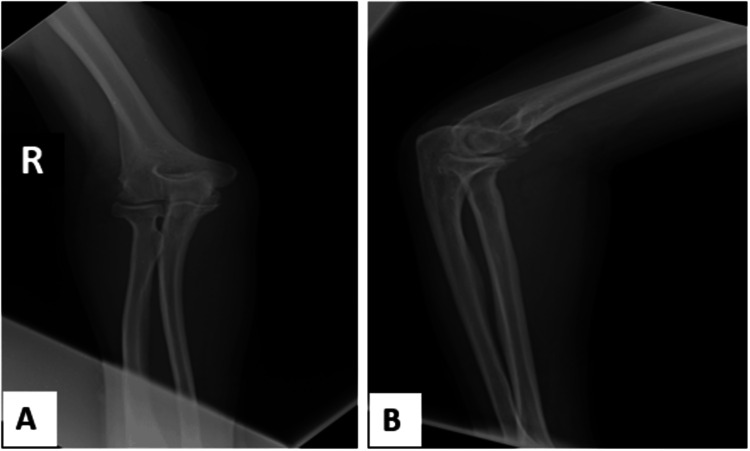 Figure 4
Figure 4| Red blood cells (1012 / L) | 5,35 | 4.25-6 |
| Hemoglobin (g/dL) | 15,200 | 13.0-18.0 |
| Hematocrit (%) | 44,600 | 39-53 |
| Leukocytes (103/mm³) | 6,800 | 4-11 |
| Platelets (103/mm³) | 240 | 150-400 |
| Blood creatinine (mg/L) | 8,700 | 6.7-11.7 |
| Protein Totals (g/L) | 68 | 64-83 |
| Calcium (mg/L) | 93 | 86-100 |
| Urea (g/L) | 0,23 | 0.17-0.49 |
| Triglycerides (g/L) | 0,89 | <1.30 |
| Glycosylated Hemoglobin (HbA1c) (%) | 5,300 | 4.5-6.2 |
| Serum Ferritin (ng/ml) | 251 | 30-400 |
| TSH us (µIU/mL) | 0,71 | 0.27-4.20 |
| ESR 1st hour (mm/h) | 10 | <13 |
| C-reactive Protein (mg/L) | 5 | < 8 |
| Rheumatoid Factors (IU/ml) | <14 | <30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal synovial abnormalities and treatments · Bone Tumor Diagnosis and Treatments · Genital Health and Disease
Introduction
Primary synovial osteochondromatosis is a benign and uncommon pathology, characterized by cartilaginous metaplasia of the synovial membrane, leading to the formation of osteochondral nodules within the joint cavity [1]. The disease is classically monoarticular and mainly affects the large joints, particularly the knee, while elbow involvement is less common [2]. Due to the rarity of this localization, its true prevalence is difficult to establish. The majority of published data consists of isolated case reports or small case series, with the largest series reporting up to 30 cases [3]. But any structure covered with synovial fluid, including all synovial joints, may be affected.
Occurring most often between the ages of 30 and 50 and more widespread in men, this pathology has a slow and progressive evolution and manifests itself by joint pain, swelling, functional discomfort, or blockages [4]. Multimodal imaging, including X-ray, CT scan, and MRI, plays a vital role in early diagnosis as well as assessment of synovial and articular cartilage involvement.
Treatment is based on surgical management, combining synovectomy and removal of loose bodies, while limiting the risk of recurrence or arthritic progression [5].
Case presentation
A 25-year-old manual worker with no significant medical or traumatic history presented with mechanical pain in his right elbow, which had been developing for three months and had increasing functional impairment. He also reported episodes of locking and progressive limitation of joint range of motion.
Clinical examination revealed moderate joint effusion, pain on palpation of the olecranon fossa and humeroradial joint space, and limited active extension and flexion. There were no local inflammatory signs or associated neurological or vascular involvement.
The biological workup, including complete blood count, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and rheumatoid factor, was within normal limits, thereby excluding an underlying inflammatory or autoimmune disorder, as seen in Table 1.
Standard radiography of the elbow revealed multiple rounded intra-articular opacities, suggesting free osteocartilaginous bodies associated with joint narrowing, subchondral changes, and osteophyte formation (Figure 1). Non-contrast CT showed grouped intra-articular calcifications in the olecranon fossa, in the coronoid fossa, confirming their presence in the anterior and posterior compartments (Figure 2).
X-rays of the right elbow (A) anteroposterior view (B) lateral viewRevealed multiple intra-articular loose bodies (arrow), pinching of the joint space, subchondral sclerosis, and osteophytes (arrowhead).
CT scan of the elbow (A) axial plane, (B) coronal plane, (C) sagittal plane, (D) three-dimensional reconstructionShowed multiple calcifications of the periarticular soft tissues(white arrow), associated with sclerotic lesions and pinching of the joint space.
Magnetic resonance imaging showed thickened synovium, intra-articular effusion, as well as several intra-articular nodular formations in T1 and T2 hypointense, reflecting osteochondral bodies and cartilaginous lesions compatible with early osteoarthritis (Figure 3).
T2-weighted MRI (A) coronal, (B) axial; T1-weighted MRI (C) sagittalShows joint effusion and multiple hypointense nodules on T1- and T2-weighted sequences, consistent with cartilaginous loose bodies, as well as associated degenerative changes and synovial thickening.
The diagnosis of primary synovial osteochondromatosis, complicated by osteoarthritis, was made. Surgical synovectomy with removal of loose bodies was performed. Histopathological analysis confirmed the diagnosis of primary synovial osteochondromatosis without signs of malignancy. The post-operative outcome was favorable, with functional rehabilitation and a clear improvement in pain and joint mobility at follow-up. At six months, radiographic control showed no residual calcified bodies, indicating effective complete excision (Figure 4).
Postoperative radiographs of the right elbow (A) anteroposterior (B) lateral Shows no calcific densities.
Discussion
Synovial osteochondromatosis (SOC) is an uncommon benign condition related to synovial metaplasia leading to the formation of multiple intra-articular cartilaginous nodules [1].
It can be primitive of idiopathic origin or secondary to an underlying joint pathology, such as osteoarthritis, trauma, inflammatory arthropathies, or neurological damage,e and can be both intraarticular and extraarticular [4,6].
Described in the 16th century by Ambroise Paré, then studied by Laennec and Brodie, joint damage by free cartilaginous bodies has historically been associated with a synovial origin [7]. The first case reported at the elbow dates back to 1918, but the disease can affect any synovial joint.
The disease is generally monoarticular and preferentially affects men between 30 and 50 years of age with a clear predominance in the knee; locations in the elbow, hip, shoulder or ankle are less frequent and manifest clinically by chronic pain, swelling, stiffness and sometimes mechanical blockage linked to the presence of free bodies [8,9].
In terms of evolution, Milgram and Pease established, from a series of 30 cases, a three-stage classification of synovial osteochondromatosis, based on histopathological criteria, ranging from active synovitis without free bodies (stage I) to a form with ossified free bodies (stage II) responsible for mechanical symptoms and inactive synovitis with persistence of ossified free bodies (stage III) [3]. Our patient falls into this latter stage. Edeiken et al. then proposed a stage IV, characterized by a large intra- or extra-articular cartilaginous mass [10].
Imaging plays a central role in the diagnosis and characterization of primary synovial osteochondromatosis. Standard radiography is the first-line examination and can reveal rounded, calcified opacities corresponding to intra-articular osteochondral bodies. However, in early non-calcified forms, the results can be falsely reassuring. In this context, computed tomography or MRI is useful to confirm the diagnosis. Computed tomography (CT) allows for more precise mapping of loose bodies and associated bone remodeling, particularly in cases of secondary osteoarthritis. More sensitive magnetic resonance imaging (MRI) completes the evaluation by visualizing soft tissues, hypertrophied synovium, effusions, as well as possible cartilaginous or extra-articular involvement, and non-calcified forms [9].
No biological marker is specific to the primary form, but certain anomalies can point towards a secondary form linked to an underlying joint pathology [11].
The differential diagnosis of synovial osteochondromatosis includes degenerative, inflammatory conditions (such as rheumatoid arthritis or gout, benign tumors such as periosteal chondroma or giant cell tumor, pigmented villonodular synovitis, and hydroxyapatite deposits. Finally, malignant lesions such as chondrosarcoma or synovial sarcoma must be systematically excluded, particularly in recurrent or atypical forms [9]. Cross-analysis of imaging, clinical, and biological data often allows for a reliable diagnosis.
The standard treatment for synovial osteochondromatosis is the excision of loose bodies, often by arthroscopic route, associated or not with a synovectomy [12]. In our case, a synovectomy of the anterior and posterior compartments was performed. The prognosis is generally favorable, but recurrences are possible, often linked to incomplete excision, and malignant transformation into chondrosarcoma, although rare, has been described, mainly in recurrent forms.
Conclusions
Primary synovial osteochondromatosis, although unusual in the elbow, should be included in the differential diagnosis in the presence of chronic pain, joint blockages, and loose bodies visible on imaging. Multimodal evaluation by radiography, CT, and MRI is essential for an accurate and early diagnosis. Surgical excision combined with synovectomy offers good functional results and limits the risk of recurrence. Finally, rigorous clinical and radiological monitoring is essential for early detection of any complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arthroscopic treatment of synovial osteochondromatosis of the elbow. Case report and literature review Rev Bras Ortop Terra BB Moraes EW de Souza AC Cavatte JM Teixeira JC De Nadai A 6076125020152653521010.1016/j.rboe.2015.08.014PMC 4610989 · doi ↗ · pubmed ↗
- 2Giant solitary synovial osteochondromatosis of the elbow causing ulnar nerve neuropathy: a case report and review of literature J Brachial Plex Peripher Nerve Inj Al-Najjim M Mustafa A Fenton C Morapudi S Waseem M 1820132335125310.1186/1749-7221-8-1PMC 3599958 · doi ↗ · pubmed ↗
- 3Synovial osteochondromatosis: a histopathological study of thirty cases The Journal of Bone & Joint Surgery Milgram JW 79280159 september 1977 https://journals.lww.com/jbjsjournal/toc/1977/59060908703 · pubmed ↗
- 4Incidental finding of synovial osteochondromatosis: a case report Cureus Bhagat SS Hammond J Fuller-Sincock DM Zehra SB 014202210.7759/cureus.28051 PMC 947637536120269 · doi ↗ · pubmed ↗
- 5Arthroscopic management of elbow synovial chondromatosis Medicine (Baltimore) Zhu W Wang W Mao X Chen Y 097201810.1097/MD.0000000000012402 PMC 620051730290596 · doi ↗ · pubmed ↗
- 6Tenosynovial (Extra-articular) Chondromatosis of the Extensor Digitorum Longus Tendon and Synovial Chondromatosis of the Ankle: Treated by Extensor Digitorum Longus Tendoscopy and Ankle Arthroscopy Foot Ankle Spec Lui TH 422425820152541629810.1177/1938640014560165 · doi ↗ · pubmed ↗
- 7Synovial osteochondromatosis of the elbow J Bone Joint Surg Br Kamineni S O’Driscoll SW Morrey BF 9619668420021235838610.1302/0301-620x.84b 7.12766 · doi ↗ · pubmed ↗
- 8Generalized synovial chondromatosis of the knee: a comparison of removal of the loose bodies alone with arthroscopic synovectomy Arthrosc J Arthrosc Relat Surg Ogilvie-Harris DJ Saleh K 16617010199410.1016/s 0749-8063(05)80088-x 8003143 · doi ↗ · pubmed ↗