Clinical Insights Into Aortitis Following Granulocyte Colony-Stimulating Factor Use in an Older Male Patient
Kaichi Sugihara, Takahiro Kamihara, Takuya Omura, Atsuya Shimizu

TL;DR
An older male cancer patient developed aortitis after using granulocyte colony-stimulating factor, highlighting the need for clinicians to consider this rare side effect.
Contribution
This case report highlights G-CSF-associated vasculitis in older male cancer patients as a rare but important clinical consideration.
Findings
A 74-year-old male developed aortitis following filgrastim administration for neutropenia.
Contrast-enhanced CT scans revealed aortic wall thickening, which improved with prednisolone treatment.
The case suggests that G-CSF can cause vasculitis, and clinicians should consider aortitis in similar patients.
Abstract
This report describes a rare case of extensive aortitis associated with granulocyte colony-stimulating factor (G-CSF) administration in a 74-year-old male with castration-resistant prostate cancer and multiple metastases. The patient developed recurrent fever and elevated inflammatory markers after receiving filgrastim for docetaxel-induced neutropenia. Despite antibiotic treatment, his fever persisted. A contrast-enhanced CT scan revealed circumferential wall thickening of the common carotid artery to the aortic arch and abdominal aorta, prompting suspicion of G-CSF-associated vasculitis. Following the initiation of prednisolone, the patient's fever resolved, inflammatory markers decreased, and clinical status improved. Subsequent CT scans showed a reduction in aortic wall thickening. This case highlighted that G-CSF-associated vasculitis can occur in older male cancer patients, urging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
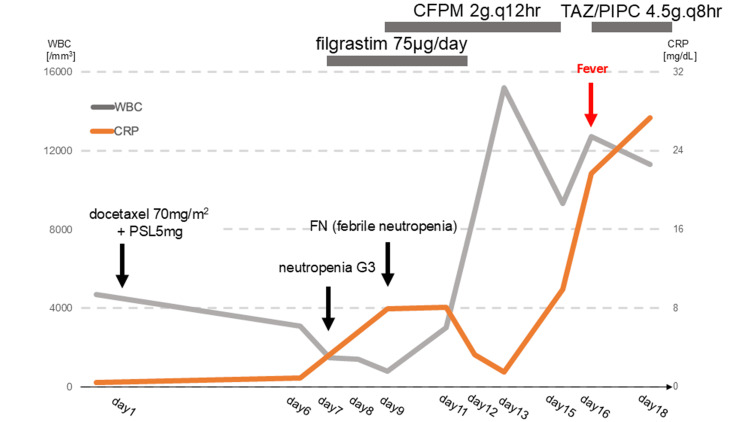 Figure 1
Figure 1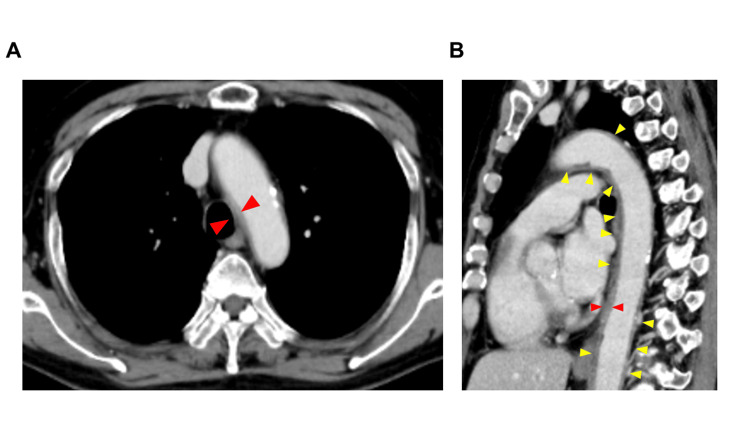 Figure 2
Figure 2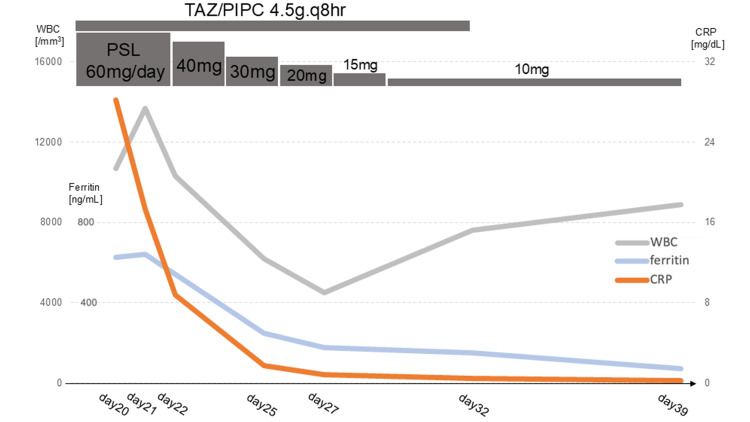 Figure 3
Figure 3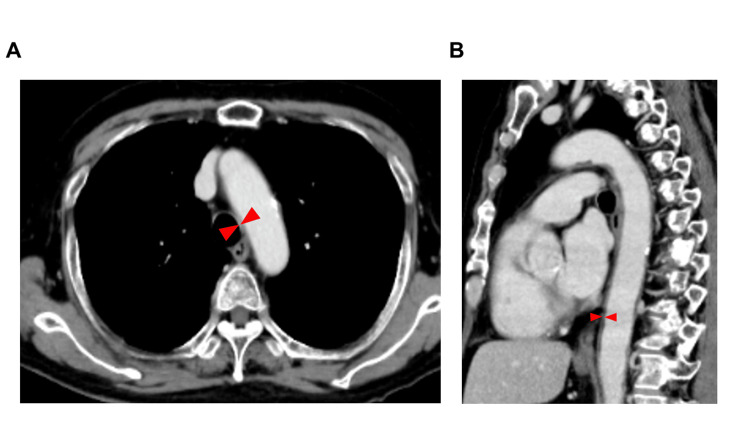 Figure 4
Figure 4| Hematology | |||
| Parameter | Patient Value | Unit | Reference Range |
| White Blood Cell Counts | 4700 | /μL | 3300-8600 |
| Neutrophils | 49.2 | % | 38-68 |
| Lymphocytes | 39.8 | % | 27-47 |
| Monocytes | 8.7 | % | 2.0-8.0 |
| Eosinophils | 2.1 | % | 2.0-8.0 |
| Basophils | 0.2 | % | 0.0-7.0 |
| Red Blood Cell Counts | 4.87×106 | /μL | 4.35-5.55×106 |
| Hemoglobin | 12.1 | g/dL | 13.7-16.8 |
| Hematocrit | 39 | % | 40.7-50.1 |
| Mean Corpuscular Volume | 80.1 | fL | 83.6-98.2 |
| Mean Corpuscular Hemoglobin | 24.8 | pg | 27.5-33.2 |
| Platelet | 24.7×103 | /μL | 15.8-34.8×103 |
| Biochemistry | |||
| Total Protein | 7.2 | g/dL | 6.6-8.1 |
| Albumin | 4 | g/dL | 4.1-5.1 |
| Total Bilirubin | 0.2 | mg/dL | 0.4v1.5 |
| Aspartate Aminotransferase | 15 | IU/L | 13-30 |
| Alanine Transaminase | 11 | IU/L | 10-42 |
| Alkaline Phosphatase | 133 | U/L | 38-113 |
| Lactate Dehydrogenase | 182 | U/L | 124-222 |
| Glucose | 114 | mg/dL | 44-132 |
| Uric Acid | 4 | mg/dL | 73-109 |
| Urea Nitrogen | 21 | mg/dL | 73-109 |
| Creatinine | 0.8 | mg/dL | 0.65-1.07 |
| Estimated Glomerular Filtration Rate | 72 | mL/min/1.73 m2 | 90- |
| Sodium | 142 | mEq/L | 138-145 |
| Potassium | 4.4 | mEq/L | 3.6-4.8 |
| Chlorine | 105 | mEq/L | 101-108 |
| Calcium | 10.1 | mg/dL | 8.8-10.1 |
| Serology | |||
| C-reactive Protein | 0.42 | mg/dL | 0.00-0.14 |
| Prostate-Specific Antigen | 0.464 | ng/mL | 0.0-4.0 |
| Hematology | |||
| Parameter | Patient Value | Unit | Reference Range |
| WBC | 11300 | /μL | 3300-8600 |
| Neutrophils | 84.5 | % | 38-68 |
| Lympocytes | 9.1 | % | 27-47 |
| Monocytes | 6.3 | % | 2.0-8.0 |
| Eosinophils | 0 | % | 2.0-8.0 |
| Basophils | 0.1 | % | 0.0-7.0 |
| RBC | 3.94×106 | /μL | 4.35-5.55×106 |
| Hb | 9.6 | g/dL | 13.7-16.8 |
| HCT | 31.2 | % | 40.7-50.1 |
| MCV | 79.2 | fL | 83.6-98.2 |
| MCH | 24.4 | pg | 27.5-33.2 |
| Platelet | 23.9×103 | /μL | 15.8-34.8×103 |
| Biochemistry | |||
| TP | 6.5 | g/dL | 6.6-8.1 |
| Alb | 2.8 | g/dL | 4.1-5.1 |
| T-BIL | 0.4 | mg/dL | 0.4-1.5 |
| AST | 19 | IU/L | 13-30 |
| ALT | 19 | IU/L | 10-42 |
| ALP | 114 | U/L | 38-113 |
| LDH | 159 | U/L | 124-222 |
| GLU | 79 | mg/dL | 44-132 |
| UA | 2.4 | mg/dL | 73-109 |
| UN | 15 | mg/dL | 73-109 |
| Cre | 0.82 | mg/dL | 0.65-1.07 |
| eGFR | 70.1 | mL/min/1.73m2 | 90- |
| Na | 138 | mEq/L | 138-145 |
| K | 4.2 | mEq/L | 3.6-4.8 |
| Cl | 103 | mEq/L | 101-108 |
| Ca | 8.3 | mg/dL | 8.8-10.1 |
| Fe | 15 | μg/dL | 40-188 |
| UIBC | 175 | μg/dL | 168-252 |
| TIBC | 190 | μg/dL | 222-433 |
| Ferritin | 627.4 | ng/mL | 21.8-274.7 |
| Coagulation | |||
| PT | 15.1 | sec | 9.8-12.5 |
| PT-INR | 1.35 | 0.9-1.1 | |
| APTT | 34.4 | sec | 30.0-40.0 |
| FDP | 1.1 | μg/mL | 0.0-5.0 |
| D-dimer | 4.7 | μg/mL | 0.0-1.0 |
| Serology | |||
| CRP | 27.33 | mg/dL | 0.00-0.14 |
| PCT | 0.27 | ng/mL | 0.00-0.05 |
| C3 | 163 | mg/dL | 73-138 |
| C4 | 37 | mg/dL | 11-31 |
| IgG | 1007 | mg/dL | 861-1747 |
| IgG4 | 26 | mg/dL | 11-121 |
| IgA | 554 | mg/dL | 93-393 |
| IgM | 46 | mg/dL | 33-183 |
| ANA | <40 | 0-39 | |
| Anti-Jo-1 Antibody | <0.3 | U/mL | 0.0-6.9 |
| Anti-RNP Antibody | 3.1 | U/mL | 0.0-3.5 |
| Anti-Sm Antibody | <0.7 | U/mL | 0.0-7.0 |
| Anti-Scl-70 Antibody | 0.7 | U/mL | 0.0-7.0 |
| Anti-SS-A/La Antibody | 1.7 | U/mL | 0.0-7.0 |
| Anti-SS-B/La Antibody | <0.4 | U/mL | 0.0-6.9 |
| Anti-dsDNA Antibody | 2 | IU/mL | 0-10 |
| Anti-ssDNA Antibody | 3 | U/mL | 0-7 |
| Anti-Cardiolipin Antibody | <4.0 | U/mL | 0.0-12.3 |
| MPO-ANCA | <0.2 | IU/mL | 0.0-3.4 |
| PR3-ANCA | <0.5 | IU/mL | 0.0-2.0 |
| Anti-CCP Antibody | <0.5 | U/mL | 0.0-4.4 |
| Urinalysis | |||
| pH | 6 | 5.5-7.5 | |
| Protein | ( - ) | ( - ) | |
| Glucose | ( - ) | ( - ) | |
| RBC | 20-29 | /HPF | ( - ) |
| WBC | 10-19 | /HPF | ( - ) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Infective Endocarditis Diagnosis and Management · Neutrophil, Myeloperoxidase and Oxidative Mechanisms
Introduction
This report details a rare case of extensive aortitis associated with granulocyte colony-stimulating factor (G-CSF) administration in an older male patient. Given the life-threatening nature of aortitis and its risk of aortic dissection, early diagnosis is paramount [1,2]. To underscore the critical importance of prompt diagnosis and to disseminate knowledge about its diagnostic approaches across various medical specialties, we present this case report. This report is particularly significant due to the rarity of reported cases of G-CSF-induced aortitis in older male cancer patients.
Case presentation
The patient, a 74-year-old male with a history of localized prostate cancer treated with bicalutamide and androgen deprivation therapy 10 years prior, presented with a gradual elevation in prostate-specific antigen (PSA) levels (0.066 ng/mL) and subsequent pulmonary metastases. A bronchoscopic lung biopsy confirmed adenocarcinoma, with PSA levels further escalating to 0.156 ng/mL. The treatment regimen was altered to enzalutamide; however, PSA levels remained elevated, and progressive pulmonary metastases and new bone metastases were observed. Consequently, the elevated PSA level indicated systemic metastasis, leading to the patient's admission for docetaxel induction therapy for castration-resistant prostate cancer with pulmonary and bone metastases. His medical history was notable for diabetes mellitus, hyperlipidemia, and stable angina pectoris (post-catheterization), all managed pharmacologically. Admission blood tests revealed no significant abnormalities beyond elevated PSA levels (Table 1).
Docetaxel (70 mg/m²) and prednisolone (PSL, 5 mg) were initiated. Grade 3 neutropenia was observed on day 7 post-treatment initiation, prompting the administration of filgrastim (75 μg). The patient developed febrile neutropenia (FN) on day 9, which resolved with cefepime (2 g every 12 hours). Filgrastim was discontinued on day 12 following neutrophil recovery. However, the patient experienced recurrent fever on day 16 (Figure 1), accompanied by elevated inflammatory markers (WBC 10,700/μL, CRP 28.2 mg/dL).
Clinical course leading to the diagnosis of aortitis.Docetaxel (70 mg/m²) and PSL (5 mg) were initiated. On day 7 post-treatment initiation, grade 3 neutropenia was observed, prompting the administration of filgrastim (75 μg). The patient developed FN on day 9, which resolved with cefepime (2 g every 12 hours). Filgrastim was discontinued on day 12 following neutrophil recovery. However, the patient experienced recurrent fever on day 16, accompanied by elevated inflammatory markers (WBC 10,700/μL, CRP 28.2 mg/dL).WBC, white blood cell; CRP, C-reactive protein; CFPM, cefepime; TAZ/PIPC, tazobactam/piperacillin; PSL, prednisolone; FN, febrile neutropenia
CT scans revealed no apparent infectious source, and tazobactam/piperacillin was initiated following blood culture collection. Despite this, the patient remained febrile, and inflammatory markers persisted at elevated levels (Table 2). This blood sample was collected on day 16 after the initiation of chemotherapy.
A contrast-enhanced CT on day 19, performed for fever source localization, revealed circumferential wall thickening of the common carotid artery to the aortic arch and abdominal aorta (Figure 2).
(A) Contrast-enhanced CT at diagnosis: a horizontal view. (B) Contrast-enhanced CT at diagnosis: a sagittal view.(A) This figure shows a horizontal view from a contrast-enhanced CT scan performed on day 19 after docetaxel initiation to identify the fever source, revealing extensive circumferential wall thickening from the common carotid artery to the aortic arch and abdominal aorta. (B) This figure displays a sagittal view. Yellow arrows indicate the extent of aortic inflammation at the time of aortitis diagnosis. Red arrows are used to compare the aortic wall thickness.
Given the absence of bacterial growth in blood cultures and the patient's refractoriness to antibiotics, an infectious etiology was deemed improbable. Furthermore, the low epidemiological likelihood of Takayasu arteritis or giant cell arteritis led to the suspicion of drug-induced vasculitis, specifically G-CSF-associated vasculitis. PSL (60 mg, 1 mg/kg/day) was initiated. Moreover, IgG4-related periaortitis was deemed unlikely due to the lack of elevated IgG4. The patient's autoantibody profile was negative (Table 2), consistent with drug-induced vasculitis. Although some test results were near the upper limit of normal, the symptoms were nonspecific and not considered diagnostic. Following steroid initiation, the patient's fever resolved, inflammatory markers decreased, and overall clinical status improved (Figure 3).
Clinical course following initiation of steroid therapy.After the commencement of steroid treatment, the patient's fever resolved, inflammatory markers decreased, and overall clinical condition improved. PSL was tapered to 10 mg over two weeks, and the patient was discharged on day 32 without a recurrence of fever or elevated inflammatory markers.WBC, white blood cell; CRP, C-reactive protein; TAZ/PIPC, tazobactam/piperacillin; PSL, prednisolone
As continued high-dose steroid therapy was undesirable, we aimed for steroid dose reduction. PSL was tapered to 10 mg over two weeks, and the patient was discharged on day 32 without a recurrence of fever or elevated inflammatory markers. A follow-up contrast-enhanced CT on day 39 showed a reduction in aortic wall thickening (Figure 4).
(A) Progression of findings on contrast-enhanced CT: a horizontal view. (B) Progression of findings on contrast-enhanced CT: a sagittal view. (A) A subsequent CT scan post-third docetaxel cycle (day 39 from initial docetaxel) demonstrated sustained reduction of aortic wall thickening. (B) This figure displays a sagittal view. Red arrows are used to compare the aortic wall thickness.
The second docetaxel cycle was initiated with PSL maintained at 10 mg and docetaxel reduced to 55 mg/m². A subsequent CT scan post-third docetaxel cycle demonstrated a sustained reduction of aortic wall thickening. In this case, three chemotherapy cycles were completed through increased steroid dosage (5 mg to 10 mg), reduced docetaxel dosage, and prophylactic antibiotic administration for FN. Aortitis has not been confirmed for seven months following that event. Unfortunately, docetaxel was later discontinued due to a lack of therapeutic efficacy in treating the cancer. However, blood tests and other monitoring continue to be performed regularly to rule out any recurrence of aortitis.
Discussion
This case report describes a patient who developed G-CSF-associated aortitis during chemotherapy but subsequently completed three additional cycles without a recurrence of vasculitis. While we initially considered a risk of G-CSF-associated aortitis recurrence if docetaxel had been continued without dose reduction, the successful completion of chemotherapy without vasculitis relapse was ultimately achieved by co-administering PSL with docetaxel and reducing the docetaxel dose to 55 mg/m² in the second cycle.
Although cabazitaxel would typically be the next treatment course after docetaxel, we determined that administering cabazitaxel without concurrent G-CSF would be risky due to its higher risk of FN compared to docetaxel. Discussions regarding alternative options to filgrastim for recurrent neutropenia are also necessary. In such cases, prophylactic levofloxacin may be recommended for persistent neutropenia below 100/µL. We believe this case report will be valuable for many clinicians involved in the future management of patients who develop aortitis during chemotherapy, especially internists, oncologists, and other physicians in cancer-related specialties, general internists managing fevers of unknown origin, and geriatricians caring for various conditions in older adults.
Aortitis should be included in the differential diagnosis in patients presenting with fever and inflammation following G-CSF administration. While G-CSF-associated vasculitis is more commonly reported in females, breast cancer cases, and those with other gynecological conditions [3], this case highlights the occurrence of G-CSF-associated vasculitis in older males. A review of the extant literature indicates that the incidence of G-CSF-associated vasculitis ranges from 0.4% to 2.7% [4-6]. However, subsequent reports, including this case, on prostate and bladder cancer patients not featured in those original studies indicate that this vasculitis may manifest across a broader spectrum of age, gender, and cancer types than previously recognized. Cases of G-CSF-associated aortitis in older patients, specifically those with bladder and prostate cancer, have only recently started to be reported [7,8]. In cancer patients, particularly older individuals, fever evaluation can be challenging due to nonspecific symptoms. Furthermore, secondary aortitis may be asymptomatic despite progressive vascular inflammation. This case underscores the importance of considering G-CSF-associated aortitis in older males and the necessity for prompt contrast-enhanced CT imaging when G-CSF-associated vasculitis is suspected. The clinical lesson from this case is that aortitis should be considered a complication in any cancer treatment, and if suspected, contrast-enhanced CT should be performed immediately.
Conclusions
This case report clearly delineated the disease characteristics and treatment approaches that were crucial for healthcare professionals managing cancer and those investigating fevers of unknown origin. This case report, by detailing the clinical course of an older male patient and referencing prior literature, contributes to the understanding that aortitis, previously considered more prevalent in gynecological oncology patients receiving chemotherapy, must now be considered in the differential diagnosis for malignancies occurring in older men.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aortitis Vascul Pharmacol Bossone E Pluchinotta FR Andreas M 1108020162672121310.1016/j.vph.2015.11.084 · doi ↗ · pubmed ↗
- 2Thoracic aortitis and aortic dissection following pegfilgrastim administration Eur J Cardiothorac Surg Sato Y Kaji S Ueda H Tomii K 9939945220172854911010.1093/ejcts/ezx 165 · doi ↗ · pubmed ↗
- 3Literature review analysis of aortitis induced by granulocyte-colony stimulating factor Front Pharmacol Zhao T Xu H 14875011520243974413610.3389/fphar.2024.1487501 PMC 11688214 · doi ↗ · pubmed ↗
- 4The incidence and clinical features of PE Gylated filgrastim-induced acute aortitis in patients with breast cancer Sci Rep Lee SY Kim EK Kim JY 186471020203312266210.1038/s 41598-020-75620-6PMC 7596224 · doi ↗ · pubmed ↗
- 5Granulocyte colony-stimulating factor-associated aortitis unveiled by 18 F-FDG PET/CT Clin Nucl Med Artigou H Foka Tichoue H Marques C Charlotte F Vion PA Kas A Rozenblum L 0350202510.1097/RLU.000000000000558039690506 · doi ↗ · pubmed ↗
- 6Single-center analysis of pegfilgrastim-induced aortitis using a drug prescription database and CT findings Radiology Takamatsu A Yoshida K Toshima F Kozaka K Yamamoto N Sai Y Gabata T 72974030520223594333510.1148/radiol.220357 · doi ↗ · pubmed ↗
- 7A case of granulocyte colony-stimulating factor-related aortitis that developed during the treatment of advanced prostate cancer with neuroendocrine differentiation Hinyokika Kiyo Hazama T Maruno K Takahashi T 1791837020243896703110.14989/Acta Urol Jap_70_6_179 · doi ↗ · pubmed ↗
- 8Granulocyte colony-stimulating factor-induced aortitis with temporal arteritis and monoarthritis BMJ Case Rep Iida K Honda Y Homma Y 16202310.1136/bcr-2022-251216 PMC 990627436750306 · doi ↗ · pubmed ↗