Reducing Physician Burnout Through Workflow Redesign: A Quality-Improvement Initiative
Jennifer Goebel, Jessica Sidle, Alma Aspiras, Leah Fow, Molly McCann-Pineo, Timmy Li

TL;DR
This paper shows how redesigning a specific paperwork task reduced physician burnout and improved workflow efficiency at a hospital.
Contribution
The study demonstrates a practical workflow redesign approach to reduce physician burnout through interdisciplinary collaboration and targeted administrative task redistribution.
Findings
76% of hospitalists reported reduced workload after removing the 3122 form from their tasks.
The intervention improved efficiency and reduced transcription errors by using EMR-generated materials.
Interdisciplinary collaboration was key to designing a sustainable solution for clinician well-being.
Abstract
Introduction Staff well-being is a critical element in any healthcare organization’s framework. Improving provider and staff well-being is increasingly recognized as essential to high-quality care. Burnout among healthcare workers is often driven by excessive administrative demands, inefficient workflows, and time-consuming clerical tasks. These burdens take time away from meaningful patient interactions and clinical decision-making. At Huntington Hospital, clerical workload, especially tasks related to electronic health records (EHRs) and manual documentation, was identified as a key source of stress. To better understand the contributors to burnout, the hospital administered the Maslach Burnout Inventory (MBI) to all hospitalists. The MBI evaluates emotional exhaustion, depersonalization, and reduced personal accomplishment, offering a comprehensive assessment of professional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
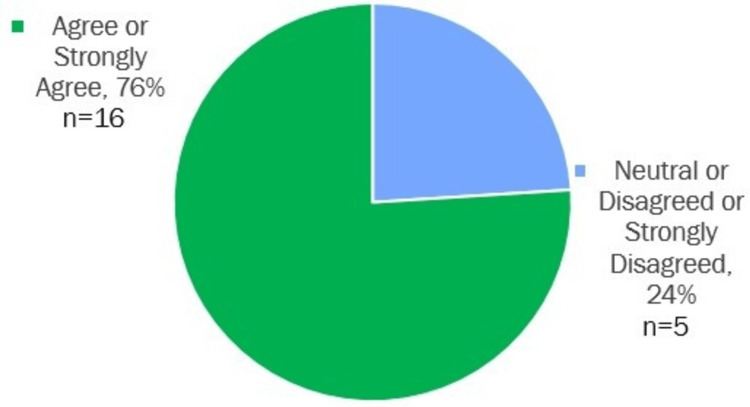 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Quality and Management · Patient Safety and Medication Errors · Innovations in Medical Education
Introduction
Staff well-being is a critical element in any organization’s framework, particularly in healthcare settings. The Quadruple Aim, a key healthcare delivery framework, emphasizes improving provider and staff well-being as one of its core pillars [1].
The 2022 U.S. Surgeon General’s advisory Addressing Health Worker Burnout underscored the need for a comprehensive societal approach to addressing burnout. It called for reducing administrative duties, focusing on human-centered health technology, and redesigning payment models to value provider-patient interactions. The advisory emphasized that providers currently spend two hours on clerical tasks for every hour spent with patients [2]. Similarly, the National Academy of Medicine highlighted the importance of streamlining workflows and minimizing manual tasks to allow physicians to engage in meaningful, focused care, often referred to as "deep work." Evidence suggests that re-engineering workflows and implementing team-based care models could reduce burnout, enhance provider well-being, and restore more time for direct patient care [2,3].
Clerical burdens, particularly those tied to electronic health records (EHRs), have been identified as the leading cause of burnout [4]. A study by DiGiorgio et al. revealed that residents spent up to 20 hours per on-call shift interacting with EHRs, with nine of those hours spent on clerical tasks instead of patient care [5]. This highlights the need for improving workflow efficiency and reducing administrative burdens to combat burnout and enhance physician well-being.
To better understand the drivers of burnout among hospital staff, Huntington Hospital distributed the Maslach Burnout Inventory (MBI) to all its hospitalists. The MBI is one of the most widely used tools for measuring burnout in healthcare providers. It assesses three key dimensions of burnout: 1) emotional exhaustion, 2) depersonalization, and 3) reduced personal accomplishment. Emotional exhaustion refers to the feeling of being overextended and drained of emotional resources, while depersonalization involves a sense of cynicism or detachment from patients [6]. Reduced personal accomplishment refers to the feeling of incompetence and a lack of achievement in one’s work. The MBI provides a detailed snapshot of how healthcare professionals are coping with the emotional and psychological demands of their work [7].
Materials and methods
A multi-disciplinary wellness learning community was established at our hospital to create evidence-based practices that best support staff well-being. Knowing that the number one driver of burnout was workload in our hospitalist group, the hospitalists unanimously wanted to tackle the workflow process of the 3122 form (Return to Assisted Living Medical Evaluation Form). Previously, hospitalists were required to complete this handwritten form for each patient discharged to an assisted living facility, taking them away from direct patient care. This form includes the patient’s diagnoses, handwritten medications requisition, allergies, mental status, Activities of Daily Living (ADLs), necessary therapies, and home care needs. The objective was to reduce this administrative burden, allowing hospitalists to focus more on their core responsibilities and patient interactions. Discussions were held with our social work and case management teams, as well as with similar groups at neighboring hospitals in the same system, to understand their workflows regarding this form.
After several multi-disciplinary meetings, the decision was made to streamline the process by assigning responsibility for the form to the social work team. This was decided because the form included questions about ADLs and other areas that are within their scope of practice. Medications, previously handwritten by hospitalist staff, were printed from the electronic medical record (EMR) and attached to the form, aligning with practices at other hospitals and improving patient safety while reducing staff workload. By printing medication information directly from the EMR, the hospital also aimed to reduce transcription errors and improve the accuracy of patient data. Hospitalists would then review the form before it was sent to assisted living facilities. The revised workflow was piloted on one floor, and even before the pilot was complete, other hospitalists expressed interest in adopting the process on their own floors.
Results
The MBI was sent out to our hospitalist physicians at our large community hospital, and with a 83% response rate (33 out of 40 hospitalists), the results revealed that workload was the primary driver of burnout.
A two-question post-implementation survey was conducted with the hospitalist group, asking them to rate the following statements: "Removing the 3122 form as a physician task has decreased my workload burden" (Figure 1) and "I recommend partnering with the Wellness Learning Community for further process changes and program development." The results were overwhelmingly positive.
Removing the 3122 form as a physician task has decreased my workload burden
76% respondents either agreed or strongly agreed that removing the 3122 form as a physician task reduced their workload, and 76% (n=21) recommended continued collaboration with the Wellness Learning Community for further process improvements and program creation.
Discussion
This project incorporated several key components that improved workflow and enhanced healthcare providers' well-being. By streamlining administrative tasks and minimizing unnecessary burdens, the initiative enabled providers to devote more time and attention to direct patient care-an essential part of their roles.
One critical focus of the project was fostering interprofessional collaboration. By involving teams from social work, case management, and other key stakeholders, the hospital developed a more efficient and effective workflow. This teamwork-driven approach is vital for improving patient care outcomes, as research consistently shows that collaboration leads to safer and higher-quality care [8].
Research also underscores the importance of healthcare providers' physical and mental well-being in reducing medical errors. For example, a 2021 study published in the American Journal of Critical Care found that critical-care nurses in better health, working in organizations prioritizing employee wellness, reported fewer medical errors [9] . Similarly, a 2022 Healthcare Executive article, "The Secret to Safer Patients: Workforce Wellness," emphasized the direct link between workforce wellness and patient safety [10]. This connection was reinforced by the Minimizing Error, Maximizing Outcome study funded by the Agency for Healthcare Research and Quality, which revealed that physician stress and burnout were linked to a higher likelihood of medical errors [11].
The redesign of the workflow process for the 3122 form reduced both administrative workload and error risks. These changes allowed hospitalists to focus more on patient care, improving both staff well-being and patient safety [12]. The impact of illegible handwriting on medical errors is well-documented. The Institute of Medicine (IoM) estimated that medical errors cause 44,000 to 98,000 preventable deaths annually in the U.S., with approximately 7,000 attributed to illegible handwriting [13]. Transitioning to electronic prescriptions has been shown to mitigate these errors, improving both safety and efficiency [14].
While this project specifically addressed the 3122 form, its principles of workflow optimization and burden reduction can be applied across various healthcare settings. It demonstrates how improving administrative processes can relieve provider workload, enabling a greater focus on patient care [15]. Integrating wellness initiatives into quality improvement efforts enhances both provider well-being and patient safety, fostering a healthier work environment and better outcomes for patients [16].
There are some limitations to this initiative. This initiative was conducted at a single community hospital with a relatively small sample size, limiting the generalizability of the findings. The assessment occurred shortly after implementation, so the long-term impact on workload and burnout remains unknown. Additionally, the results were based on self-reported survey responses, which are inherently subjective and may not fully reflect objective changes in workflow or burden. While the intervention aimed to reduce transcription-related medical errors, no direct measurement of patient safety outcomes was conducted.
Conclusions
This project demonstrates the powerful impact of targeting specific, modifiable workflow inefficiencies as a means of supporting clinician well-being. Rather than relying solely on wellness programs that focus on self-care or resilience, this intervention addressed one of the root causes of burnout: administrative overload. By listening to frontline hospitalists and identifying a concrete, high-friction task, the team was able to develop a practical, sustainable solution that directly improved physicians’ daily experience.
The collaborative nature of this project was central to its success. Engaging social work, case management, and hospital leadership allowed for a more efficient redistribution of tasks, aligning responsibilities with appropriate scopes of practice. This kind of interprofessional teamwork not only lightens the load for individual clinicians but also improves overall system efficiency and safety. Importantly, the positive response from hospitalists following the intervention points to a readiness for more of these changes. Providers want to be part of system improvement; they often just need a framework and a forum in which to participate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2023 Mayo Clin Proc Shanafelt TD West CP Sinsky C 117202510.1016/j.mayocp.2024.11.03140202475 · doi ↗ · pubmed ↗
- 2Health worker burnout 2 2025 https://www.hhs.gov/surgeongeneral/priorities/health-worker-burnout/index.html
- 3Taking action against clinician burnout: a systems approach to professional well-being National Academies of Sciences Engineering Engineering and Medicine 2019 Washington, DC The National Academies Press Washington, DC 201931940160 · pubmed ↗
- 4Maslach Burnout Inventory-ES form (MBI)APA Psyc Tests Maslach C Jackson SE 1981
- 5Death by 10,000 Clicks: The Electronic Health Record 5 2025 2023 https://www.medpagetoday.com/opinion/second-opinions/102722
- 6The measurement of experienced burnout J Organ Behav Maslach C Jackson SE 9911321981
- 7Teamwork in healthcare: key discoveries enabling safer, high-quality care Am Psychol Rosen MA Diaz Granados D Dietz AS Benishek LE Thompson D Pronovost PJ Weaver SJ 4334507320182979245910.1037/amp 0000298 PMC 6361117 · doi ↗ · pubmed ↗
- 8Well-being, work environment affect medical errors 2 2025 American Association of Critical-Care Nurses.(2021 2021 https://www.aacn.org/newsroom/well-being-work-environment-affect-medical-errors