Complex Hepatic Abscess in a Child Following Esophageal Procedures: Clinical Insights and Management
Jack Hachem, Anthoula Christodoulou, William Hunt, John Manaloor, Javier J Monagas

TL;DR
A child developed a rare liver infection after esophageal procedures, highlighting the need for infection prevention in similar cases.
Contribution
This case report highlights the risk of hepatic abscesses following esophageal interventions in children and suggests the need for prophylactic antibiotics.
Findings
A five-year-old girl developed a complex hepatic abscess after multiple esophageal interventions.
Bacterial translocation from oral cavity organisms was suspected as the cause of the abscess.
Antibiotic management and source control were necessary for recovery.
Abstract
This case report describes a rare occurrence of a hepatic abscess in a five-year-old girl following esophageal interventions due to caustic ingestion. Persistent strictures led to multiple balloon dilations and serial esophageal stents, after which she developed abdominal pain, fever, and anorexia. Imaging revealed a complex hepatic abscess. Cultures identified Eikenella corrodens and Prevotella oralis, organisms typically found in the oral cavity, suggesting bacterial translocation due to mucosal disruption from the esophageal procedures. The patient initially received ceftriaxone and metronidazole, showing improvement, but experienced fever recurrence upon switching to ampicillin/sulbactam, necessitating a return to the original antibiotic regimen. The patient eventually recovered with continued treatment, highlighting the risk of serious infections following esophageal interventions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
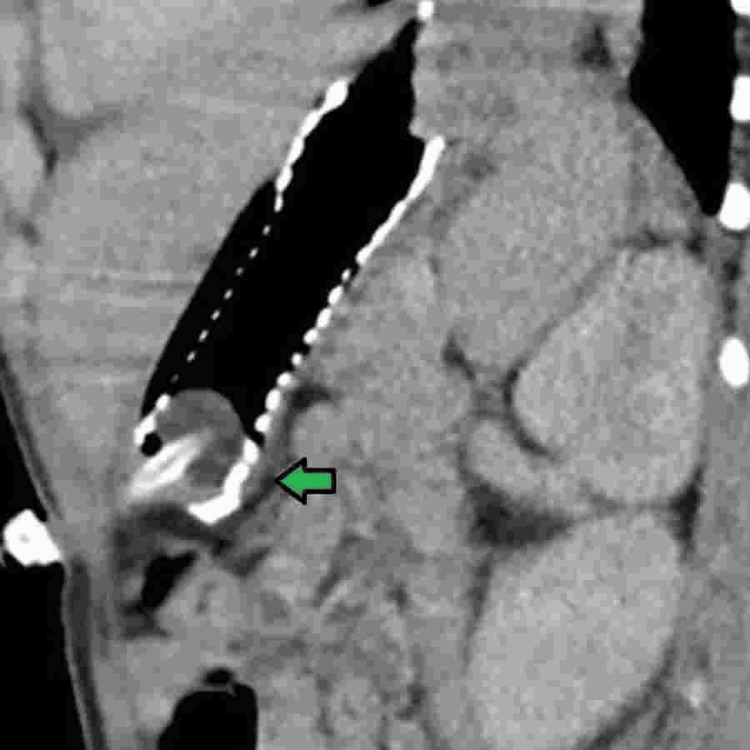 Figure 1
Figure 1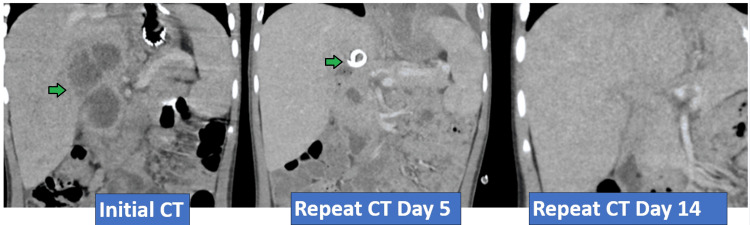 Figure 2
Figure 2| Lab Test | Result | Reference Range |
| White blood cell (WBC) count | 20,000 | 4,500-11,000 cells/mm3 |
| Hemoglobin | 8.1 | 12.5-16.5 g/dL |
| Platelet count | 483,000 | 150,000-450,000/mm3 |
| Sodium | 145 | 136-146 mEq/L |
| Potassium | 3.91 | 3.5-5 mEq/L |
| Chloride | 101 | 95-105 mEq/L |
| Bicarbonate | 20 | 22-28 mEq/L |
| Albumin | 2.7 | 3.3-4.5 g/dL |
| C-reactive protein (CRP) | 37.8 | <0.50 mg/dL |
| Erythrocyte sedimentation rate (ESR) | >145 | 0-10 mm/hr |
| Procalcitonin | 0.68 | 0-0.5 ng/mL |
| Alanine transaminase (ALT) | 100 | 10-33 U/L |
| Aspartate aminotransferase (AST) | 67 | 10-33 U/L |
| Bilirubin total | 0.4 | 0.1-1 mg/dL |
| PT | 14.4 | 12.3-15.1 sec |
| PTT | 48 | 24.5-36.1 sec |
| Lipase | 5 | 8-78 U/L |
| Case | Age/Sex | Causes of Mucosal Compromise | Clinical Presentation | Identified Organism | Anti-infective Therapy |
| Lopez-Tobaruela et al. (2021) [ | 55 y/o F | Multiple bougie/balloon dilations and stent placement | Fever to 102°F. Chest and epigastric pain radiating to the right hypochondrium. Leukocytosis (13,630 cells/µL). Elevated CRP (20.9 mg/dL). | Streptococcus intermedius | Levofloxacin |
| Cirimele et al. (2023) [ | 31 y/o F | Endoscopic sleeve gastroplasty | Two-day history of fever up to 102°F, epigastric pain two weeks after endoscopic sleeve gastroplasty. Leukocytosis and elevated C-reactive protein levels. | Streptococcus intermedius | Cefotaxime, gentamicin |
| Kessler and Kourtis (2001) [ | 53 y/o M | Impacted fish bone | Four-week history of abdominal pain and a tender right upper quadrant mass. Leukocytosis (8,100 cells/µL). | Eikenella corrodens | Vancomycin, piperacillin-tazobactam |
| This study | 5 y/o F | Multiple balloon dilations and stent exchange in a neoesophagus | Three-day history of progressive abdominal pain, fevers up to 102°F, anorexia, and weight loss two weeks post-esophageal stent placement. Leukocytosis (20,000 cells/µL), elevated procalcitonin (0.69 mg/dL), and elevated C-reactive protein levels (37.8 mg/dL). |
| Ceftriaxone, metronidazole, amoxicillin-clavulanate |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
Introduction
Esophageal strictures resulting from caustic ingestions often necessitate endoscopic and surgical interventions. When endoscopic dilatation fails or in cases of long segment strictures, severe caustic injuries, or recurrent strictures, esophageal replacement becomes a critical option. One surgical technique employed is the reversed gastric tube esophagoplasty. This procedure involves isolating a segment of the stomach, which is then fashioned into a tube while preserving its blood supply. This newly formed tube is anastomosed to both the remaining esophagus and stomach, effectively bypassing the damaged or absent esophageal segment. The reversed orientation of the gastric tube aids in maintaining peristalsis and facilitating normal swallowing.
Despite its benefits, stricture formation is a relatively common complication in approximately 30% of esophageal reconstruction surgeries involving gastric tubes [1]. Managing these strictures is challenging and may lead to complications such as perforations, fistulas, and infections. Endoscopic and surgical interventions, such as balloon dilation or gastroplasty, can disrupt the gastroesophageal mucosal barrier, potentially facilitating bacterial translocation into the local venous circulation. There have been documented cases of complicated hepatic abscesses arising from esophageal procedures [2-6]. In this paper, we present a case involving a five-year-old patient who developed a complex hepatic abscess secondary to esophageal interventions. This case highlights the potential complications and challenges associated with treating esophageal strictures in pediatric patients.
Case presentation
A five-year-old girl with a history of ingestion of a caustic cleaning agent at one year of age underwent a reverse gastric sleeve reconstruction after failing multiple esophageal dilations. Post-surgery, she continued to experience recurrent strictures at the anastomotic site, necessitating further esophageal balloon dilations and ultimately the placement of a fully covered esophageal metal stent. This intervention led to transient improvement, allowing her to tolerate a soft mechanical diet. However, approximately two weeks after the stent placement, she began experiencing progressive abdominal pain, fevers, with a maximum temperature of 102°F, and anorexia with weight loss. She was taken to urgent care and was found to have an elevated white blood cell count (WBC) of 20,000 cells/mm^3^ as well as elevated transaminases, prompting transfer to our emergency department. Upon examination, the patient was febrile, appeared sickly, and was pallorous, with no signs of jaundice or icterus. The abdominal exam was notable for right upper quadrant tenderness and an increased liver span, measuring 2 cm below the costal margin. Additional labs at our hospital showed an elevated CRP at 37.84 mg/dL, an ESR of 93 mm/hr, and a procalcitonin level of 0.68 ng/mL (Table 1). Blood cultures, GI pathogen polymerase chain reaction (PCR) panel, and Entamoeba histolytica antigen tests were obtained and later found to be negative. A chest radiograph revealed interval migration of the esophageal stent, with the distal portion wrapped around the gastrostomy balloon (Figure 1).
Radiograph image of stent migration to the stomach, with the distal portion wrapped around the gastrostomy balloon (green arrow).
Further imaging was obtained with IV and oral contrast computed tomography (CT) of the abdomen/pelvis, revealing a complex septated hepatic abscess at the hilum (4.1 x 3.8 x 4.6 cm). The patient was empirically started on parenteral antibiotics with ceftriaxone and metronidazole. The stent was successfully retrieved via the gastrostomy site. Interventional radiology placed an 8-French Cook percutaneous drain that remained in place for six days. Brown purulent fluid was drained and sent for aerobic and anaerobic cultures. The Gram stain of the fluid showed many polymorphonuclear leukocytes and heavy growth of gram-negative rods, later revealed to be Eikenella corrodens and Prevotella oralis. 16S Next-Generation Sequencing (NGS) results confirmed abundant Prevotella loescheii and moderate Prevotella oralis presence. Fungal and acid-fast bacteria (AFB) stains were negative. Repeat labs revealed a decrease in WBC count from 20,000 to 15,300 cells/mm^3^ and CRP down to 15.5 mg/dL after three days of empiric antibiotics with Ceftriaxone and Metronidazole. Based on infectious disease recommendations, we switched to Ampicillin/Sulbactam to narrow the coverage, as it is effective monotherapy for Eikenella. However, this resulted in a recurrence of fever and a rebound of CRP to 25.5 mg/dL on day six of antibiotic therapy. The patient was switched back to parenteral ceftriaxone and oral metronidazole. The fever defervesced and repeated labs after eight days of antibiotic therapy improved with a WBC count of 8,400 cells/mm^3^ and a CRP of 11.39 mg/dL. The patient remained afebrile and completed an additional two weeks of parenteral ceftriaxone and PO metronidazole. WBC before discharge was 7,500 cells/mm^3^, and the CRP was 0.24 mg/dL. The patient was sent home on a six-month course of daily enteral antibiotic prophylaxis with amoxicillin-clavulanate. Repeat CT imaging at the end of therapy showed resolution of the abscess (Figure 2).
CT depiction of complex septated fluid collection in the hepatic hilum before and after intervention.Green arrow in initial CT and repeat CT day 5 indicates complex septated fluid collection in the hepatic hilum.
Discussion
Endoscopic and surgical procedures, such as endoscopic balloon dilation or gastroplasty, can be traumatic and disrupt the gastroesophageal mucosal barrier, potentially facilitating bacterial translocation into the local venous circulation. The incidence of bacteremia after esophageal reconstruction is up to 56% in the immediate postoperative period and range from 22% to 72% of cases involving repeated esophageal balloon dilation, particularly when the stricture is malignant [7-9]. Complicated infections, including brain abscesses, endocarditis, and meningitis, have been documented [2]. However, only a few cases of complicated hepatic abscesses related to esophageal procedures have been published. Lopez-Tobaruela et al. reported a 55-year-old woman who developed a hepatic abscess approximately two weeks after receiving a biodegradable esophageal stent for an upper esophageal stricture [3]. The mucosal tears from the esophageal dilations likely compromised mucosal integrity, allowing bacteria to enter the bloodstream and subsequently the liver. Similarly, Cirimele et al. described a 31-year-old who developed hepatic abscesses two to three weeks following endoscopic sleeve gastroplasty, and Kessler and Kourtis reported a 53-year-old with an impacted fishbone who developed a hepatic abscess four weeks after the initial insult [4-6]. To our knowledge, there are no pediatric cases for comparison. However, we believe these cases share a common theme of disruption to the gastroesophageal mucosal integrity, allowing oral bacteria to enter the gastroepiploic veins, subsequently seeding into the portal vein and extending to the hepatic hilum, where the bacteria localize into a complicated abscess. A comparison table of the currently published cases is provided in Table 2.
Eikenella corrodens is commonly part of the oral flora and is often associated with human bites. There is very little published literature implicating *Eikenella *in hepatic abscess infections. In the case reported by Kessler and Kourtis, it was presumed that the *Eikenella *organism was acquired from the patient's oral cavity, while he was eating fish [5]. Similarly, in our patient, during the initial endoscopic insertion, the endoscope could acquire Eikenella corrodens when it contacts the oral mucosa before entering the esophagus. *Eikenella *could then presumably be introduced through mucosal tears during dilation or stent therapy. This mechanism underscores the potential vulnerability of patients with invasive esophageal procedures.
Prevotella is also an integral part of the oral flora. Prevotella oralis is frequently found in subgingival plaque and is associated with periodontal disease, including gingivitis, periodontitis, and dentoalveolar abscesses [10]. It can also extend beyond its primary habitat in the oral cavity. Prevotella loescheii has been known to cause infections in prosthetic joints, such as total hip arthroplasty, likely due to hematogenous spread from oral sources. Prevotella oralis has been identified in systemic infections, notably in cases of bacteremia of hepatic origin, where it has been isolated from hepatic abscess drainage [11].
The onset of liver infection seems to occur several weeks following compromise to the mucosal barrier. Currently, no standard practice exists for administering prophylactic antibiotics to patients undergoing endoscopic therapies or surgeries that compromise the mucosal barrier. However, antibiotic prophylaxis in patients undergoing repeated endoscopic therapies, such as dilation, stent placement, or stent replacement, particularly those with esophageal reconstruction or who are immunocompromised, may be beneficial in managing these patients. This approach would be similar to antibiotic prophylaxis use in patients undergoing dental procedures that are high risk for bacteremia [12]. In general, an antibiotic effective against anaerobic organisms, such as Augmentin, should be considered. A second agent may be necessary to ensure broader spectrum coverage for all potential esophageal pathogens. It is advisable to consult with a clinical pharmacist, as clinical data on this topic is limited.
Conclusions
Our case is particularly unique due to the rare complication and the unusual organisms involved. Notably, no pediatric cases have been reported, nor have any cases involving Prevotella oralis. The implications of this case highlight the importance of considering antibiotic prophylaxis for patients undergoing frequent esophageal interventions. Prophylactic antibiotics could significantly reduce the risk of bacterial translocation and subsequent abscess formation. This approach is especially pertinent for pediatric patients with complex esophageal reconstructions, who are at increased risk for such complications. Ensuring appropriate antibiotic coverage during and after these procedures could help mitigate severe infections and improve patient outcomes.
While the risk of infection following endoscopic procedures is not universally acknowledged, the potential for serious complications such as hepatic abscess formation warrants consideration of prophylactic measures in high-risk patients. Further research and clinical guidelines are needed to establish protocols that can effectively prevent these rare but significant complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Early prediction of complex benign anastomotic stricture after esophagectomy using early postoperative endoscopic findings Surg Endosc Nishikawa K Fujita T Yuda M Tanaka Y Matsumoto A Tanishima Y Yanaga K 346034693420203157103310.1007/s 00464-019-07123-z · doi ↗ · pubmed ↗
- 2Hepatic abscess: diagnosis and management J Visc Surg Lardière-Deguelte S Ragot E Amroun K 23124315220152577074510.1016/j.jviscsurg.2015.01.013 · doi ↗ · pubmed ↗
- 3Hepatic abscess after biodegradable esophageal stent placement: a rare complication Am J Gastroenterol Lopez-Tobaruela JM Valverde-Lopez F Lopez de Hierro-Ruiz M Redondo-Cerezo E 22222311620213282657410.14309/ajg.0000000000000821 · doi ↗ · pubmed ↗
- 4Liver abscess after endoscopic sleeve gastroplasty: a case report Radiol Case Rep Cirimele V D'Amone G Vertulli D 418741901820233775350010.1016/j.radcr.2023.08.113PMC 10518679 · doi ↗ · pubmed ↗
- 5Liver abscess due to Eikenella corrodens from a fishbone N Engl J Med Kessler AT Kourtis AP 0345200110.1056/ENEJ Micm 01043311759661 · doi ↗ · pubmed ↗
- 6Hepatic abscess due to Eikenella corrodens and Streptococcus milleri: implications for antibiotic therapy J Infect Quinlivan D Davis TM Daly FJ Darragh H 4748331996884299510.1016/s 0163-4453(96)92776-0 · doi ↗ · pubmed ↗
- 7The detection of intraoperative bacterial translocation in the mesenteric lymph nodes is useful in predicting patients at high risk for postoperative infectious complications after esophagectomy Ann Surg Nishigaki E Abe T Yokoyama Y Fukaya M Asahara T Nomoto K Nagino M 47748425920142354942710.1097/SLA.0b 013e 31828 e 39e 8 · doi ↗ · pubmed ↗
- 8Bacteremia with esophageal dilation Gastrointest Endosc Nelson DB Sanderson SJ Azar MM 563567481998985244410.1016/s 0016-5107(98)70036-7 · doi ↗ · pubmed ↗