Robotic Stereotactic Body Radiation Therapy for High-Risk Prostate Cancer: The Georgetown University Experience
Vaibhav Sharma, Tim Kearney, Zach Lee, Padraig Brennan Pilkington, Marielle Fis Loperena, Malika Danner, Alan L Zwart, Deepak Kumar, Brian Collins, Michael Carrasquilla, Suy Simeng, Sean Collins

TL;DR
This study shows that robotic SBRT is a safe and effective treatment for high-risk prostate cancer, with good cancer control and minimal impact on quality of life.
Contribution
The study provides long-term quality of life and cancer control data for high-risk prostate cancer patients treated with robotic SBRT.
Findings
Three-year biochemical disease-free rate was 89% in high-risk prostate cancer patients treated with robotic SBRT.
Most recurrences were bone metastases, followed by PSA-only recurrences and local or lymph node involvement.
Quality of life scores remained largely stable or improved after treatment, with minimal clinically significant decline.
Abstract
Introduction Stereotactic body radiation therapy (SBRT) has emerged as a highly conformal and hypofractionated treatment modality, demonstrating safety and efficacy in low- and intermediate-risk prostate cancer (PCa). Traditionally, high-risk (HR) PCa has been managed with conventional fractionation external beam radiotherapy. Such extended treatment may be burdensome to elderly PCa patients. There is a dearth of long-term patient-reported outcome data for HR PCa patients treated with SBRT. This retrospective study examines cancer control and health-related quality of life (HRQOL) outcomes in HR PCa patients receiving robotic SBRT. Materials and methods HR PCa patients who underwent robotic SBRT treatment (7-7.25 Gy in five fractions over one to two weeks) from December 2008 to July 2023 were included in this retrospective analysis. Biochemical failure was defined according to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
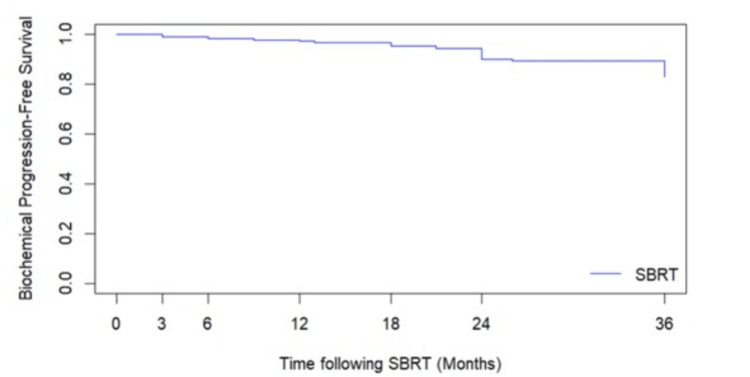 Figure 1
Figure 1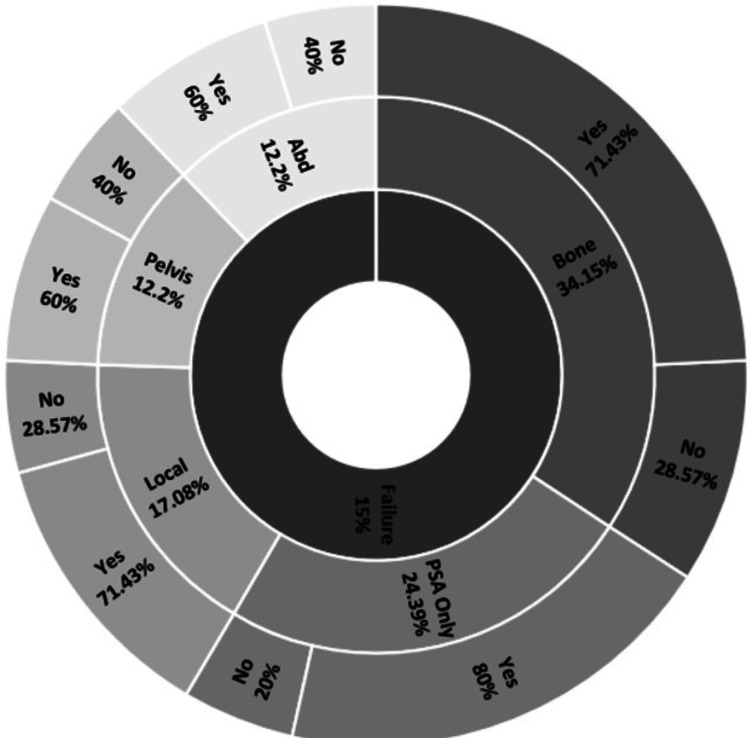 Figure 2
Figure 2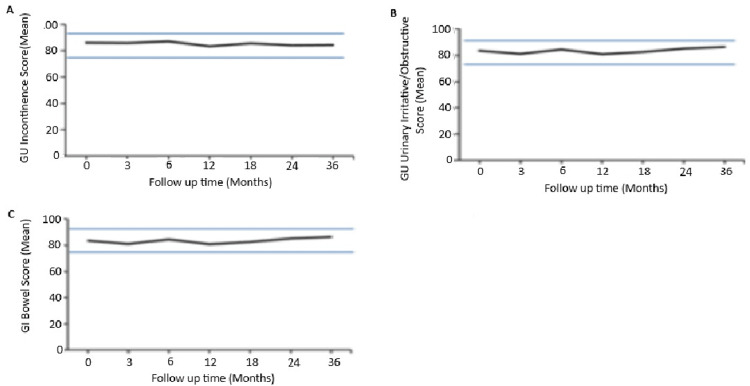 Figure 3
Figure 3| Domain | Patients (N=216) | Percent patient (%) | |
| Age | |||
| <60 | 7 | 3 | |
| 60-69 | 53 | 25 | |
| 70-79 | 84 | 39 | |
| >80 | 71 | 33 | |
| Race | |||
| White | 107 | 50 | |
| Black | 84 | 39 | |
| Hispanic | 4 | 2 | |
| Other | 21 | 10 | |
| Initial PSA | |||
| <10 | 82 | 38 | |
| 10-20 | 50 | 23 | |
| >20 | 84 | 39 | |
| Gleason score | |||
| 3 + 3 = 6 | 19 | 9 | |
| 3 + 4 = 7 | 26 | 12 | |
| 4 + 3 = 7 | 23 | 11 | |
| 4 + 4 = 8 | 101 | 47 | |
| 3 + 5 = 8 | 8 | 4 | |
| 4 + 5 = 9 | 37 | 17 | |
| 5 + 5 = 10 | 2 | 1 | |
| Dose | |||
| 35 Gy/5 fx | 38 | 18 | |
| 35.5 Gy/5 fx | 2 | 1 | |
| 36.25 Gy/5 fx | 176 | 81 | |
| Hormone | |||
| Yes | 156 | 75 | |
| No | 51 | 25 | |
| Average (range) | |
| PSA ng/ml | |
| Initial | 22.9 (1.3-6) |
| Nadir | 1.82 (0.1-34) |
| Recurrence | 22.03 (0.39-429.8) |
| Time to failure (months) | 40 (3-131) |
| Percent patients N (%) | |
| Gleason score | |
| G6 | 1 (3%) |
| G7 | 8 (24%) |
| G8 | 12 (36%) |
| G9 | 12 (36%) |
| Dose (Gy) | |
| 35 | 6 (18%) |
| 36.25 | 27 (82%) |
| DRE | |
| Abnormal | 18 (55%) |
| Normal | 15 (45%) |
| Pattern of failure | |
| Bone | 11 (34.15%) |
| Local | 6 (17.08%) |
| PSA only | 8 (24.39%) |
| Abdomen | 4 (12.2%) |
| Pelvis | 4 (12.2%) |
| ID | iPSA | Stage | Gleason | Staging imaging | Dose | ADT | PSA nadir | Time to failure | PSA recurrence | DRE | Recurrence imaging | Pattern of failure | Radiotherapy |
| 1 | 50 | T3a | G7 | BS, MRI | 36.25 | Y | 0.1 | 24 | 5.6 | Abnormal | BS, CT | Abd | N |
| 2 | 20 | T2c | G9 | MRI | 35 | N | 1.7 | 36 | 3.8 | - | - | PSA only | N |
| 3 | 31.8 | T2a | G6 | BS, CT, MRI | 36.25 | Y | 0.6 | 24 | 3.9 | Normal | BS | Bone | Curative |
| 4 | 32.5 | T1c | G7 | MRI | 36.25 | N | 0.5 | 96 | 3.2 | Normal | Choline, C-11, PET, axumin | Abd | N |
| 5 | 38 | T2b | G9 | BS, MRI | 36.25 | Y | 0.35 | 24 | 3.94 | Normal | - | PSA only | N |
| 6 | 15.5 | T2b | G9 | BS, CT, MRI | 36.25 | Y | 0.1 | 48 | 3.0 | Abnormal | Axumin, MRI, PSMA | Bone, local | N |
| 7 | 20.4 | T1c | G7 | MRI | 36.25 | N | 6.8 | 9 | 11 | Normal | BS, CT | Bone | Curative |
| 8 | 47 | T2 | G9 | BS, CT | 36.25 | Y | <0.1 | 36 | 5.1 | Abnormal | PSMA | Local | N |
| 9 | 6.8 | T2c | G8 | - | 35 | Y | 0.1 | 24 | 4 | Abnormal | - | PSA only | N |
| 10 | 8.4 | T2a | G8 | - | 36.25 | Y | 0.5 | 21 | 4.8 | Normal | BS | Bone | Curative |
| 11 | 54 | T2b | G9 | MRI | 36.25 | N | 0.9 | 13 | 2.8 | Abnormal | BS, CT | Bone, pelvis | N |
| 12 | 12.6 | T1c | G8 | BS, CT, MRI | 36.25 | Y | 0.1 | 24 | 2.3 | Abnormal | BS, CT | PSA only | N |
| 13 | 1.3 | T2a | G8 | MRI | 36.25 | N | 1.23 | 48 | 2.6 | Abnormal | Axumin | Abd, bone, pelvis | Curative |
| 14 | 7.9 | T2b | G8 | - | 36.25 | Y | 0.6 | 18 | 3.1 | Abnormal | Biopsy, BS, MRI | Bone, pelvis | Palliative |
| 15 | 25.4 | T2a | G7 | CT | 36.25 | Y | 2.2 | 36 | 24 | Normal | BS, MRI | Bone, local | Curative |
| 16 | 10.3 | T2b | G9 | BS | 35 | Y | 0.1 | 36 | 2.2 | Abnormal | - | PSA only | N |
| 17 | 40 | T2c | G8 | BS | 36.25 | Y | <0.1 | 18 | 3.9 | Abnormal | BS | PSA only | N |
| 18 | 17 | T2b | G8 | - | 35 | N | 0.9 | 42 | 2.9 | Normal | BS | Bone | N |
| 19 | 8.3 | T2c | G7 | MRI | 36.25 | N | 0.22 | 131 | 4.3 | Abnormal | Axumin | PSA only | N |
| 20 | 60 | T2b | G7 | MRI | 36.25 | Y | 3.6 | 36 | 55.7 | Normal | MRI | Local | N |
| 21 | 31.6 | T1c | G7 | BS, MRI | 36.25 | Y | 0.1 | 90 | 429.8 | Normal | BS, CT | PSA only | N |
| 22 | 46.1 | T2b | G8 | BS, CT, MRI | 35 | Y | 34 | 3 | 61.9 | Abnormal | BS | Bone | Palliative |
| 23 | 5.5 | T1c | G9 | MRI | 36.25 | Y | 0.1 | 50 | 5.27 | Normal | MRI, CT, BS | Bone, local | N |
| 24 | 8.5 | T2c | G9 | BS | 36.25 | Y | 1.6 | 3 | 6.2 | Abnormal | BS, CT | Bone | N |
| 25 | 4.3 | T1c | G8 | CT, MRI | 36.25 | Y | <0.1 | 36 | 36.6 | Normal | BS, PSMA | Abd, pelvis | N |
| 26 | 4.7 | T2a | G9 | BS, CT | 36.25 | Y | <0.1 | 104 | 0.39 | Normal | PSMA | Abd | Curative |
| 27 | 37.5 | T2a | G8 | BS, MRI | 36.25 | N | 0.8 | 80 | 3.1 | Normal | MRI, PSMA | Local | N |
| 28 | 17.6 | T1c | G9 | MRI | 36.25 | N | 1 | 64 | 3.2 | Normal | MRI | Local | N |
| 29 | 20.3 | T2c | G9 | - | 35 | Y | 0.8 | 24 | 8.8 | Abnormal | BS | Bone | No |
| 30 | 4.8 | T1b | G9 | BS, MRI | 36.25 | Y | 0.4 | 26 | 2.9 | - | PSMA | Pelvis | Curative |
| 31 | 22.4 | T2c | G8 | BS, CT | 36.25 | Y | 0.1 | 6 | 6.3 | Abnormal | BS | Bone | N |
| 32 | 38 | T2b | G7 | BS | 36.25 | Y | 0.2 | 36 | 5.1 | - | - | PSA only | N |
| 33 | 7.9 | T1c | G8 | BS | 36.25 | Y | <0.1 | 56 | 5.2 | Normal | MRI | PSA only | N |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Diagnosis and Treatment · Advanced Radiotherapy Techniques · Prostate Cancer Treatment and Research
Introduction
Stereotactic body radiation therapy (SBRT) in low-risk (LR) and intermediate-risk (IR) prostate cancer (PCa) has demonstrated excellent tumor control with acceptable toxicity [1-3]. Two randomized trials comparing conventionally fractionated versus SBRT revealed comparable rates of physician-reported toxicities and patient-reported outcomes, emphasizing the consistent safety profile of SBRT [4,5]. Five-year biochemical failure-free rates were high in participants who received SBRT and were non-inferior to those of conventional radiotherapy [4,5]. These excellent results have established SBRT as the standard of care for LR and IR PCa patients [6].
The role of SBRT in high-risk (HR) PCa patients is an area of active clinical investigation. Conventionally fractionated radiation therapy (RT) for HR PCa has historically yielded poor cancer control [7]. Dose escalation via brachytherapy or SBRT boost has been utilized in the HR population, resulting in improved biochemical disease-free survival (BDFS), but with increased high-grade toxicity, inconvenience, and cost [8-11]. Androgen deprivation therapy (ADT) in combination with RT is recommended in HR patients to improve cancer control [6]. Results from the SHARP consortium showed improved BDFS in HR patients treated with SBRT receiving ADT with estimated four-year biochemical recurrence-free survival and distant metastasis-free survival rates of 82% and 89%, respectively [4]. The incidence of late grade 3 or higher genitourinary and gastrointestinal complications was low at 2.3% and 0.9%, respectively [4].
Robotic SBRT delivers hundreds of individualized non-isocentric beams with a targeting error of less than 1 mm, allowing the safe delivery of highly conformal treatment plans with steep dose gradients [12,13]. Unlike standard image-guided RT, robotic SBRT incorporates a real-time tracking system that provides updated prostate position information to the robot, allowing it to correct the targeting of the therapeutic beam during treatment [14]. This feature enables a reduction in the planning target volume (PTV), thereby better limiting the dose to surrounding critical organs. Recent analysis suggests that this approach may allow for intra-prostatic dose escalation with reduced urinary toxicity [15]. Here, we present our institutional experience with robotic SBRT for HR PCa.
Materials and methods
Patient selection
Patients eligible for inclusion in this retrospective study were those with HR PCa, as classified by D’Amico, who underwent robotic SBRT (CyberKnife, Accuray, Madison, WI) at Medstar Georgetown University Hospital from December 2008 to July 2023 [16]. Exclusion criteria included distant metastasis at baseline, prior pelvic radiotherapy, and/or prior radical prostatectomy. The Georgetown University Institutional Review Board approved this single institutional retrospective review (approval number: 2009-510).
Stereotactic body radiation therapy
Robotic SBRT was delivered as previously described [13,17]. Three to six gold fiducial markers were placed in the prostate. Seven days later, a treatment planning MRI was obtained, followed by a non-contrast simulation CT scan with 1.25 mm slice thickness. Both scans were done with an empty bladder, and patients were advised to have a low-gas, low-motility diet at least five days prior to imaging and treatment delivery. Patients did not take anything orally the night before the simulation, and an enema was administered one to two hours before imaging and treatment. Fused MR and CT scans were then used for treatment planning. The clinical target volume included the prostate, areas of radiographic extracapsular extension, and proximal seminal vesicles to the point where the left and right seminal vesicles separate. The rectum, bladder, and membranous urethra were contoured and evaluated. The SBRT-PTV equaled the clinical target volume, spaced 5 mm to the right and left and 3 mm elsewhere. Patients were treated with an SBRT prescription dose of 35-36.25 Gy to the PTV, which was delivered in five fractions of 7-7.25 Gy. Target position was verified multiple times during each treatment using paired, orthogonal X-ray images with a minimum of three properly placed fiducials. Shared decision-making was utilized to determine the use and duration of ADT [18].
Pretreatment assessment, follow-up, and statistical analysis
Prostate-specific antigen (PSA) levels were obtained, and PCa-specific QOL questionnaires were administered before the first SBRT treatment (baseline) and at three months, six months, 12 months, 18 months, 24 months, and then yearly after completion of RT. PSA nadirs were defined as the lowest PSA prior to failure. If a PSA rose, a digital rectal exam (DRE) was performed, and the best available imaging at the time was obtained as previously described [19]. Imaging studies, such as bone scans, abdominal and pelvic CT scans, and, more recently, PET imaging, were used to identify distant failures. Patterns of failure were classified as PSA only, local, pelvic node, abdominal node, or bone. Biochemical failure was classified as PSA-only if no malignancy was seen on the scan. Local failure was classified as occurring only in the prostate. Lymph node failure was classified as pelvic or abdominal. If bone metastases were identified, the failure was classified as bone independent of nodal status.
The health-related quality of life (HRQOL) domain scores for urinary incontinence, urinary irritative/obstructive, and bowel function were determined by the expanded PCa index composite (EPIC)-26 quality of life (QOL) questionnaire as previously described [20]. Briefly, EPIC scores ranged from 0 to 100, and higher scores indicated improved QOL. Differences in ongoing QOL scores were assessed and compared to the baseline and each follow-up using the Kruskal-Wallis test. This test was used to determine the significance of the difference between nonparametric, ordinal data. The Post-Hoc Dunn Multiple Comparison Test was employed to examine significant changes within HRQOL domains. Minimally important differences were calculated using 0.5 of a standard deviation at baseline.
Results
Patients
Between December 2008 and July 2023, 216 HR PCa patients were treated with robotic SBRT. The median follow-up was 40 months. Table 1 provides a summary of patient characteristics. The median age was 75 years (range: 54-94). Caucasian patients comprised 50% of the subjects, while Black patients accounted for 39% of the subjects. The median pretreatment PSA was 14.2 ng/ml (range: 1.3-148 ng/ml). The median prostate volume was 39 cc (range: 15-186 cc). The median baseline Charleston Comorbidity Index (CCI) score was 1, with 9.7% of patients having a CCI score above 3. ADT was administered to 75% of patients for a median duration of 10 months (range: 3-48 months).
Cancer control
In our analysis, a total of 33 recurrences (15% of total subjects) were observed, with 23 (11% of total subjects) occurring within 36 months, indicating a BDFS rate of 89% at three years. Figure 1 shows the BDFS curve, and Table 2 provides the patient characteristics of those who failed treatment. Notably, four recurrences (12% of all recurrences, 2% of total subjects) occurred within the first 12 months (Table 3). The median time to failure was 36 months, with a range of 3 to 121 months. The average initial PSA was 22.9 ng/ml, with an average PSA nadir of 1.82 ng/ml post-treatment and an average PSA at recurrence of 22.03 ng/ml.
Biochemical control for HR PCa receiving SBRT at three-year follow-upSBRT: stereotactic body radiation therapy, HR PCa: high-risk prostate cancer
Recurrence characteristics
Among all recurrences, bone metastases were the most common (34.15%), followed by PSA-only recurrences (24.39%), local recurrences (17.08%), and abdominal and pelvic lymph node involvement (12.2% each) (Table 2, Figure 2). There were no isolated seminal vesicle recurrences. High-grade disease was common, with Gleason scores of 8 and 9 accounting for 36% of recurrences each, Gleason 7 in 24%, and Gleason 6 in only 3%. ADT was used in 70% of recurrent cases, while 30% did not receive ADT. On clinical examination during recurrence follow-up, 47% had normal DRE findings and 53% had abnormal DREs.
Failure patterns after SBRT in HR PCaTypes of failure in HR PCa after five-fraction SBRT, alongside ADT use (yes/no) for each failure typeSBRT: stereotactic body radiation therapy, HR PCa: high-risk prostate cancer, ADT: androgen deprivation therapy, PSA: prostate-specific antigen
Quality of life
Figure 3 shows QOL following robotic SBRT. The study found that the mean urinary incontinence function score decreased slightly from 86.04 at baseline to 84.4 at the 36-month follow-up (p>0.05). Weak stream (14%) and frequency (24%) were the most common symptoms in the urinary irritative/obstructive domain. Similarly, the mean bowel function score showed a minor reduction from 92.7 at baseline to 90.6 at 36 months, without statistical significance (p>0.05). Bowel symptoms were less frequent than urinary symptoms, with urgency ranging from 5% to 7% over the study period, peaking at 7% at six months. The percentage of patients reporting bowel frequency increased from 3% at baseline to a peak of 8% at 18 months.
Average EPIC domain scores at baseline and follow up for HR PCa patients after receiving SBRT(A) EPIC GU incontinence domain. (B) EPIC GU irritative/obstructive domain. (C) EPIC bowel domain. The upper and lower thresholds represent clinically significant changes in score ( ½ SD). EPIC scores range from 0 to 100, with higher values indicating a more favorable QOL.EPIC: expanded prostate cancer index composite, SBRT: stereotactic body radiation therapy, GU: genitourinary, QOL: quality of life, SD: standard deviation, HR PCa: high-risk prostate cancer
Discussion
This study aimed to assess failure patterns and QOL metrics in a cohort of HRPC patients who received robotic SBRT without elective pelvic irradiation. Our results add to the growing body of evidence that definitive prostate SBRT for localized HRPC may have similar outcomes for patients while sparing them elective pelvic radiation dose. Our study saw favorable local disease control, with a three-year BDFS of 89%. These numbers are consistent with those of the SHARP consortium, which assessed a group of HRPC patients who also underwent definitive prostate SBRT [21]. We found that local failures constituted 21% of the total three-year recurrences, suggesting that BDFS could be higher with higher prescription doses. A growing body of evidence indicates that dose escalation to the DIL, or the prostate as a whole, significantly improves local control, and our findings support these data [22-24]. Staging PSMA-PET scans, with their emerging prominence in diagnosing and localizing HR primary PCa and recurrent disease, could help us safely escalate doses for our patients.
Pelvic lymph node recurrence constituted only 15% of our failures. This suggests elective nodal irradiation (ENI) would not have improved the clinical outcomes of most of our cohort by the three-year follow-up. Indeed, the literature regarding elective pelvic ENI remains controversial, showing mixed benefits [25]. Additionally, those who undergo whole-pelvis radiotherapy (WPRT) usually experience much higher rates of gastrointestinal toxicity in the long term. The POP-RT trial shows improved short-term BDFS with WPRT; however, most of these patients underwent pre-treatment PSMA imaging to rule out metastases or locoregional spread [26]. Our patients did not undergo PSMA imaging during initial staging, so it is difficult to apply the POP-RT results to our cohort. It is possible that had our patients undergone PSMA imaging prior to treatment, pelvic nodal metastases could have been identified, in which case these would not be considered failures from the omission of pelvic ENI. Furthermore, abdominal lymph node recurrence constituted 12.2% of our total failures, a proportion that is favorably small. These failures would likely not have been impacted by WPRT.
Our cohort had a relatively large proportion of patients from lower socioeconomic backgrounds, who faced numerous social challenges. Many of our patients had difficulty with transportation and social support. A large proportion were frail. These patients likely would have had difficulty with a several-week regimen of daily RT. Our results can therefore be applied to these populations, demonstrating that five-fraction SBRT remains a highly favorable option, even for HR PCa. Recent data suggest that ultrahypofractionated elective pelvic nodal irradiation (25 Gy in five fractions) is safe and effective at preventing pelvic nodal recurrences [27]. The inability to treat the prostate and pelvic nodes simultaneously is a known limitation of robotic SBRT [28].
Despite highlighting the favorable outcomes associated with hypofractionated SBRT in HR PCa patients, we acknowledge the limitations inherent in our retrospective study design and reliance on patient-reported outcomes. Notably, the absence of stratification and propensity-matched scoring warrants further exploration in future research to validate these findings. There was variability in initial imaging during the staging and workup of each patient, affecting cohort uniformity.
Conclusions
Definitive prostate SBRT for localized HRPC has been shown to yield similar short-term oncologic outcomes to the current standard of care while still affording patients an excellent QOL. We see non-significant decreases in the gastrointestinal and genitourinary EPIC domain scores, suggesting that this treatment yields minimal long-term toxicity at three-year follow-up. We also note that only 12.2% of treatment failures occurred in the pelvis, prompting us to question the cost-benefit utility of electively irradiating the pelvis in the first place. Prostate SBRT spares this dose to the pelvis while still allowing the possibility for future salvage RT if locoregional failure occurs. While the idea of elective pelvic nodal irradiation remains controversial in the HR patient population, our data support local definitive treatment as a favorable option. This option should be especially considered for patients who are at a higher risk of missing treatments or who prefer a shorter course.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tumor control probability modeling and systematic review of the literature of stereotactic body radiation therapy for prostate cancer Int J Radiat Oncol Biol Phys Royce TJ Mavroidis P Wang K 22723611020213290056110.1016/j.ijrobp.2020.08.014PMC 9445430 · doi ↗ · pubmed ↗
- 2Multicenter trial of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer: survival and toxicity endpoints Int J Radiat Oncol Biol Phys Meier RM Bloch DA Cotrutz C 29630310220183019186410.1016/j.ijrobp.2018.05.040 · doi ↗ · pubmed ↗
- 3Long-term outcomes of stereotactic body radiotherapy for low-risk and intermediate-risk prostate cancer JAMA Netw Open Kishan AU Dang A Katz AJ 1880062201910.1001/jamanetworkopen.2018.8006 PMC 648459630735235 · doi ↗ · pubmed ↗
- 4Phase 3 trial of stereotactic body radiotherapy in localized prostate cancer N Engl J Med van As N Griffin C Tree A 1413142539120243941337710.1056/nejmoa 2403365 PMC 7616714 · doi ↗ · pubmed ↗
- 5Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial Lancet Widmark A Gunnlaugsson A Beckman L 38539510196201910.1016/S 0140-6736(19)31131-631227373 · doi ↗ · pubmed ↗
- 6Acute lymphoblastic leukemia 3 2025 2025 https://www.nccn.org/guidelines/guidelines-detail
- 7Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer Int J Radiat Oncol Biol Phys Zelefsky MJ Levin EJ Hunt M Yamada Y Shippy AM Jackson A Amols HI 112411297020081831352610.1016/j.ijrobp.2007.11.044 · doi ↗ · pubmed ↗
- 8Brachytherapy boost improves survival and decreases risk of developing distant metastases compared to external beam radiotherapy alone in intermediate and high risk group prostate cancer patients Radiother Oncol Miszczyk M MagrowskiŁ Krzysztofiak T 10963218320233696344210.1016/j.radonc.2023.109632 · doi ↗ · pubmed ↗