The Effects of a Reproductive Health Voucher Program on Out-of-Pocket Family Planning and Safe Motherhood Service Expenses: A Yemeni Study
Omar Z. Al-Sakkaf, El-Morsy A. El-Morsy, Shaimaa A. Senosy, Al Shaimaa Ibrahim Rabie, Ahmed E. Altyar, Rania M. Sarhan, Marian S. Boshra, Doaa M. Khalil

TL;DR
A voucher program in Yemen reduced out-of-pocket costs for reproductive health services, improving access and satisfaction for mothers compared to areas without the program.
Contribution
Demonstrates the effectiveness of a reproductive health voucher program in improving service use and satisfaction in low-income settings.
Findings
Mothers in the voucher program used reproductive health services more frequently than those without vouchers.
Voucher users reported higher satisfaction with all aspects of reproductive healthcare.
The program significantly increased the use of modern contraceptive methods and facility-based deliveries.
Abstract
Background/Objectives: Using healthcare vouchers mitigates the financial burdens of low-income individuals, therefore enhancing mothers’ satisfaction and encouraging service utilization. In Yemen, reducing financial barriers results in marked improvement in reproductive health services utilization for mothers and their newborns. Such financial strain can be addressed through reproductive health vouchers, which reduce out-of-pocket expenses of family planning, pregnancy, birth, postnatal care and neonatal care. This study compares the Safe Motherhood and Family Planning Voucher Program in the Lahj governorate to the non-voucher program in the Abyan governorate in terms of enhancement of reproductive healthcare accessibility and use. Methods: This facility-based, quantitative, comparative, cross-sectional study was conducted in the Lahj governorate, which supports the Safe Motherhood and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
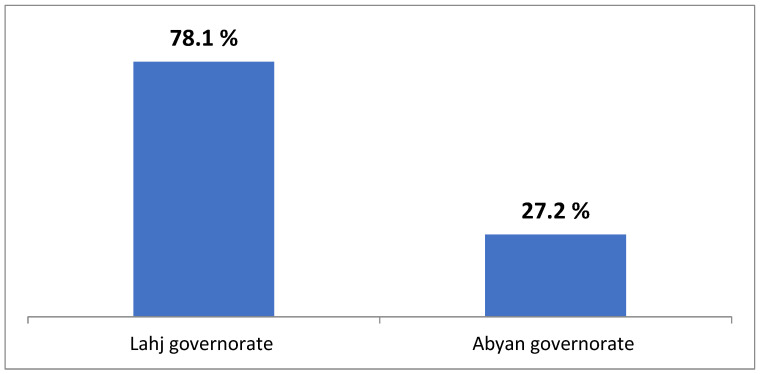 Figure 1
Figure 1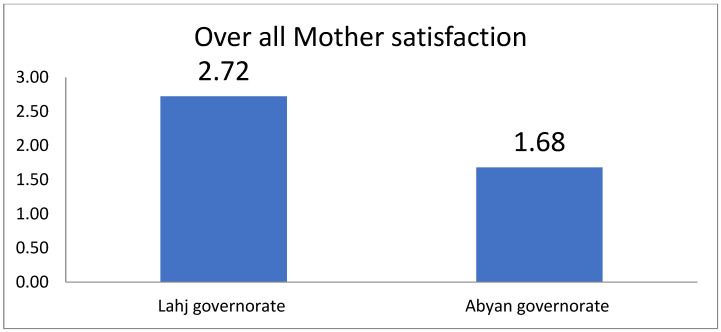 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Healthcare Systems and Reforms · Poverty, Education, and Child Welfare
1. Introduction
Unfortunately, fragile and conflict-affected nations fell behind in terms of attaining the Millennium Development Goals (MDGs). The Sustainable Development Goals (SDGs) do not consider the distinctive hurdles these nations face, especially when it comes to providing their citizens with essential services [1,2]. Weak and failing institutions, extreme poverty and inequality, and the global expansion of violence and conflict are among the numerous factors that contribute to national vulnerability. Along with the dynamic nature of healthcare needs, the unpredictability of healthcare expenses, and regional variations in morbidity and mortality rates, humanitarian crises pose unique challenges that call for creative responses [3].
The supply of healthcare and the facilitation of access to services present substantial obstacles for governments in these conditions, since pregnant mothers and their newborns face unique health risks in states ravaged by violence [4]. Yemeni women experience various forms of violence, particularly during the displacement crisis, in which over 3 million Yemeni citizens have become internally displaced persons (IDPs). This situation has significantly impacted maternal and infant health, leading to increased morbidity and mortality rates among mothers and their infants. Atrocities, forced migration, and other natural disasters account for almost 60% of maternal deaths, 53% of child deaths, and 45% of infant deaths worldwide [5].
Women and their families can receive healthcare more easily with the support of vouchers for safe motherhood programs, which also channel critical funds to service providers, allowing them to improve the quality of their services. Healthcare vouchers have a long history of providing underserved populations with access to valuable services [6,7].
Yemen has been on the list of fragile nations and conflict-affected regions since 2010, and it is one of the poorest countries in the Middle East and North Africa (MENA) region [4]. Notably, public health facilities in rural areas of Yemen are underfunded, whereas most private healthcare facilities are located in urban areas, particularly within the main cities of governorates and their districts, resulting in relatively better accessibility to health services in urban areas. These facilities often cater to individuals with higher disposable incomes.
There are myriad financial hurdles that affect underprivileged mothers, such as the cost of maternal health treatments, as well as travel and subsistence expenses while they are away from home, all of which incur significant costs. The life and health of pregnant women and their fetuses are put at great risk when they travel to a distant health facility, considering factors such as high and unpredictable expenses, lengthy distances, and unsafe traveling conditions [4]. A significant number of women do not have access to family planning, resulting in a heightened risk of unplanned pregnancies in environments that may endanger their health and well-being. Consequently, an estimated 75,000 pregnant Yemeni women are in danger of experiencing difficulties due to the critical condition of health services in the nation [8].
The Reproductive Health Voucher Program in Yemen, funded by the German government through the Kreditanstalt für Wiederaufbau (KfW), has been running since 2013 and serves two governorates: Ibb in the central region and Lahj in the southern region. As a result of the conflict, the program remained suspended from 2015 until the end of 2018. At the present time, serious food insecurity is afflicting Lahj, one of the poorest governorates in southern Yemen [4]. Nevertheless, the governorate has benefited from a relatively functional public health system and committed health staff engaged in discovering novel ways to improve the health of Lahj residents [9]. This study targeted two governorates: the Lahj governorate, which is supported by the SMHFPVP, and the Abyan governorate, which is not.
The Lahj governorate is characterized by the following features:
Geography and Climate:
Lahj is situated in southwestern Yemen, bordered by the Red Sea to the west and the Arabian Sea to the south. The governorate encompasses diverse landscapes, including coastal plains, fertile valleys, and mountainous regions. The climate varies from arid in the lowlands to temperate in the highlands.
Demographics and Society:
The population of Lahj is predominantly Arab, with a rich cultural heritage influenced by various historical periods. The society is organized into tribal communities, each with its own customs and traditions. The urban centers are characterized by a mix of modern and traditional architecture, while rural areas maintain a more traditional lifestyle.
Economy and Livelihood:
Agriculture is the backbone of Lahj’s economy, with the fertile Wadi Tuban valley supporting the cultivation of crops such as sorghum, sesame, and vegetables. Livestock farming is also prevalent, with sheep and goats being the most common. Fishing along the coastline provides an additional source of income for coastal communities.
History and Politics:
Historically, Lahj was part of the Sultanate of Lahj, a protectorate under British colonial rule until 1967. The region has experienced various political changes, and its strategic location has made it a focal point in Yemen’s modern history.
The Abyan governorate is characterized by the following features:
Geography and Climate:
Abyan is located in southern Yemen, bordering the Arabian Sea. The governorate features a mix of coastal plains, fertile valleys, and mountainous terrain. The climate is generally hot and arid, with seasonal variations influencing agricultural practices.
Demographics and Society:
The Abyan population is primarily Arab, with a strong presence of tribal communities. The social structure is deeply rooted in tribal affiliations, which play a significant role in governance and community life. The region has a history of political instability, affecting its social dynamics.
Economy and Livelihood:
Agriculture is a key economic activity in Abyan, with the fertile valleys supporting the cultivation of crops like bananas, dates, and vegetables. Livestock farming and fishing are also important, contributing to the livelihood of many residents. However, the economy has faced challenges due to conflicts and environmental factors.
History and Politics:
Abyan has a complex history, with periods of conflict and political upheaval. It was once part of the Fadhli Sultanate. The governorate has experienced significant political changes, influencing its development and stability.
Table 1 shows the sociodemographic and health characteristics of mothers of reproductive age (15–49) in the Lahj and Abyan governorates.
N.B.: Despite the sociodemographic similarities between Abyan and Lahj, as demonstrated in Table 1, any bias introduced by differences in socioeconomic characteristics between the two governorates would tend to favor Abyan, since Abyan residents fall within a higher wealth quintile compared to Lahj residents, and the literacy rate is much higher in Abyan (which has a slightly higher economic status and literacy percentage).
Local voucher distributors find eligible women in the community, educate them about safe motherhood services, and offer vouchers for Yemeni Rial (YER) 200 (less than USD 1) [10]. About 15% of vouchers are totally subsidized for individuals who cannot pay this low charge. The voucher provides free access to four antenatal care (ANC) appointments; safe delivery, including in the case of pregnancy-related complications and cesarean section; two postnatal care (PNC) visits; two neonatal care (NNC) visits and postnatal family planning. The package includes free transportation to a hospital, as well as lodging for companions and food, if necessary.
In the current study, we assessed the effectiveness of the Safe Motherhood and Family Planning Voucher Program in improving the access and utilization of reproductive health services in the Lahj governorate through examining the uptake of specific RH services among women in the health facilities studied, compared to in the Abyan governorate, where the program is not supported.
2. Materials and Methods
2.1. Study Type, Location, and Period
This quantitative, facility-based, analytical, cross-sectional study was designed to investigate the effectiveness of the SMHFPVP in improving access to and utilization of reproductive health services (RHSs) in the Lahj governorate, where the program was active and supporting health facilities, compared to in the Abyan governorate, which was not supported by the SMHFPVP. The Lahj governorate was chosen since it was the only governorate in the southeastern region that conducted the program, while the Abyan governorate, another southeastern governorate, was not supported by the SMHFPVP and is similar to the Lahj governorate in terms of sociodemographic characteristics, the types and distribution of health facilities, and geographical characteristics. A program effectiveness comparison was easy because the Lahj governorate was SMHFPVP-supported while the Abyan governorate was not. The study selected districts and health facilities (HFs) in the Lahj governorate that provided reproductive health services (RHSs) with support from the SMHFPVP; in contrast, in the Abyan governorate, HFs were included that offered RHSs without support from the SMHFPVP. The study targeted mothers in both governorates who attended the targeted health facilities from January to December 2019; this was the period during which the SMHFPVP was fully implemented in the selected HFs in the Lahj governorate. The period of data collection was from July to December 2020.
2.2. Population Frame and Sample Size
The population frame was prepared by the researcher and the head of the Statistical Unit at both Governorate Health Offices (GHOs), with the help of an expert from the Central Statistical Organization (CSO) in the Lahj and Abyan governorates and the SMHFPVP coordinator in Lahj. In the Abyan governorate, the study targeted only HFs providing RHSs within districts with the same characteristics and the same number as the districts in the Lahj governorate, which did not receive any support from donors during 2019. This was conducted with full coordination with the Abyan GHO and Reproductive Health (RH) Department. In both governorates, the study included all governorate hospitals (GHs), district hospitals (DHs), maternal care health centers (MCHCs), health centers (HCs), and private hospitals (PHs) from the selected districts that fulfilled the inclusion criteria. Regarding health units (HUs), only 50% from each district fulfilled the inclusion criteria, from which sample units were selected using a simple random or systematic sampling technique.
Healthcare Facility (HF) Criteria:Lahj Governorate:Included: Public/private HFs providing RHSs (2018–2019), fully supported by the SMHFPVP in 2019, and not supported by other donors.Excluded: HFs not providing RHSs, not supported by the SMHFPVP in 2019, or supported by other donors.Abyan Governorate:Included: Public/private HFs providing RHSs (2018–2019) and not supported by any donors.Excluded: HFs not providing RHSs or supported by any donors.Mother Selection Criteria (Reproductive Age 15–49)Both Governorates: Mothers attending eligible HFs in 2019 until the sample size was reached.Lahj Governorate:Mothers who:
- -Had a child ≥2 years old prior to the study.
- -Received RHSs from SMHFPVP-supported HFs only.
- -Attended SMHFPVP-supported HFs for RHSs in 2019.
- -Lived in the same household (≥1 year) within the catchment area. Abyan Governorate:Mothers who:
- -Had a child ≥2 years old prior to the study.
- -Received RHSs from HFs with no donor support.
- -Lived in the same household (≥1 year) within the catchment area.
The sample preparation frame was based on RH reports from both governorates in 2019, illustrating the number and percentage of utilization of RHS packages among women who sought specific RH services in the targeted health facilities in both governorates, including ANC, facility-based delivery (FBD) (normal or cesarean section delivery), PNC, family planning (FP) services, and, finally, treatment of pregnancy-related complications (PRCs), for each targeted HF. This frame was used to calculate the prevalence of different RHSs per HF and district. By using the formula below, the required number of mothers was calculated for each HF and district. Subsequently, the required number of mothers comprising the required sample size in the selected HFs and districts was determined proportionately to the prevalence of RHSs and mothers who attended the HFs. The sample units (HFs) were selected using a simple random sampling technique.
All HFs in the targeted districts from both governorates that provided RHSs were listed. The number and the percentage of mothers who attended each of the targeted HFs from the analyzed districts during 2019 were determined in order to obtain the prevalence of utilization of each type of RHS in each HF during 2019. Probability proportionate to sample size was used to select the required number of mothers who fulfilled the inclusion criteria to yield and determine the needed number of mothers per HF in each district. In all the selected HFs, eligible mothers were recruited to participate in a face-to-face interview.
The sample size of married women (mothers), aged 15–49 years, who attended HFs in the targeted districts and fulfilled the inclusion and exclusion criteria was calculated using the following formula:
where n = the sample size of married women (mothers) aged 15–49 years old selected for the study; k = the standard of 1.96 at 95% certainty; p = the prevalence of ANC, delivery by skilled birth personnel (SBPs) (FBD and home delivery (HD), PNC, treatment of pregnancy-related complications (PRCs), and FP in the targeted districts; q = 1 – p; and d = the precision or error allowable, which, in our study, is 0.05.
The calculated sample size in the Lahj governorate (based on prevalence assumptions), from the targeted districts, was 369 mothers, and 10% was added to this sample size to compensate for possible non-response, reaching a total sample size of 406 mothers. From the Abyan governorate targeted districts, 374 mothers, as well as 10% additional participants, were recruited to compensate for possible non-response, with a total sample size of 411 mothers. The required number of mothers from each district was considered using the probability proportionate to the number of mothers who received ANC in each target; they were interviewed directly, face-to-face, at the HFs in those districts.
2.3. Study Instruments/Data Collection Techniques (Questionnaire)
Paper-based, structured, pre-designed, and pre-tested questionnaires were employed in face-to-face interviews with the targeted mothers. Before the study, these questionnaires were piloted for consistency and validity. The questionnaires were designed utilizing numerous sources of standard RH information and based on national child and family health surveys, while satisfaction measures were taken from past studies. The questionnaires for the mothers who attended HFs consisted of the following sections: [the distribution of the selected health facilities; the distribution of the opinions of the mothers interviewed toward HF characteristics and the socioeconomic and sociodemographic characteristics of the mothers; reproductive health and family planning service utilization by the mothers interviewed; mothers’ satisfaction items; an SMHFPVP-related section (only for targeted mothers from the Lahj governorate); and utilization of reproductive health and family planning services (RHFPSs) by mothers (ANC, delivery, PNC, and FP)].
To understand mothers’ RH behaviors and decision-making concerning the aforementioned topics, well-structured interviews were conducted in both governorates. We employed standardized satisfaction-evaluation measures to assess mothers’ satisfaction, including Bruce’s RHS quality points, in the questionnaire [11].
These were as follows: (1) the accessibility and environmental characteristics of the HFs; (2) the continuity and sustainability of healthcare in the HFs; (3) the communication skills of staff and interpersonal relationships; (4) the provision of health education in the HFs; (5) the quality of healthcare services provided by the HFs. A total of 29 questions were prepared for all five aspects, and these were tested for their validity and reliability. The perceptions of the respondents were measured and rated on a three-point Likert Scale consisting of (1) “Low Satisfaction”, (2) “Moderate Satisfaction”, and (3) “High Satisfaction”. Overall satisfaction was defined as the average score for the five measured aspects of satisfaction. The mean level of satisfaction was calculated by averaging the respondents’ ratings for the satisfaction parameters. If a mother’s response scored (2.34) or above, the client was considered to have a high level of satisfaction, whereas if she scored (1.66) or less, she was considered to have a low level of satisfaction, and if she scored (1.67–2.33), the client was considered to have an undecided level of satisfaction (Moderate). The questionnaires were reviewed by RH experts at the Faculty of Medicine and RH experts at the Ministry of Health in both governorates in order to evaluate the relevance (or face validity) and completeness (or content validity) of the questionnaire. Participants providing and receiving RH and FP services were asked to describe their perceptions and reasons for satisfaction with the quality of the services. After piloting for consistency and validity, the questionnaires were used in the study. To ensure that the mothers could understand the questions, pilot research was conducted with 20 responses from each group. These responses were excluded from the study, and certain questions were rephrased. To assess questionnaire reliability, Cronbach’s α was determined.
2.4. Data Processing and Analysis
After the researcher checked and coded the questionnaires, Statistical Package for Social Sciences (SPSS) version 21 was utilized to examine quantitative data. Normality was evaluated using histograms and Kolmogorov–Smirnov tests (p > 0.05). In bivariate analysis, a t-test was employed for normally distributed data and a Whitney U-test for non-normal data. Comparisons were made using chi-square analysis for categorical variables. Fisher’s exact test and Yates’s adjustment for small cell frequency were significant tests. Quantitative variables were expressed using arithmetic means ± standard deviations (SDs) for normally distributed data and median & interquartile range (IQR) for not normally distributed variables. All the statistical analyses considered p-values < 0.05 to be significant.
3. Results
3.1. The Distribution of the Selected Health Facilities and the Mothers Interviewed
Around half the selected health facilities were health units in both governorates, followed by health centers, which represented around one-third (29.5%) in the Lahj governorate and 17.3% in the Abyan governorate, while the remaining health facilities were nearly equally distributed. Around half (44.8%) of the mothers interviewed attended health centers in the Lahj governorate, compared with 19.5% in the Abyan governorate, and around one-third (30.4%) of the mothers attended district hospitals in the Abyan governorate, compared with 14.8% in the Lahj governorate. On the other hand, mothers’ attendance at the other types of health facilities was nearly equal in both governorates.
3.2. The Sociodemographic Characteristics of the Mothers Interviewed
Table 2 illustrates the sociodemographic characteristics of the mothers interviewed in the Lahj and Abyan governorates.
Regarding the sociodemographic characteristics of the mothers interviewed in both governorates, we found no statistically significant differences, including in the mother’s age and education level, husband’s education level, and monthly family income; this indicates that these variables had no effect on access to and utilization of reproductive health services (RHSs) in either governorate.
3.3. The Opinions of the Mothers Interviewed Regarding the Characteristics of the Health Facilities
Table 3 demonstrates the distribution of the opinions of the mothers interviewed who attended HFs seeking RHSs. While the reported accessibility and the time to reach health facilities did not differ significantly between the Lahj and Abyan governorates (p = 0.189 and p = 0.471, respectively), transportation methods varied notably. Renting a car—funded by the SMHFPVP—was more common in Lahj (75.6%) than Abyan (58.9%), whereas walking was more frequent in Abyan (32.8%) than Lahj (19.0%) (both p < 0.001). Lahj also had significantly higher rates of routine 8 h workdays (66.5% vs. 52.3%) and more suitable working conditions (95.6% vs. 85.6%) (both p < 0.001). No significant differences were found in staff availability or waiting time suitability.
3.4. Family Planning (FP) Services
Table 4 illustrates the characteristics of the family planning (FP) methods utilized by the mothers interviewed in the Lahj and Abyan governorates. Mothers’ knowledge of FP methods and their acceptance of FP utilization were high in both governorates; however, they were significantly higher in the Lahj governorate compared to in the Abyan governorate. There was a non-statistically significant difference regarding previous FP utilization and the type of FP used. Modern FP methods (oral contraceptive pills, implants, injectables, contraceptive patches, vaginal rings, and intrauterine devices (IUDs)), and public health facilities as sources of FP utilization were both significantly higher in the Lahj governorate compared to in the Abyan governorate.
3.5. The Gestational History of the Mothers Interviewed in Both Governorates
Regarding the gestational history of the mothers interviewed in the voucher and non-voucher governorates, all the studied variables showed no statistically significant differences between both groups, as shown in Table 5 below.
3.6. Antenatal Care Service (ANC) Utilization in Both Governorates
Table 6 describes mothers’ utilization of ANC services as part of RHSs. In the table, all the variables showed that there were highly significant differences between the Lahj governorate and the Abyan governorate regarding the utilization of ANC services.
3.7. The Last-Delivery Characteristics of the Mothers Interviewed in Both Governorates
Table 7 demonstrates the last-delivery characteristics among the mothers interviewed in both governorates. Cesarean section (CS) delivery was significantly more frequently undertaken in the Lahj governorate compared to in the Abyan governorate (22.2% vs. 11.9%, p < 0.001); health facility delivery (public/private) was significantly higher in the Lahj governorate compared to in the Abyan governorate (88.2% vs. 62.5%, p < 0.001); delivery with trained healthcare providers (physician/ midwife/nurses) was significantly more frequent in the Lahj governorate compared to in the Abyan governorate (99.0% vs. 80.3%, p < 0.001); and free-of-charge delivery services were significantly more frequent in the Lahj governorate compared to in the Abyan governorate (95.8% vs. 32.8%, p < 0.001).
3.8. Postnatal Care (PNC) Service Utilization in Both Governorates
The utilization of PNC services was significantly higher in the Lahj governorate compared to in the Abyan governorate (73.9% vs. 25.1%, p < 0.001),
Table 8 demonstrates the postnatal care (PNC) utilization among the mothers interviewed in both governorates. Health facility PNC (public /private) was significantly more commonly used in the Lahj governorate compared to in the Abyan governorate (72.3% vs. 51.5%, p < 0.001); PNC with physicians was significantly more common in the Lahj governorate compared to in the Abyan governorate (58.7% vs. 22.3%, p < 0.001); the number of PNC visits was significantly higher in the Lahj governorate compared to in the Abyan governorate; and free-of-charge PNC services were significantly more prevalent in the Lahj governorate compared to in the Abyan governorate (98.3% vs. 38.8%, p < 0.001).
3.9. Neonatal Care (NNC) Service Utilization in Both Governorates
Table 9 demonstrates the neonatal care (NNC) utilization among the mothers interviewed in both governorates. NNC utilization was significantly higher in the Lahj governorate compared to in the Abyan governorate (63.5% vs. 24.6%, p < 0.001); health facility NNC (public /private) was significantly more common in the Lahj governorate compared to in the Abyan governorate (76.0% vs. 45.5%, p < 0.001); NNC with physicians was substantially more utilized in the Lahj governorate compared to in the Abyan governorate (50.4% vs. 28.7%, p < 0.001); the number of NNC visits was significantly higher in the Lahj governorate compared to in the Abyan governorate; and free-of-charge NNC services were significantly more prevalent in the Lahj governorate compared to in the Abyan governorate (97.7% vs. 40.6%, p < 0.001).
3.10. Mothers’ Satisfaction with Various Characteristics of Healthcare Facilities
Table 10 and Table 11 illustrate the mothers’ satisfaction with the characteristics of the health facility where the RHSs were accessed. As shown in the two tables, in all the items in the sections, the differences in means and percentages between both governorates are statistically significant (p < 0.001).
Almost all interviewed mothers in Lahj reported receiving and using ANC services provided by the SMHFPVP (98.5%); however, this utilization rate dwindled to 73.8% for PNC services and 63.5% for NNC services. Regarding family planning services, 76.6% of the mothers received an FP voucher and used it, while 9.6% received one through the SMHFPVP but did not use it, and the remaining 13.8% did not receive one and did not care about FP vouchers in general (Table 12).
Figure 1 and Figure 2 illustrate the overall satisfaction of mothers with the health facility where they received their RHSs. As shown in the two figures, the difference in the overall mean satisfaction score between both governorates was statistically significant, with p-values < 0.001.
4. Discussion
Access to and the cost of private primary care services are especially concerning in Yemen due to the undersupply of public primary care services and the financial obstacles caused by out-of-pocket payments [12]. There are three main benefits to the maternal health voucher program: products or services related to maternal and neonatal health, transportation, and accommodation.
In our study, the Lahj governorate demonstrated significantly superior RHS utilization and satisfaction compared to Abyan, despite Abyan having slightly better socioeconomic qualities, such as a higher wealth quintile and a higher rate of literacy. When analyzing the demographic data of our participants, we found that both governorates were statistically comparable, with no significant differences between the mothers interviewed in both regions regarding age (p = 0.508), education (p = 0.813), the husband’s education (p = 0.079), or monthly family income (p = 0.094), indicating that the disparities stemmed from health system factors, namely the SMHFPVP, rather than population characteristics. Additionally, mothers in Lahj had substantially higher rates of antenatal care (98.5% vs. 77.6%), facility-based deliveries (88.2% vs. 62.5%), postnatal care (73.9% vs. 25.1%), and neonatal care (63.5% vs. 24.6%), with most services being free-of-charge in Lahj, with the help of the SMHFPVP (72.3% free ANC, 95.8% free deliveries, 98.3% free PNC, and 97.7% NNC services, vs. 34.5%, 32.8%, 38.8%, and 40.6% in Abyan, respectively; p < 0.001).
Of the studied variables, statistically meaningful differences were noted in terms of methods of transportation, working hours, and workplace conditions. Our analysis revealed that 75.6% of mothers in Lahj utilized rental cars to commute to the healthcare facility (paid for by the SMHFPVP), as opposed to 58.9% of mothers in Abyan (who had no financial support by any program). Moreover, a significantly larger number of mothers in Abyan resorted to walking to the healthcare facility compared to in Lahj (32.8% vs. 19%; p < 0.001). Evidently, having a reliable means of transportation is critical for individuals to be able to access health centers and effectively use reproductive health services. Considering this, the availability of transportation becomes pivotal. The significantly higher rate of rental car use among Lahj mothers could be explained by the fact that the SMHFPVP in the Lahj governorate finances the transportation costs of its targeted mothers so that they may commute to and from medical appointments. Mothers in the Lahj governorate were probably able to overcome mobility obstacles and access reproductive health services more readily than mothers in the Abyan governorate thanks to this financial assistance, which made rental cars more accessible and inexpensive. However, women in the Lahj governorate (supported by the SMHFPVP) and the Abyan governorate (unsupported) did not differ significantly in their overall reports of accessibility of health facilities, with 72.2% of women in Lahj reporting easy accessibility compared to 70.3% in Abyan (p= 0.189).
Studies that have found women to be financially burdened by travel expenses indicate that transportation is a crucial component of maternal health voucher programs [13]. In 2018, 8.8 million Yemenis (30.6%) lived more than 30 min from the nearest partially or fully functional public primary healthcare facility, and 12.1 million (42.4%) lived more than 1 h away [14], which makes the results of our current study consistent with many previous studies in the same context. According to Tappis et al., financial access often hinders care-seeking more than physical access [15]. As expected, our study found that transportation is a major factor in the decision to use a health facility for ANC and delivery services. Mothers who used rental cars had an increased probability of using health facility delivery services as seen in Lahj governorate because the program covered the cost of rental cars compared with mother in Abyan where the program was not implemented.
In several Yemeni provinces and districts, the distance between health facilities and population housing, poor road infrastructure, and lack of transportation prevent people from using needed RH services [14]. A recent qualitative study examined a situation analysis for the provision of integrated comprehensive sexual and reproductive health services to Yemeni displaced people, stating that “Geographic distance and challenging roads with the scarcity of transportation and its high cost ranging from 20,000 to 30,000 YRs in this financial difficulty has prohibited women from accessing health care services.” [16].
A comprehensive assessment of eight conflict-affected countries, including Yemen, examined maternal health service consumption from both perspectives: the demand (community) angle included mobility, female education, autonomy, health awareness, and ability to pay, whereas the supply (health services) angle included service availability and quality, community health workers, and health facility charges and informal payment [17].
The survey found considerable differences in the availability of health facilities between the governorates. A higher number of health facilities in the Abyan governorate are available 24/7 than in Lahj (47.7% vs. 33.5%, p < 0.001). Despite this, targeted women in the Abyan governorate, which lacked program assistance, used RHSs less than in the Lahj governorate, which was supported by the SMHFPVP. This shows that variables other than health facility working hours affect mothers’ access to RHSs. Conversely, a Nigerian study revealed that inconvenient health facility opening hours prevented teenagers from using reproductive healthcare [18]. A Pakistani study found that health facilities’ operating hours prevented them from providing 24/7 necessary services, jeopardizing countless lives [19].
Onono et al., in their Kenyan study, found that even though women were aware of the benefits of skilled birth attendance, other systemic factors, like opening hours or healthcare workers’ attitudes, still deterred them from delivering in health facilities [20]. Facility operating hours and the restricted number of public facilities impeded access to healthcare [21].
Regarding reproductive health service characteristics and utilization, Yemen has one of the highest maternal death rates in the Arab world, 385 per 100,000 live births [8]; without access to reproductive health services, women have an increased risk of life-threatening complications [22].
A maternal and child health voucher scheme to subsidize four services—antenatal care (ANC), delivery, postnatal care (PNC), and neonatal care (NNC)—for pregnant women would help them to overcome financial barriers and would raise awareness of ANC and skilled birth attendant (SBA) delivery, which can reduce maternal and neonatal mortality. Lahj governorate mothers used ANC, delivery services by SBAs (at HFs and at home), PNC, and NNC services more than those in the Abyan governorate, and virtually all women received ANC. In Lahj, 82.5% of the interviewed mothers received ANC by a doctor, compared to 39.2% of the women in Abyan. ANC visits were likewise higher in Lahj than in the Abyan governorate. The majority (88.2%) of interviewed mothers in the Lahj governorate gave birth in a hospital attended by a trained healthcare provider, compared to 62.5% of the mothers in Abyan.
Yemen exhibits the lowest antenatal care coverage in the region, presenting numerous problems for women when it comes to institutional birth, resulting in most mothers delivering at home. The latest National Health and Demographic Survey (NHDS) for Yemen indicates that 34% of Yemeni women in rural regions receive assistance from a skilled birth attendant during childbirth, in contrast to 73% in urban areas, while only 23% of women in rural areas deliver at a health facility [23]. The factors influencing demand in Yemen for maternal health service (MHS) utilization are found to be affected by conflict, as poverty and the inability to pay, which have been worsened by the recent political situation in Yemen, cause women to neglect their health, assuming that if there are no obvious complications, it is not necessary to utilize maternal health services [17]. Previous research in Uganda, Kenya, and Pakistan has shown that coupons improve maternal care utilization [24,25,26].
In contrast, a quasi-experimental study in Kenya examined how a maternal health voucher program affected service utilization before and after free maternity services were introduced. The difference between their study and others may be due to free maternity services in non-voucher counties, which improved access to facility-based deliveries so significantly that outcomes in these areas nearly matched those in voucher-supported regions [27]. Voucher program coverage was associated with a two-fold increase in delivery at a health facility (OR: 2.1; 95% CI: 1.5–3.1) [28]. Cambodia’s voucher program improves institutional delivery. It has been linked to a 10% rise in institutional delivery and a 15.6% increase in public healthcare facility childbirth among the poorest 40% of households [29]; similar results have been found in studies in Kenya [30], Bangladesh, and Pakistan [25].
In Yemen, knowledge of family planning services is universally high, exceeding 98% across all demographics, including age, education, wealth, residency, and governorate. Women in rural areas report a lower level of knowledge (97.6%) compared to nearly all women in urban areas (99.8%) [23].
The findings of the current study indicate that in Lahj, knowledge (98.5% vs. 92.9%; p < 0.001), approval (95.8% vs. 87.4%; p < 0.001), and modern-method usage (92.3% vs. 67.8%; p < 0.001) were significantly higher compared to in Abyan, primarily sourced from public facilities (71.7% vs. 50.6%; p < 0.001). Modern methods of contraception (oral contraceptive pills, implants, injectables, contraceptive patches, vaginal rings, IUDs), were used at significantly greater rates in Lahj compared to in the Abyan governorate, whereas traditional family planning methods were more commonly used in Abyan (32.2% vs. 7.7%; p < 0.001), corroborating previous studies in Pakistan [23,24,25,26,27,28,29,30,31,32], also in other study done by Ali et al. reported a 26% increase in net percentage points for modern contraceptives in intervention areas and an 18% increase in points for IUD use was also noted [19].
In terms of uses the voucher for FP services—only for mothers in Lahj governorate were the program implemented—only 76.6% of mothers in Lahj received and used vouchers for FP services, while 9.6% received a voucher for FP, but did not use it. On the other hand, 13.8% of mothers did not care for FP vouchers, so they did not receive a voucher, and around a quarter of the mothers did not use FP services (23.4%), either because they did not receive a voucher, or they received a voucher and did not use it. Despite calls from the Ministry of Health to prioritize the distribution of family planning vouchers for free, this remains an underutilized service [33]. Targeting disadvantaged women with a locally contextualized (provincial or territorial) poverty assessment tool can improve voucher eligibility criteria for future voucher schemes.
Regarding mothers’ satisfaction, program monitoring and evaluation usually focus on service and voucher use. Some programs track quality indicators including patient satisfaction and provider knowledge. To measure mother satisfaction, we used established satisfaction-measuring instruments, including Bruce’s major criteria for RHS quality, in the questionnaire [11]. These were (1) the accessibility and environmental characteristics of the HFs, (2) the continuity and sustainability of healthcare in the HFs, (3) the communication skills of the staff and interpersonal relationships, (4) the provision of health education at the HFs, and (5) the quality of healthcare services at the HFs.
The current study found significantly higher satisfaction scores in the Lahj governorate—where vouchers were supported—compared to in the Abyan governorate—which did not implement the voucher program—across all satisfaction domains, as well as in the total satisfaction scores. The war in Yemen recently led to the months-long closure of many government facilities, including the governorate primary hospital, which explains these results. During wartime, nearby private midwifery clinics and hospitals have provided these reproductive health services to women.
The Safe Motherhood Voucher includes free family planning in its postnatal care package. User satisfaction has been investigated in many voucher program reviews. The Uganda Reproductive Health Vouchers Project (RHVP) pleased 94% of voucher users and 76% of non-voucher users. Coupon facilities also performed more comprehensive prenatal and postnatal clinical exams than non-voucher facilities [34]. In Uganda, 99% of family planning voucher recipients assessed the program as satisfactory or very good [35]. In Madagascar, 95% of voucher recipients were satisfied with the overall program [36]. According to Abuya et al., 99% of individuals who redeemed vouchers rated the services as good or very good [37].
Conversely, Kundu et al., in their study, reported that non-voucher users had higher levels of satisfaction than voucher users: 93.9% of non-voucher clients reported being satisfied or very satisfied with their service, vs. 88.4% of voucher users (p = 0.032) [38].
Also, the patient satisfaction scores in our study are consistent with many previous studies, which have shown that vouchers increase patient satisfaction as the user is at liberty to choose a provider [39]. When the voucher encompasses the total expense of services, or when the costs are the same across all providers, the holder typically makes a selection based on their impression of which provider delivers the most convenient, most comfortable, and highest-quality service [24]. This choice raises satisfaction with the service, and providers will consequently tend to raise the quality of their services to attract more voucher users [40].
The impact of vouchers on user satisfaction has been shown to be largely positive in most previous studies [24]. A thorough review identified benefits such as quality improvement and patient satisfaction. Therefore, it seems pertinent to evaluate the efficacy of voucher programs in relation to other alternative health financing methods [41].
5. Limitations
Our study faced some limitations, such as the ongoing conflict and instability, which limit access to some areas, especially in remote or conflict-prone districts (frontline health facilities). In addition, the large numbers of internally displaced persons (IDPs), including mothers, may skew population characteristics, as displacement affects access to health services and might make it hard to track consistent health behaviors or outcomes, especially in the Abyan governorate. Furthermore, variation in health facility quality between Lahj and Abyan may have influenced health outcomes independently of the voucher program. Lastly, some of the selected health facilities were non-functional due to the conflict, so they were replaced by other HFs.
6. Conclusions
The primary impacts of the voucher program in Yemen on healthcare providers and HFs included ensuring a consistent flow of funds to facilities amidst unreliable or discontinued government financing; maintaining service provision, even during the most critical phases of the crisis; enhancing local adaptability and capacity to manage drug and supply shortages; and facilitating quality-assurance support.
The vouchers enabled impoverished women and their families, frequently residing in isolated rural regions, to secure institutional deliveries without the burden of unforeseen and exorbitant expenses, such as travel with an escort, while enhancing provider selection by permitting women to choose a suitable healthcare provider nearer to their residence.
Although voucher programs provide benefits, they are not a robust health system strategy, and they fail to address the long-standing and deep-rooted health system challenges faced by fragile states. Nevertheless, fragility and instability frequently result in urgent health needs, particularly for women and adolescents, which must be addressed promptly and efficiently. We advise program implementers in precarious circumstances to utilize vouchers to sustain the provision of safe motherhood services to women in need.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1OECD States of Fragility 2015: Meeting Post-2015 Ambitions OECD Paris, France 2015
- 2Dunning C. Malknecht A. Norris J. Fragile Progress: The Record of the Millenium Development Goals in States Affected by Conflict, Fragility, and Crisis Center for American Progress Washington, DC, USA 2015
- 3Andrews R.J. Quintana L.M. Unpredictable, unpreventable and impersonal medicine: Global disaster response in the 21st century EPMA J.20156210.1186/s 13167-014-0024-925663953 PMC 4320615 · doi ↗ · pubmed ↗
- 4Grainger C.G. Gorter A.C. Al-Kobati E. Boddam-Whetham L. Providing safe motherhood services to underserved and neglected populations in Yemen: The case for vouchers Int. J. Humanit. Action 20172610.1186/s 41018-017-0021-4 · doi ↗
- 5Temmerman M. Khosla R. Bhutta Z.A. Bustreo F. Towards a new Global Strategy for Women’s, Children’s and Adolescents’ Health BMJ 2015351 h 441410.1136/bmj.h 441426371228 · doi ↗ · pubmed ↗
- 6Gorter A.C. Grainger C. Okal J. Bellows B. Systematic Review of Structural and Implementation Issues of Voucher Programs Analysis of 40 Voucher Programs In-Depth Analysis of 20 Programs Report July 2012 Population Council New York, NY, USA 2012
- 7Grainger C. Gorter A. Okal J. Bellows B. Lessons from sexual and reproductive health voucher program design and function: A comprehensive review Int. J. Equity Health 2014133310.1186/1475-9276-13-3324779653 PMC 4024100 · doi ↗ · pubmed ↗
- 8Van Hoeve E. Bushell B. Gender Equality and the Empowerment of Women and Girls in the Middle East 201911131 Available online: https://carleton.ca/bgins/wp-content/uploads/Middle-East-and-North-Africa-Country-Reports-2019.pdf(accessed on 14 May 2023)