Time trends incidence of celiac disease in a Spanish population
Julia María Cabo del Riego, María Jesús Núñez-Iglesias, Andrés Blanco Hortas, Tamara Álvarez Fernández, Ignacio Corchero, Silvia Novío, José Paz Carreira, Carmen García-Plata González, José Abel González-Ramirez, Sofia Zaera, Manuel Freire-Garabal Núñez

TL;DR
The study tracks a rising incidence of celiac disease in Spain from 2012 to 2019, with notable increases in adults and elderly.
Contribution
It provides the first detailed time-trend analysis of celiac disease incidence across age groups in Spain.
Findings
Celiac disease incidence increased from 13.11 to 20.92 per 100,000 person/year between 2012 and 2019.
The incidence in adults and elderly nearly tripled over the study period.
Classic symptoms of celiac disease became less frequent among new cases over time.
Abstract
Very few studies on celiac disease (CD) incidence across all age groups have been carried out so far, particularly in Spain. We evaluate the time trend incidence of CD of children, adults and elderly. Prospective study. Using an integrative primary and tertiary care setting approach with a standardized algorithm we identify all new cases of CD from January 1, 2012, to December 31, 2019, in a well-defined area of Galicia county, Spain. The crude incidence rate of CD was calculated as new cases per 100.000 person/year. Incidence rates were stablished by age categories 0–4, 5–19, 20–44, 45–64, 65–84, ≥ 85 and periods of 1-year intervals. Between 2012 and 2019, 19,564 patients with suspicion and risk of CD were tested. 294 new cases of CD were diagnosed. Increasing CD incidence was observed from 13.11 per 100.000 person/year in 2012 to 20.92 per 100.000 100.000 person/year in 2019 (95% CI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
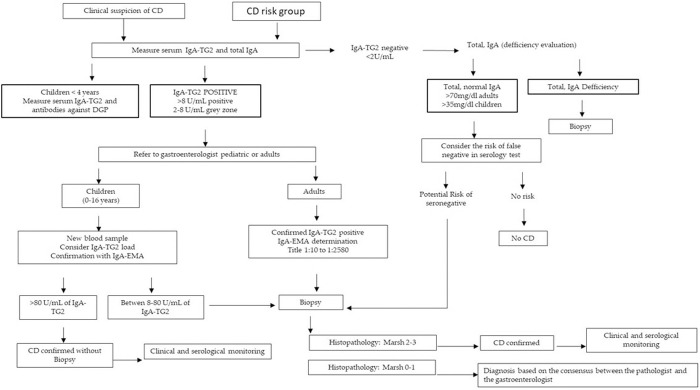 Fig 1
Fig 1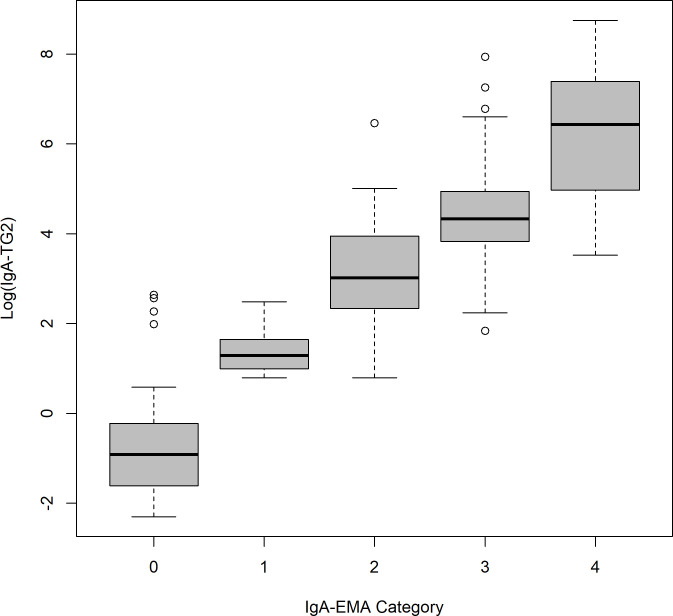 Fig 2
Fig 2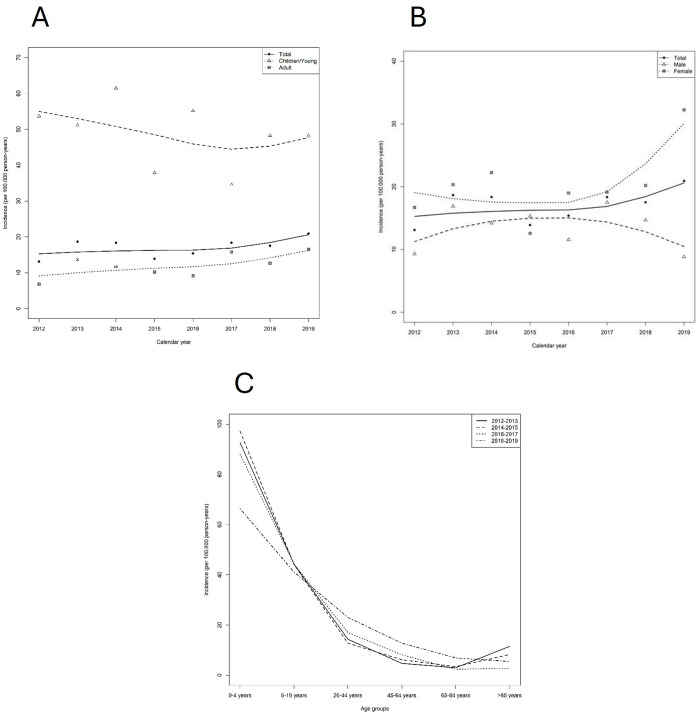 Fig 3
Fig 3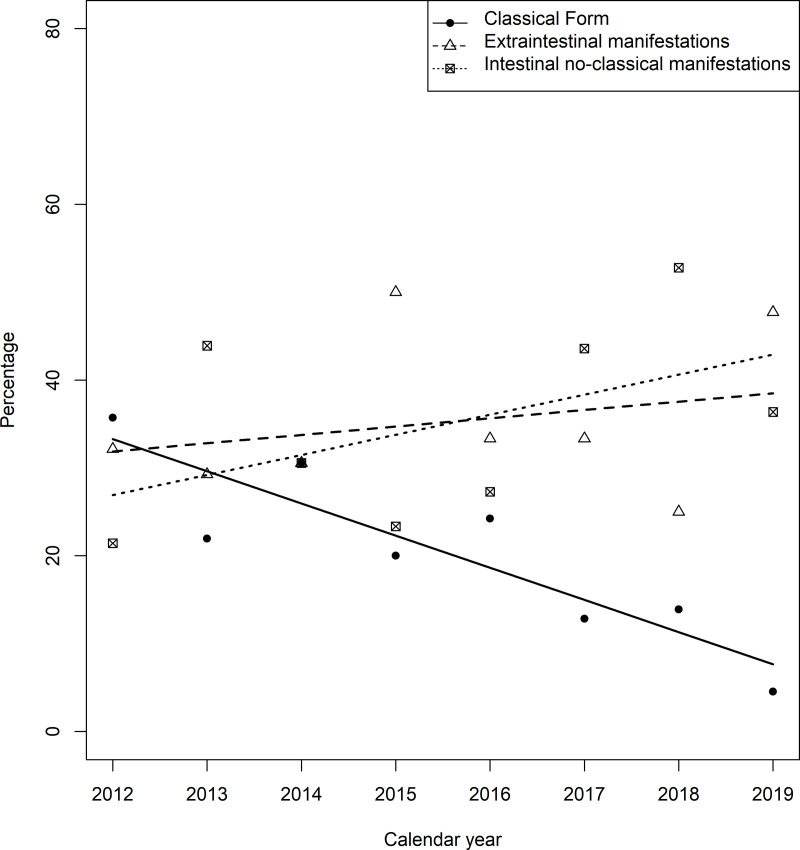 Fig 4
Fig 4- —ThermoFisher, Freiburg, Germany
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCeliac Disease Research and Management · Microscopic Colitis · Eosinophilic Esophagitis
Introduction
Celiac disease (CD) is a chronic immune-mediated disorder characterized by gastrointestinal and extra-intestinal manifestations, CD-specific autoantibodies [tissue transglutaminase 2 (TG2), endomysial (EMA) and deamidated forms of gliadin peptides antibodies], HLA-DQ2 and/or DQ8 haplotypes, and enteropathy which is developed in genetically susceptible individuals in response to gluten and related prolamins ingestion; being a gluten-free diet (GFD) an effective treatment for the majority of patients [1].
Review and meta-analysis studies showed increasing CD incidence [2–4] which varies geographically. This variation appears to be associated with several factors such as the prevalence of HLA DQ2, wheat consumption [4], age related patterns of CD presentation [4,5], race [2] as well as with testing and diagnostic paradigms [2,3,6,7]. Thus, further studies are required on the incidence of CD.
Studies are scarce on temporal trends in CD incidence, particularly including children, adults and elderly [2]. In a recent systematic review and meta-analysis [2] defining the worldwide incidence of CD (50 studies with adequate data for analysis) only 21 studies showed CD incidence across all age groups but were established with non-homogenous diagnose criteria. In this study we analyzed temporal trend in CD incidence including child, adults and elderly by using a standardized CD diagnostic algorithm, performed under control of quality [ISO, interlaboratory comparison programs for analysis and interpretation of the results (UK NEKAS SEQC), the Quality Club Control (Thermo Fisher Scientific, Uppsala, Sweden).
Furthermore, there are few studies on temporal trends in CD incidence that applied an integrative approach between different health care levels to analyze CD incidence [4,6]. In this regard, this study was based on the use of an integrative diagnostic approach between primary and tertiary health care levels. The aim of this study was to analyze the incidence of CD in a specific Galicia’s county population (Spain, Southwestern Europe) between 2012 and 2019.
Materials and methods
Setting
Galicia county, situated in the Southwest of Europe at the northwest side of Spain, is one of the 17 administrative regions that has his own health department.
Galicia´s Health System [Galician Healthcare Service (SERGAS)] is the major provider of health care in Galicia and provides universal and fairness of financing health care coverage for all residents. It is structured in 7 well-defined functional and organizational geographical health care areas which include coordinated health care (primary and tertiary referral university hospital per area from each one). SERGAS has a unique medical records linkage system.
This study was performed in Lucus Augusti University Hospital (HULA), a reference hospital for one of the above-mentioned well-defined geographical health areas.
In 2012, an integrative health care approach was initiated for CD diagnosis, including primary and tertiary health care providers, with the computerized standardization of the serological diagnostic procedure and an algorithm to confirm CD diagnose, according to the updated national and European guidelines [1,8].
From 2012 to 2019, 19,564 residents of HULA health-area with suspicion and/or at risk of CD were referred to HULA to rule out or confirm CD diagnosis.
The time frame used in our study (2012−2019) was determined by three main aspects: (1) ESPGHAN (European Society Pediatric Gastroenterology, Hepatology and Nutrition) 2012 CD diagnostic guidelines [1]; (2) 2020 update of ESPGHAN 2012 guide [9] and (3) to avoid Covid-19 pandemic (on 31 January 2020 was reported the first confirmed case of the 2019 novel Coronavirus in Spain).
CD diagnosis and data collection
Fig 1 and Table 1 show CD algorithm and diagnostic methods, respectively. Since serological and histopathological tests have a main role in CD diagnosis, the quality control process of those tests was guaranteed by internal and external quality assessment procedure including: (a) positive and negative control samples analyzed in each run; (b) accreditation UNE-EN-ISO 15189 standard of clinical laboratories (accreditation May 2011; reaccreditation 2013, 2015, 2017, 2019 and 2020); (c) participation in Interlaboratory Comparison Programs for analysis and interpretation of the results such as UK NEKAS (SEQC) United Kingdom and the Quality Club Control (Thermo Fisher Scientific, Uppsala, Sweden);(d) standardized biopsy and samples analysis by experts. Data was collected from 1 March to 18 December 2019, under pseudonymization techniques, and policy guidance by Institutional Ethic Committee according to current legislation.Informed consent was not required.
Table 1: CD diagnosis method.
Flow chart of CD diagnosis.Abbreviations: CD, Celiac disease; IgA-EMA, Endomysial IgA antibodies; IgA TG2, Tissue transglutaminase IgA antibody.
Ethical considerations
The study follows the ethical guidelines given in the Declaration of Helsinki. This study was initiated in 2012 and concluded in 2019, following the corresponding successive approvals of Institutional Ethic Committee (last code number 2019/098). Patient´s authorization and data use were performed under operational policy and procedures established by Institutional Ethic Committee and current legislation Regulation (EU) 2016/679 and Organic Law 3/2018. Authors did not have access to information that could identify individual participants during or after data collection.
Statistical analysis
Annual crude incidence rates were computed as new cases per 100,000 person/year all age ranges. Data from the Galician registry of statistics and the municipal register of inhabitants from 2012 to 2019 were used for the calculation of incidence. We tabulated incidence rates according to age categories 0–4, 5–19, 20–44, 45–64, 65–84, ≥ 85 and periods of 1-year intervals.
Results were summarized with absolute and relative frequencies in the case of categorical variables. Continuous variables were presented by mean and standard deviation. Comparison of categorical variables was performed with Chi-square test. The ANOVA test was used to compare means of IgA-EMA and IgA-TG2 and age groups. Smooth evolution of incidences along the years by gender and age groups were modeled by loess procedure (Local Polynomial Regression Fitting). Finally, ANCOVA (analysis of covariance) model was fitted to study the different CD manifestations. Statistically significant differences are considered with p < 0.05. SPSS 22.0 and R 3.6.3 were used.
Results
CD diagnosis
From 2012 to 2019, 294 new cases of CD were diagnosed. Among them, 23 (8.01%) had been identified through family screening.
Table 2 and Fig 2 show results of CD serological biomarkers diagnostic test. We observed high correlation (p < 0.001) between EMA-IgA and TG2-IgA. All patients with IgA-TG2 > 2U/ml were tested for IgA-EMA and all patients with IgA-TG2 > 80U/ml showed a statistically significant relationship with the endomysium category.
Table 2: Values of serological diagnostic biomarkers by age groups.
Correlation between IgA-TG2-and IgA-EMA.Abbreviations: IgA-TG2, IgA against specific tissue transglutaminase type 2 antibodies; EMA-IgA, endomysial IgA.
HLA genotyping was measured in 178 patients and their genetic distribution was: HLA DQ 2.5, 138 (77.53%); HLA DQ 8, 12 (6.74%); HLA DQ 2.2, 11 (6.18%); HLA DQ 2.5 + DQ8, 10 (5.62%); No DQ, 7 (3.93%).
The results of small-bowel biopsy are observed in Table 3.
Table 3: Biopsy.
Clinical manifestations exhibited a change in pattern from classical manifestations to extra-intestinal as well as intestinal non-classical ones (section temporal trends in CD incidence according to clinical manifestations).
Temporal trends in CD incidence
The overall annual incidence of CD increased from 13.11 per 100.000 person/year in 2012 to 20.92 per 100.000 person/year in 2019 (Table 3). The cases with normal or minimal alteration biopsies (Marsh 0 (n = 3) and Marsh 1 (n = 14)) were diagnosed according to serological criteria (positive IgA-TG2 confirmed with IgA-EMA), compatible clinical presentation, and/or genetic risk factors. Several of these cases belonged to risk groups and had associated diseases. After differential diagnosis with other compatible conditions, CD was considered, and GLD (gluten free diet) was initiated, leading to clinical recovery and serological normalization. Cases of gluten reintroduction or transgression, the markers elevated again, and clinical alterations recurred.
The time trends of incidence rates of CD are shown in Fig 2.
Regarding age groups (Table 4), children´s incidence was high over the entire study period in comparison to the remaining age groups (Table 4, Fig 2 A and C). Particularly, high incidence rate was observed in female children <4 years of age. In adults/elderly age groups the annual incidence rates increased over the study period. Thus, the incidence rate was 6.79 per 100,000 person/year in 2012 and 16.55 per 100,000 person/year in 2019. Specifically, in women aged 45–64 and 65–84 years, significant increase in incidence were seen compared to men in the same age ranges (Table 5; Fig 2B).
Table 4: CD incidence per 100.000 person/year (median ± CI 95%).
Table 5: CD incidence by gender and age group per 100.000 person/year.
When considering gender, divergent time trends in CD were found. Among women, incidence increased from 2016 to 2019 whereas among men, incidence has been in decline since 2016 (Fig 2B).
Temporal trends in CD incidence according to clinical manifestations
Fig 3 shows temporal tend in the proportion of CD patients with clinical manifestations. Over time the proportion of cases showing classic manifestations (diarrhea, weight lost, etc) decreased significantly (p < 0.001) while extra-intestinal, increased (anemia, osteoporosis, infertility, etc.) as well as intestinal non classical ones (abdominal distension, esophagitis, etc.) (Fig 4).
Rates of CD incidences along time adjusted by Loess Smoothing Methods.(A) By age group. (B) By gender. (C) Age trends of CD incidence by groups of 2 natural years adjusted by Loess Smoothing Method. Locally estimated scatterplot smoothing with 95% confidence intervals (dashed lines).
Temporal tends in the proportion of classical manifestations in incidence CD cases between 2012 to 2019.ANCOVA regression lines. Abbreviations: ANCOVA, analysis of covariance; CD, celiac disease.
Discussion
This study is the first Spanish study on time trend of CD incidence that includes children, adults and elderly in Spanish population. Other studies in our country are specifically targeted at children [11,12] or adults [13].
Throughout this discussion, we will contrast the main findings with those from other studies, considering methodological aspects, characteristics of the sample and other aspects that could influence the results.
We have verified an increasing CD incidence from 13.11 per 100.000 person/year in 2012 to 20.92 per 100.000 person/year in 2019. Comparing this data with those corresponding to other countries [2,4,6], reveals similar evolution. For example, Italy exhibited <4.6 per 100.000 person/year and >12.7 per 100.000 person/year before and from 2000 onwards. Nevertheless, our reported incidence is higher.
Those studies that cover approximately the last half of the 20th and the first years of the 21th century [2,14] provide discordant intra and intercountry variability. Probably due to the different aspects such as diagnostic algorithm used, coordination between the different levels of health care for the diagnosis of CD, data source for incidence calculation, screening strategies to identify CD, as well as race. In addition, other aspects can influence such as diet, gluten related factors, etc.
The number and quality of available serological and genetic tests can be confusing factors [15]. Particularly, a large variation in CD diagnostic accuracy was observed [15]. A Spanish study [16] enrolling Spanish Clinical Laboratories from the 17 administrative regions (each with their own public health care system) showed high variability in the use of serological markers of CD in primary care. To the best of our knowledge, this is the first study both in Spain and in southwestern Europe to use an algorithm in a wide sample of patients, −19,565 patients- of all ages from 0 to 87 years. We used TG2-IgA for the first-line screening. IgA-EMA test was performed in positive or borderline samples to increase positive predictive value (accreditation UNE 15189 and use the same observed for IgA-EMA). In the pediatric groups of age, intestinal biopsy was avoided according to our algorithm based on the ESPGHAN guidelines [1] when the child exhibited typical symptoms and signs of CD as well as high titters of IgA-TG2, detectable endomysial antibody, and HLA-DQ2/HLA DQ8 positivity. Nevertheless, these criteria are not used worldwide, where biopsy is still required largely in pediatric and adult cases to establish CD diagnosis.
Another aspect to consider is that CD screening strategies vary depending on the country and even the geographic area [2,3,6,13,15,17,18] and CD screening recommendations do not always achieve unanimity [4,9,19–22].
We should mention that for CD screening, and specifically on first-degree relatives, our practice is aligned with ESPGHAN guidelines [1,9], the Spanish Working Group on CD diagnosis [8] and NICE [320]. Thus, we identified 8.0% of new CD cases from first-degree relatives of CD patients. It is to note the percentage magnitude. Other studies on children from high-risk families (Leiden, the Netherlands) [23] based on predictive model) showed a cumulative incidence from 7.5% to 17.5% at 3 and 10 years of age, respectively. In Spain, a recent study [18] has verified that the screening of relatives of people with CD must be improved since family screening has not been recommended in 20% and 40% of pediatric and adult cases with CD, respectively.
If we considered gender, we verified higher CD incidence in women, particularly among adult/elderly group versus children and young people (54.1% vs. 67.4%). We attributed this finding, at least in part, to more medical testing and higher prevalence of anemia which orients to CD testing [24]. Similarly, increasing trends in female CD rates have been also reported in other countries [5]. Some studies showed that the risk of undetected CD appeared to be higher among females compared to males (RR, 1.42; 95% CI, 1.27–1.57; P < .00001) [25]. Nevertheless, it was showed that when men show diarrhea or weight loss is less likely to undergo duodenal biopsy and consequently there could be underdiagnosed [26].
CD has high prevalence in the Nordic countries or some zones of North Africa where there is a high proportion of HLA-DQ2.5 and/or DQ8 carriers. In Western Europe, the Middle East and North Africa, CD is common in paralleled to HLA-DQ2.5 and DQ8 that reach 20% and 10% [4,27]. In our Health Sanitary Area, we observed similar Haplotypes distribution [28,29]. Paraphrasing to Iversen and Sollid [30], HLA-DQ25 is considered a “chief factor” which is exhibited by around 90% of patients, showing an equal distribution between HLA-DQ2.2 and HLA-DQ8 remaining patients. Nevertheless, HLA genes are a necessary but not a sufficient factor to develop CD. Thus, only 3% of all European individuals harboring HLA-DQ2.5- or HLA-DQ8 loci that have gluten consumption develop CD [31]. In the same way, among CD patients in Spain 3% are negative for HLA-DQ2.5 and HLA-DQ8. Non-HLA risk loci could be involved in CD pathogenesis [32,33].
Regardless of the points aforementioned, other factors, which will be the subject of our future investigations, could be a contributing factor. Bread is the most common wheat-based food in Spain [34] and Galician county, where our study was conducted, is the geographical area of Spain with the highest consumption of bread [35], even compared to other countries, such as US [36] or Italy [37], where its consumption is very common. Also other gluten-related factors (vital gluten as a food additive, variations in individual diets with regard to the amount and types of wheat consumed, wheat genetics, and agronomic practices (such as nitrogen fertilization) could contribute to determining the effect of wheat [38–42] for people with the appropriate genetic susceptibility for CD; mainly those carrying the genes for particular proteins of the major histocompatibility complex, DQ2 and DQ8. Therefore, further research would be needed to evaluate such factors. Also, breastfeeding could be a potential protective factor [10,43–45]. In Spain breastfeeding is increasing [46]. Additionally, other environmental factors such as gastroenteritis or other infections could influence CD risk. As an example, H. pylori infection is associated to CD risk [43] and its seroprevalence among Spanish adult population is high [44].
The main limitation of the present study is that population is predominantly Caucasian. Thus, our data could not be extrapolated to other populations. The main strength of our study is an integrative health care approach with the availability of unique applicable algorithms under accreditation quality criteria. In our study there was used a standard computerized algorithm used by the physicians and pediatrics of primary care as well as hospital pediatricians and gastroenterologists of a well-defined health area (see Methods section). Murray et al. [5] or Ludvigson et al. [6] were precursors in postulating an integrative approach between health care providers.
Conclusions
A increase in incidence of CD between 2012 and 2020 has been observed. Standardized algorithm for CD diagnosis with first-line serology testing followed by biopsy, if needed, confirmed the CD incidence increase over 8 years period.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Husby S, Koletzko S, Korponay-SzabóIR, Mearin ML, Phillips A, Shamir R, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54(1):136–60. doi: 10.1097/MPG.0b 013e 31821 a 23d 0 22197856 · doi ↗ · pubmed ↗
- 2King JA, Jeong J, Underwood FE, Quan J, Panaccione N, Windsor JW, et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am J Gastroenterol. 2020;115(4):507–25. doi: 10.14309/ajg.0000000000000523 32022718 · doi ↗ · pubmed ↗
- 3Roberts SE, Morrison-Rees S, Thapar N, Benninga MA, Borrelli O, Broekaert I, et al. Systematic review and meta-analysis: the incidence and prevalence of paediatric coeliac disease across Europe. Aliment Pharmacol Ther. 2021;54(2):109–28. doi: 10.1111/apt.16337 34115894 · doi ↗ · pubmed ↗
- 4Kang JY, Kang AHY, Green A, Gwee KA, Ho KY. Systematic review: worldwide variation in the frequency of coeliac disease and changes over time. Aliment Pharmacol Ther. 2013;38(3):226–45. doi: 10.1111/apt.12373 23782240 · doi ↗ · pubmed ↗
- 5Murray JA, Van Dyke C, Plevak MF, Dierkhising RA, Zinsmeister AR, Melton LJ 3rd. Trends in the identification and clinical features of celiac disease in a North American community, 1950–2001. Clin Gastroenterol Hepatol. 2003;1:19–27.15017513 10.1053/jcgh.2003.50004 · doi ↗ · pubmed ↗
- 6Ludvigsson JF, Rubio-Tapia A, van Dyke CT, Melton LJ 3rd, Zinsmeister AR, Lahr BD, et al. Increasing incidence of celiac disease in a North American population. Am J Gastroenterol. 2013;108(5):818–24. doi: 10.1038/ajg.2013.60 23511460 PMC 3686116 · doi ↗ · pubmed ↗
- 7Norström F, Myléus A, Nordyke K, Carlsson A, Högberg L, Sandström O, et al. Is mass screening for coeliac disease a wise use of resources? A health economic evaluation. BMC Gastroenterol. 2021;21(1):159. doi: 10.1186/s 12876-021-01737-1 33836647 PMC 8034082 · doi ↗ · pubmed ↗
- 8Ministerio de Sanidad. Protocolo para el diagnóstico precoz de la enfermedad celíaca. Ministerio de Sanidad, Servicios Sociales e Igualdad. Servicio de Evaluación del Servicio Canario de la Salud (SESCS); 2018.