Assessing the Therapeutic Role of Rehabilitation Programs in Chemotherapy-Induced Peripheral Neuropathy (CIPN)—A Scoping Review
Yazan A. Al-Ajlouni, Omar Al Ta’ani, Sophia A. Zweig, Magdalena Bak, Mohammad Tanashat, Ahmed Gabr, Zaid Khamis, Farah Al-Bitar, Mohammad Islam

TL;DR
This review explores how rehabilitation programs can help manage chemotherapy-induced nerve damage, showing that exercises and complementary therapies may improve symptoms and quality of life for cancer patients.
Contribution
The study provides a comprehensive overview of rehabilitation interventions for CIPN, emphasizing the integration of physical and complementary therapies into standard care.
Findings
Physical modalities like ultrasound and exercise showed promise in relieving CIPN symptoms in colorectal and breast cancer patients.
Complementary therapies such as acupuncture and yoga were effective in managing CIPN symptoms.
No distinct advantage was found in the timing of exercise interventions for CIPN.
Abstract
Background: Chemotherapy-induced peripheral neuropathy (CIPN) is a common, debilitating side effect of cancer treatment. Characterized by symptoms like pain, numbness, and muscle weakness, CIPN significantly impacts patients’ quality of life. Current management strategies vary, with limited consensus on effective treatments. This scoping review aims to explore comprehensive rehabilitation interventions for CIPN, focusing on enhancing patient well-being and functional abilities. Methods: A scoping review, guided by Arksey and O’Malley’s framework and Levac et al.’s refinements, was conducted to assess rehabilitation programs for CIPN. Searches across six databases were performed, with inclusion and exclusion criteria focusing on studies with physical rehabilitation interventions. Data were charted, detailing interventions, demographics, and outcomes. Results were synthesized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
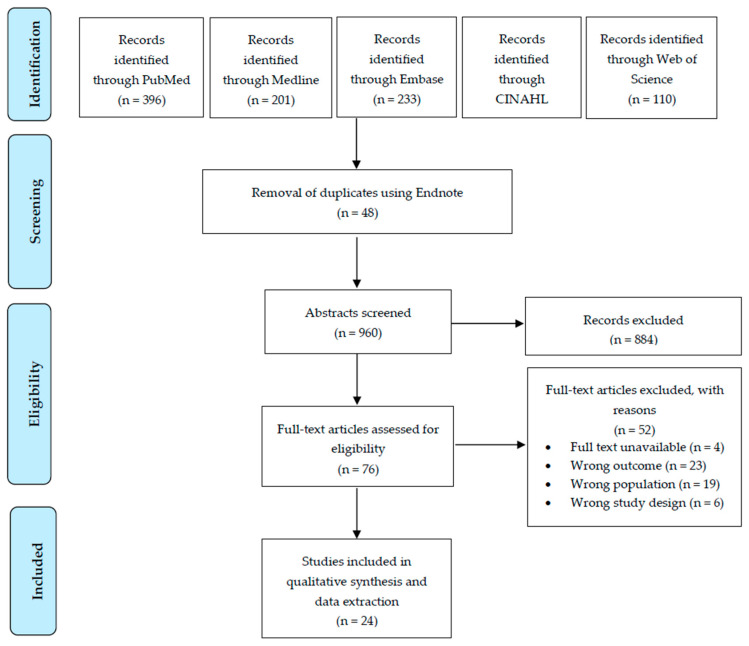 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Treatment and Pharmacology · Chemotherapy-related skin toxicity · Pain Mechanisms and Treatments
1. Introduction
Chemotherapy-induced peripheral neuropathy (CIPN) stands as a significant and often debilitating side effect of cancer treatment, casting a shadow over the lives of countless patients battling this formidable disease. As a neurological disorder triggered by the administration of chemotherapeutic agents, especially those that are platinum-based (e.g., Cisplatin), CIPN encompasses a wide spectrum of symptoms, including tingling sensations, numbness, pain, and muscle weakness, which typically manifest in the hands and feet [1]. Several conditions may be associated with CIPN including autonomic dysfunction, sleep disturbances, fatigue, and mood disorders such as anxiety and depression [2]. These conditions can worsen the functional impairments and can significantly reduce quality of life. CIPN follows a glove-and-stocking pattern with symmetric loss of sensation in distal extremities. Symptoms may persist in some cases after the completion of chemotherapy, causing long-term disability, gait instability, and increased risk of falls [3].
The prevalence of CIPN among patients receiving chemotherapy varies widely, with estimates ranging from 12% to 96% [2,4,5], depending on the specific drugs and dosages administered [6]. Beyond the physical discomfort it inflicts, CIPN holds profound implications for the overall well-being and treatment outcomes of individuals already grappling with the burdens of cancer [7,8]. This variability in CIPN’s impact stresses the need for effective management strategies to address the wide-ranging challenges it poses to patients.
To date, the evidence regarding CIPN’s management continues to be inconsistent, with some reports concluding that neuropathies cannot be treated, and protective treatment strategies have not been significantly effective [9]. Other reports have suggested positive treatment efforts, including decompression surgery [10] and pharmacological strategies [11,12]. Furthermore, emerging research in the literature has explored the role of exercise in the management of CIPN’s symptoms. For instance, previous systematic reviews reported significant improvements in postural control, quality of life, muscular strength, and independence [13,14].
Furthermore, CIPN’s symptoms extend beyond physical manifestations to an emotional toll on patients, especially as they fear compromised treatment efficacy. Consequently, this makes it imperative to address CIPN using a comprehensive approach, one that not only addresses the physical symptoms but also seeks to enhance patients’ overall quality of life. In this context, emerging strategies within the field of Physical Medicine and Rehabilitation (PM&R) offer promising avenues for improving the well-being of cancer patients undergoing chemotherapy. PM&R, as a specialty that primarily focuses on enhancing patients’ functional abilities and quality of life, may hold the key to effective CIPN management by providing holistic interventions that extend beyond pharmacological or surgical approaches. To date, and to the best of our knowledge, there has been limited exploration in the literature reviewing the evidence of comprehensive rehabilitation approaches for CIPN. Previous research has predominantly focused on exercise programs and behavioral interventions [15,16]. However, considering the increasing attention to the long-term effects of CIPN and the potential impact of rehabilitation on improving patients’ functions and quality of life [17], a scoping review of the extent of multidisciplinary rehabilitation programs on CIPN could significantly enhance our understanding in this domain.
In light of these considerations, this study aimed to conduct a scoping review to explore the breadth and depth of comprehensive rehabilitation interventions for CIPN. By encompassing a wider range of rehabilitation interventions, this scoping review aims to provide a more holistic view of the strategies employed to address CIPN. The insights gained from this review are expected to inform clinical practice and aid in the development of tailored rehabilitation interventions that meet the specific needs of patients with CIPN. This is particularly pertinent given the global expansion of PM&R, a field inherently multidisciplinary in nature, emphasizing a holistic approach to patient care that integrates various therapeutic modalities to optimize function and quality of life.
2. Methods
A scoping review was conducted following the methodological framework suggested by Arksey and O’Malley [18] and further refined by Levac et al. [19]. This approach was chosen instead of PRISMA-ScR to explore the breadth of literature and map the key concepts and evidence concerning rehabilitation programs on CIPN. This review was not registered on a platform such as the Open Science Framework, as its primary goal was exploratory conceptual mapping rather than hypothesis testing—a common practice for Arksey and O’Malley-based scoping reviews.
While PRISMA-ScR is a valuable tool for structured reporting [20], our review adopted the Arksey and O’Malley framework [18], refined by Levac et al. [19], as it better aligns with our exploratory aims to map broad evidence rather than answer a narrow clinical question. This approach emphasizes iterative literature engagement and conceptual mapping, which was critical given the heterogeneity of CIPN rehabilitation interventions. However, to enhance transparency, we now include a PRISMA-ScR checklist (Table S1) and flow diagram (Figure 1).
2.1. Search Strategy and Selection Criteria
This study sought to examine what is known about the effects of rehabilitation programs on CIPN from the existing literature. A comprehensive search strategy was designed using a set of developed keywords (outlined in Table S2 in the Supplementary File). Searches were conducted across multiple databases: (1) PubMed; (2) PsycINFO; (3) Web of Science; (4) EMBASE; (5) ScienceDirect; (6) CINAHL. Boolean operators were used to enhance the search.
Initial search results (n = 1008) were managed using Endnote reference manager software (Endnote X9.3.3). After duplicate removal (n = 48), titles and abstracts of unique search results (n = 960) were screened for relevance by two independent reviewers (Y.A.A and M.T). The inclusion and exclusion criteria were iteratively developed and refined during the screening process, with emphasis on studies involving human subjects, published in English, and focusing on physical rehabilitation interventions for patients with CIPN. Table S3 in the supplementary file details the complete eligibility criteria post-screening.
2.2. Data Charting
Data charting was performed to identify and outline the breadth and variety of studies in the domain of rehabilitation programs for CIPN. A data charting form was developed and employed to systematically extract and organize key information from each study.
The parameters extracted included a detailed description of the physical intervention along with its duration. Additionally, information about the comparator group or any other intervention was noted, including a full description and the duration of these interventions. The sample size of each study was recorded, as well as demographic data such as mean age (with standard deviation), gender distribution (expressed as number and percentage), and the cause of neuropathy. Further details were charted about the type of chemotherapy used, the cancer types treated, and any other treatments administered alongside the primary intervention.
A crucial aspect of charting involved documenting the signs of neuropathy as reported in each study, providing insights into the clinical presentation of CIPN in the context of the rehabilitation programs. Lastly, the main findings of each study were extracted, focusing particularly on the outcomes and effectiveness of the rehabilitation interventions compared to the comparators.
This meticulous process of data charting was initiated by a single reviewer and was subsequently validated by the coauthors to ensure accuracy and comprehensiveness. The data collected offers a panoramic view of the current research landscape on rehabilitation interventions for CIPN, highlighting varied approaches, methodologies, and findings across different studies.
2.3. Data Presentation and Analysis
Data were synthesized descriptively, focusing on mapping the extent, range, and nature of the research activity in this field. The results were presented in a tabular format and accompanied by a narrative summary that highlights key trends, demographic characteristics, types of interventions, and reported outcomes in the studies reviewed.
3. Results
The identified studies examined various physical interventions for the treatment of CIPN. Studies by Al Onazi et al. and Hammond et al. delve into physical modalities, with ultrasound therapy exhibiting promise for colorectal cancer patients and home exercises showing potential benefits for those with breast cancer. Bland et al. explored exercise timing, revealing no distinct advantages in immediate versus delayed supervised training for breast cancer patients. Complementary therapies, such as acupuncture, demonstrated effectiveness, suggesting a role in managing CIPN symptoms. Furthermore, yoga interventions [21] and transcutaneous electrical nerve stimulation [22] displayed positive outcomes.
3.1. Overview of Studies Included
The review consists of 24 studies published from 2019 to 2023. Geographically, the studies cover diverse regions: Canada [23,24], the USA [22,25,26], Sweden [27], Israel [28], China [29], Iran [29], Japan [30], Turkey [31], Germany [32,33], Republic of Korea [34], and India [35]. The reviewed papers examine multiple cancer types, including colorectal [24,29,36,37,38], breast [23,28,29,31,36,39,40,41], as well as many others like lung, ovarian, prostate, colorectal, colon, rectum, gynecological, and lymphoma [26,29,36,41]. Diverse chemotherapy medications were used, with the most prominent being oxaliplatin [21,22,24,30,38,41] and paclitaxel [22,25,28,30,31,34,35,39,41,42,43]. The characteristics of the included studies are summarized in Table 1.
3.2. Comparators Used in Studies
The studies included in the review employed diverse control interventions and standard care approaches for comparison. Common control interventions involved a placebo [34,36] or sham treatment [39] to assess the specific effects of the intervention under investigation. Additionally, some studies compared the intervention against standard care practices [23,24,28,41] ensuring a benchmark for evaluating its efficacy.
3.3. Types and Efficacy of Interventions
Figure 2 illustrates the various interventions identified in this scoping review, as described in detail in this subsection.
3.3.1. Aerobic Exercise
Bland et al. [43] studied the impact of immediate versus delayed exercise (IE vs. DE), including physical intervention (aerobic exercise) such as immediate exercise (supervised aerobic, resistance, and balance training), which was offered 3 days a week for 8–12 weeks. Although the exercise interventions showed no significant differences in managing CIPN, both groups experienced increased sensory and motor symptoms during chemotherapy, with recovery post-treatment, and the IE group reported a lower percentage of participants with numbness in the toes or feet at pre-cycle 4 compared to the DE group.
3.3.2. Resistance Training
In examining the effectiveness of resistance training as an intervention for CIPN, several studies have presented compelling evidence. Streckmann et al. and Zimmer et al. both highlighted the benefits of supervised exercise programs, which encompassed resistance training among other activities [32,33,38,43].
Streckmann et al. conducted two pivotal studies, each exploring different facets of exercise interventions. In their first study [33], the intervention group underwent supervised exercise twice a week for 1 h each over 36 weeks, incorporating activities like cycling or treadmill walking, postural stabilization tasks, and resistance exercises. The control group continued chemotherapy without structured exercise. The intervention group showed significant improvements in quality of life, constipation, diarrhea, and pain, with a lower incidence of peripheral neuropathy (PNP) compared to the control group. The intervention group also exhibited increased activity levels and improved balance control. In Streckmann et al.’s other study [32], participants engaged in supervised training twice a week for 6 weeks, with two intervention arms: sensorimotor training (SMT) and whole-body vibration training (WBV). SMT involved progressively challenging balancing exercises, while WBV utilized a vibration platform. The SMT group demonstrated improved Achilles and patellar tendon reflexes compared to the control group, with reduced pain and dyspnea. The WBV group also showed improvements in pain and dyspnea.
Adding to the body of evidence on the topic, Zimmer et al. [38] conducted an eight-week supervised exercise program for individuals who had undergone chemotherapy. The program included endurance, resistance, and balance training conducted twice weekly for 60 min each session. The control group received written standard recommendations to achieve physical fitness. The participants had colorectal cancer and were exposed to oxaliplatin-based chemotherapy. The exercise group exhibited improved physical fitness and quality of life compared to the control group, which received only written standard recommendations for physical activity.
3.3.3. Balance and Flexibility Exercises and Mind–Body Therapies
This subsection explores the promising role of balance, flexibility exercise, and mind–body therapies. These exercises encompass practices like yoga, tai chi, qigong, and mindfulness techniques. They aim to enhance both physical and mental well-being through a combination of physical postures, controlled breathing, and meditation.
In a study by Galantino et al. [27], cancer survivors with CIPN participated in somatic yoga and meditation (SYM) sessions twice a week for 8 weeks. These 90 min sessions, led by certified yoga instructors, aimed to address the sensory and motor deficits associated with CIPN. Somatic movements use pandiculation, voluntary muscular contraction, and slow, controlled decontraction (eccentric contraction), with a constant focus on sensation, to increase the resting length of muscles. The study found that SYM had positive effects on both clinical measurements and patient-reported symptoms, indicating its potential in improving proprioceptive signals, enhancing postural control, and reducing the risk of falls.
Similarly, Knoerl et al. [21] conducted research involving 28 individuals with CIPN, predominantly comprising older women who had undergone various chemotherapy regimens. The participants engaged in at least 12 modified Hatha yoga sessions over 8 weeks. The study reported that yoga brought about improvements in well-being across different cancer types and chemotherapy regimens.
Zhi et al. [25] further contributed to this body of research by examining the effects of an 8-week yoga intervention on individuals who had completed neurotoxic chemotherapy. Participants engaged in daily 60 min yoga sessions, which included breathwork (pranayama) and adaptable postures (asanas). The yoga group showed significant reductions in pain, improvements in neuropathy-specific quality of life (FACT/GOG-Ntx scores), and enhanced functional reach, which is crucial in predicting fall risk.
Furthermore, Ben-Arye et al. [28] investigated the impact of complementary integrative medicine (CIM) on patients with breast or gynecological cancer undergoing taxane-based chemotherapy or those with hematological malignancies receiving neurotoxic treatments. In the intervention arm, patients received twice-weekly CIM sessions for 6 weeks, including acupuncture and other manual or mind–body therapies. During the baseline-to-6-week assessments, participants in the intervention group experienced notable improvements in emotional well-being and overall FACT-Tax scores compared to the control group. Specifically, they reported reduced hand numbness/tingling and discomfort, along with enhanced physical functioning as measured by the EORTC scale. Additionally, both intervention groups (A and B) showed significant enhancements in various aspects of quality of life, including physical well-being, total FACT-Tax score, and reduction in feet discomfort. Moreover, there were improvements in EORTC pain scores.
3.3.4. Physical Therapy Interventions
This subsection delves into the impact of physical therapy interventions on CIPN, drawing from studies by Ikio et al. and Al Onazi et al. [24,30].
Ikio et al. [30] focused on muscle strength exercises, manual dexterity training, and sensory function training among patients with hematological or gastrointestinal malignancies. The intervention group demonstrated a substantially lesser decline in activities of daily living compared to the control group at the second time point (defined in the trial as two chemotherapy cycles), as measured by the Michigan Hand Outcomes Questionnaire (MHQ). This was evident in both intention-to-treat and as-treated analyses, with notable improvements in pain management.
Al Onazi et al. [24] explored the combination of ultrasound therapy (3 cm transducer, 3 MHz frequency, and continuous ultrasound at an intensity of 0.7–0.8 w/cm^2^ for 5 min to each location), with a home exercise regimen in colorectal cancer patients experiencing chemotherapy-induced hand and foot pain. Over the first two weeks, participants underwent 10 sessions of ultrasound therapy, applying a 3 cm transducer with a frequency of 3 MHz and continuous ultrasound at an intensity of 0.7 to 0.8 w/cm² for 5 min to each location (fingers and toes/base of feet). The standard care group followed a 6-week regimen comprising education on CIPN, a home exercise program, and education on self-care strategies.
3.3.5. Complementary Therapies
The exploration of complementary therapies in the treatment of CIPN has gained notable attention, as seen in studies by Iravani et al., Greenlee et al., and Izgu et al. [29,31,39]. These research efforts delve into the potential of acupuncture, electro-acupuncture, and classical massage as viable treatment options.
Iravani et al. [29] examined the effectiveness of acupuncture for CIPN among a group of nineteen participants predominantly diagnosed with breast and colorectal cancer. The study found that acupuncture not only safely treated CIPN but also showed superior efficacy compared to conventional treatments such as vitamin B1 and gabapentin.
Greenlee et al. [39] conducted a study to assess the impact of electro-acupuncture (EA) on CIPN in patients with stage I–III breast cancer receiving paclitaxel. This study included 63 participants and used a sham electro-acupuncture (SEA) group as a control. Each group received their respective treatments over a 12-week period. However, patients in the EA group reported worse peripheral neuropathy symptoms than those in the SEA group.
Lastly, Izgu et al. [31] explored the role of classical massage therapy in managing paclitaxel-induced CIPN, particularly in breast cancer patients. Over 12 weeks, nineteen participants received massage sessions aimed at reducing neuropathic pain and enhancing quality of life (QOL). The results showed significant reductions in neuropathic pain and improvements in both sensory and motor QOL sub-scale scores for the massage group. Additionally, the sensory action potential amplitude of the median nerve was significantly higher, and the tibial nerve latency was significantly shorter in the CMG compared to the CG at week 12.
4. Discussion
This scoping review explores various physical interventions for managing CIPN, a prevalent and debilitating side effect among cancer patients. Encompassing a diverse array of modalities—from aerobic and resistance exercises to mind–body therapies and tailored physical therapy interventions—this review synthesizes findings from studies conducted across various global contexts. Its primary objective was to evaluate the efficacy and applicability of these interventions in alleviating CIPN symptoms across different cancer types and chemotherapy regimens, with a special focus on prevalent drugs like oxaliplatin and paclitaxel. Our review not only highlights key outcomes such as enhanced quality of life, effective pain management, improved physical fitness, and reduced neuropathy symptoms but also sheds light on the long-term benefits and sustainability of these interventions, thereby offering a comprehensive perspective on potential therapeutic strategies for CIPN.
The integration of physical exercises, particularly aerobic and resistance training, into the management of CIPN suggests potential benefits. The results of studies examining these interventions [32,33,38,43] indicate that these forms of exercise may play a role in both alleviating existing CIPN symptoms and preventing their severity. Aerobic exercises have been associated with improvements in overall patient well-being [44,45], while resistance training may enhance muscle strength and functional capacity [46,47]. These studies collectively underscore the pivotal role of structured, supervised physical exercise regimens in managing CIPN. They demonstrate that a diverse range of physical activities, tailored to the needs of chemotherapy patients, can substantially improve not only their physical well-being but also their overall quality of life. This evidence advocates for the integration of such exercise programs into standard care protocols for CIPN management, emphasizing the need for personalized, patient-centered approaches in oncology care. This evidence suggests that a combined approach of both aerobic and resistance exercises might offer a more holistic management strategy for CIPN.
The impact of the timing of these exercise interventions also emerges as an area of interest [43]. Despite some inconclusive results, initiating exercise programs early in the chemotherapy process could influence the development and severity of CIPN. This hypothesis aligns with current research indicating the importance of early intervention in managing chronic conditions [48,49]. Moreover, the focus on supervised training underscores the need for personalized and safe exercise regimens. Supervised exercises ensure patient safety [50,51] and could optimize therapeutic outcomes, possibly leading to improvements in neuropathy symptoms and quality of life. These insights, while preliminary, suggest the potential for integrating structured exercise into standard CIPN management protocols.
Furthermore, balance, flexibility exercises, and mind–body therapies, such as yoga, have emerged as promising complementary approaches. The outcomes of these interventions point toward notable improvements in proprioception and balance, which are critical for patients experiencing the disorienting effects of CIPN. Additionally, these therapies have shown effectiveness in managing pain, a primary concern for many undergoing chemotherapies [52]. Yoga has an integrative approach, which utilizes a combination of physical movement, breathing exercises, and mindfulness and has shown promising results among mind–body therapies. Gentle yoga for CIPN patients focuses on balance, stretching, and relaxation, which can be adapted to accommodate sensory deficits and muscle weakness. Studies have shown that yoga improves pain, balance, fatigue, and psychological outcomes among cancer survivors, including those with CIPN [53,54]. It is imperative to consider the implementation of such practices under expert supervision, especially in oncology, to ensure safety and efficacy.
By improving sensory and motor functions, reducing pain, and enhancing quality of life, these non-pharmacological approaches offer valuable complementary strategies for CIPN management in cancer survivors. Their adaptability across various cancer types and chemotherapy regimens further underscores the potential of incorporating these practices into holistic care plans for individuals suffering from CIPN. Beyond physical benefits, these practices have a profound impact on the overall quality of life, offering a holistic approach to managing the multifaceted challenges of CIPN. The therapeutic value of these interventions, as suggested by current research, lies not only in their physical aspects but also in their ability to address the psychological and emotional strains faced by patients [55,56,57]. This dual impact on both physical and mental health positions these therapies as valuable components of comprehensive CIPN management strategies.
Physical therapy interventions have shown promise in the management of CIPN, offering a range of techniques tailored to individual patient needs. These interventions, ranging from specific exercises and ultrasound therapy to comprehensive approaches that integrate acupuncture and exercise, demonstrate substantial promise in improving patient experiences. Among these, muscle strength exercises and sensory function training stand out. While muscle strength exercises focus on the physical debilitations of CIPN, sensory function training addresses the nuanced sensory deficits, aiding in the re-establishment of proprioception and coordination, enhancing functionality, and improving daily living activities [24,30]. Their effectiveness is evident in enhancing daily activities, alleviating pain, and elevating the overall quality of life for individuals undergoing chemotherapy. These studies collectively reinforce the importance and potential of physical therapy as a critical component in the management of chemotherapy-induced complications.
Additionally, the emerging role of ultrasound therapy in CIPN symptom management represents an innovative and increasingly popular approach. Its non-invasive nature offers potential benefits in pain relief and nerve regeneration, although the underlying mechanisms are still under investigation. These sessions often include a variety of therapeutic practices targeting both physical and psychological aspects of CIPN. Thus, the combined use of traditional physical therapy approaches with innovative techniques like ultrasound therapy and CIM sessions demonstrates the evolving landscape of CIPN management, acknowledging the need for multifaceted treatment strategies.
Finally, our review has also shown that complementary therapies, notably acupuncture and massage therapy, are gaining traction in the management of CIPN, as highlighted in recent studies. Acupuncture, with roots in traditional Chinese medicine, has shown promise in reducing CIPN symptoms, potentially offering an alternative for patients who have limited relief from traditional Western treatments. Its efficacy in alleviating pain, tingling, and numbness, as evidenced by Iravani et al., positions it as a valuable option in the CIPN treatment arsenal. Similarly, massage therapy, as explored by Greenlee et al. and Izgu et al. [31,39], has been associated with not only symptomatic relief but also improvements in overall patient well-being. While acupuncture and massage show potential benefits, the varied outcomes with electro-acupuncture indicate a complex landscape, necessitating further research to fully understand and optimize these therapies for CIPN management. The safety profiles of both acupuncture and massage therapy add to their appeal, presenting minimal risks when conducted by trained professionals. The implications of these findings are significant for current treatment practices; they further highlight the need for a more integrative approach to patient care, embracing complementary therapies as part of a holistic treatment plan. This shift not only aligns with patient preferences for non-pharmacological interventions but also addresses a broader spectrum of CIPN symptoms, thereby enhancing the quality of life for cancer survivors. Collectively, these studies illuminate the promising role of complementary therapies in managing CIPN, offering alternative or adjunctive options to traditional medical treatments.
4.1. Clinical Implications
The findings of this scoping review emphasize the necessity of integrating diverse physical interventions, including aerobic and resistance exercises, balance and flexibility exercises, and mind–body therapies such as yoga, into the standard care protocols for CIPN. These interventions, tailored to individual patient needs and conditions, hold significant promise in not only alleviating CIPN symptoms but also in enhancing overall patient well-being. There is a critical need for healthcare professionals to be educated and trained in these varied techniques to ensure safe and effective administration. Furthermore, early intervention strategies, particularly for patients at high risk or in the initial stages of chemotherapy, could potentially mitigate the severity of CIPN symptoms. This proactive approach, coupled with patient education and involvement in treatment decisions, may lead to better adherence to therapy and improved outcomes.
Additionally, the growing evidence supporting complementary therapies like acupuncture and massage therapy in CIPN management suggests that these should be more widely integrated into treatment plans, especially for patients seeking non-pharmacological options. These treatment options are often not covered by insurance [58,59,60]; thus, healthcare systems and insurance policies would need to adapt to include these therapies to make them more accessible and affordable. By embracing these clinical implications and strategies, healthcare providers can significantly enhance the quality of life and care for patients suffering from CIPN, marking a pivotal shift in the current management paradigm of this challenging condition.
4.2. Limitations and Future Research
This review has several limitations. Firstly, the nature of a scoping review may limit the depth of analysis for each specific intervention. This approach, while beneficial for mapping the range of evidence, does not provide the detailed assessment of quality and robustness that systematic reviews offer. Variations in study designs across the reviewed research introduce challenges in synthesizing and comparing findings, potentially affecting the robustness of our conclusions. Many studies reported general quality-of-life improvements without CIPN-specific quantitative metrics (e.g., neuropathy scales or pain scores), limiting our ability to assess direct impacts on neuropathy symptoms. Moreover, the notable heterogeneity in the types of intervention, outcomes, and patient characteristics among included studies makes it arduous to reach a definitive conclusion regarding the effectiveness of specific interventions. While several interventions have reported desirable outcomes, these should be interpreted with caution. Additionally, the diversity in sample sizes, which ranged from small pilot studies to larger trials, may influence the generalizability of the results. The geographic distribution of the studies also presents a limitation, as the majority are concentrated in certain regions, potentially limiting applicability across diverse populations and healthcare systems.
Future research should focus on addressing these gaps by conducting studies with uniform design methodologies and larger, more diverse sample populations. This would enable more definitive conclusions about the efficacy and applicability of various interventions for CIPN. Further, research efforts could benefit from a more focused approach, such as systematic reviews or meta-analyses, to provide a deeper understanding of specific interventions. Expanding research to include a wider geographic spread can ensure that findings are relevant and adaptable globally. Investigating the long-term effects of these interventions and their impact on the progression of CIPN symptoms would also be valuable. Additionally, exploring the underlying mechanisms through which these therapies exert their benefits could offer insights into novel treatment approaches and refine existing ones for better patient outcomes.
5. Conclusions
In conclusion, this scoping review has illuminated the diverse landscape of physical and complementary interventions for managing CIPN, revealing significant potential in improving patient outcomes. Our comprehensive analysis highlights that incorporating a multifaceted approach, encompassing aerobic and resistance exercises, tailored physical therapy, mind–body practices, and emerging complementary therapies like acupuncture and massage therapy, can effectively alleviate CIPN symptoms and enhance the overall quality of life for cancer patients. These findings advocate for a paradigm shift in CIPN management, urging the integration of these varied interventions into standard care protocols and patient-specific treatment plans. As the landscape of CIPN management continues to evolve, it becomes imperative for healthcare systems to adapt, prioritizing patient-centered, holistic care approaches that address both the physical and psychological aspects of this challenging condition. This review paves the way for future research and clinical practice to focus on more comprehensive, personalized, and proactive strategies in the battle against the debilitating effects of CIPN.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boyette-Davis J.A. Hou S. Abdi S. Dougherty P.M. An updated understanding of the mechanisms involved in chemotherapy-induced neuropathy Pain Manag.2018836337510.2217/pmt-2018-002030212277 PMC 6462837 · doi ↗ · pubmed ↗
- 2Seretny M. Currie G.L. Sena E.S. Ramnarine S. Grant R. Mac Leod M.R. Colvin L.A. Fallon M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis Pain 20141552461247010.1016/j.pain.2014.09.02025261162 · doi ↗ · pubmed ↗
- 3Smith E.M. Pang H. Cirrincione C. Fleishman S. Paskett E.D. Ahles T. Bressler L.R. Fadul C.E. Knox C. Le-Lindqwister N. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: A randomized clinical trial JAMA 20133091359136710.1001/jama.2013.281323549581 PMC 3912515 · doi ↗ · pubmed ↗
- 4Eckhoff L. Knoop A.S. Jensen M.B. Ewertz M. Persistence of docetaxel-induced neuropathy and impact on quality of life among breast cancer survivors Eur. J. Cancer 20155129230010.1016/j.ejca.2014.11.02425541155 · doi ↗ · pubmed ↗
- 5Osmani K. Vignes S. Aissi M. Wade F. Milani P. Lévy B.I. Kubis N. Taxane-induced peripheral neuropathy has good long-term prognosis: A 1- to 13-year evaluation J. Neurol.20122591936194310.1007/s 00415-012-6442-522349867 · doi ↗ · pubmed ↗
- 6Quasthoff S. Hartung H.P. Chemotherapy-induced peripheral neuropathy J. Neurol.200224991710.1007/PL 0000785311954874 · doi ↗ · pubmed ↗
- 7Zhang X. Chen W.-W. Huang W.-J. Chemotherapy-induced peripheral neuropathy Biomed. Rep.2017626727110.3892/br.2017.85128451384 PMC 5403454 · doi ↗ · pubmed ↗
- 8Simão D.A.d.S. Murad M. Martins C. Fernandes V.C. Captein K.M. Teixeira A.L. Chemotherapy-induced peripheral neuropathy: Review for clinical practice Rev. Dor 20151621522010.5935/1806-0013.20150043 · doi ↗