Combining Self-Reported Information with Radiographic Bone Loss to Screen Periodontitis: A Performance Study
José João Mendes, Margarida Neves, Clara Supiot, Leonor Pinto, Diogo Tenda, Nuno Silva, Luís Proença, Yago Leira, Vanessa Machado, João Botelho

TL;DR
This study shows that combining self-reported data with radiographic bone loss can effectively screen for periodontitis, especially when full exams are not possible.
Contribution
The study introduces a combined screening method for periodontitis using self-reports and radiographic bone loss data.
Findings
The R-PBL model had the highest AUC for periodontitis (0.833) and severe periodontitis (0.796).
The Either model showed similar sensitivity to R-PBL, while SR and Both models underperformed.
Decision curve analysis confirmed the clinical utility of R-PBL and Either models.
Abstract
Background/Objectives: The objective of this study is to evaluate the diagnostic performance of a combined screening approach using self-reported periodontal information and radiographic periodontal bone loss (R-PBL) in identifying individuals with periodontitis. Methods: An exploratory cross-sectional study was conducted including adult participants with available panoramic radiographs and responses to a validated self-reported periodontal screening questionnaire. R-PBL was assessed on interproximal sites and classified according to established thresholds. Self-reported information followed a validated strategy based on the Center for Diseases Control tool. The performance of individual and combined indicators was analyzed against the 2018 case definition for periodontitis, calculating sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
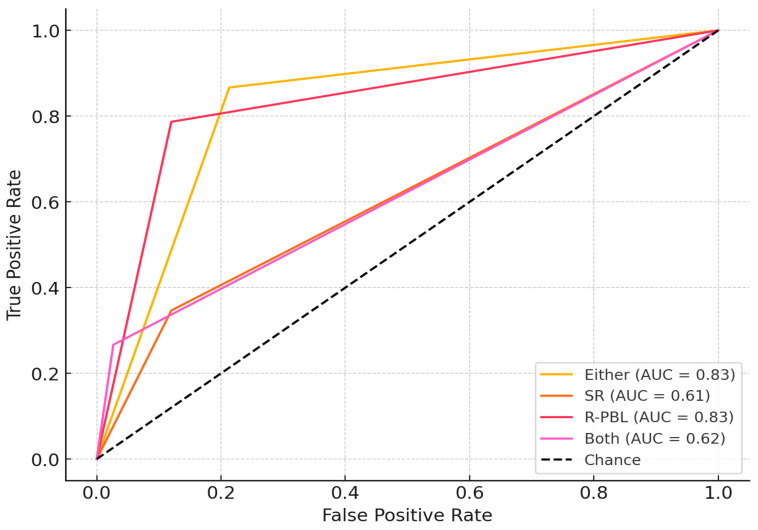 Figure 1
Figure 1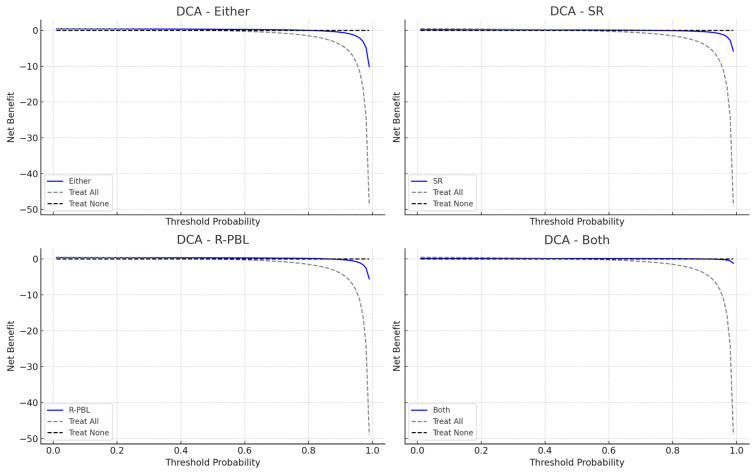 Figure 2
Figure 2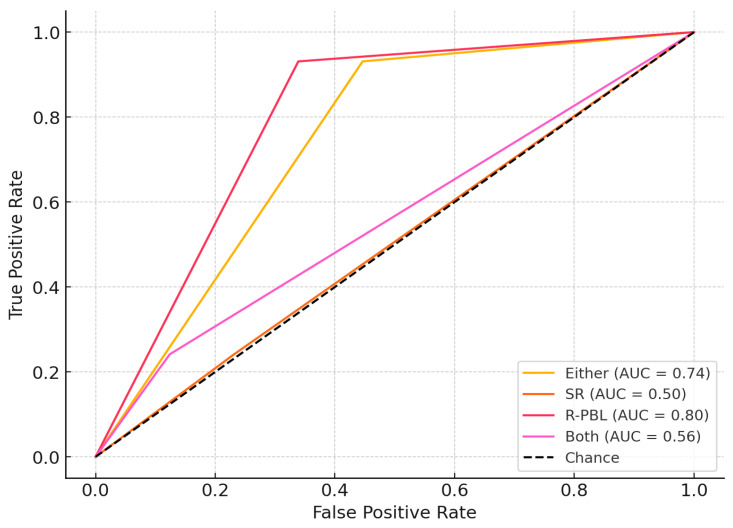 Figure 3
Figure 3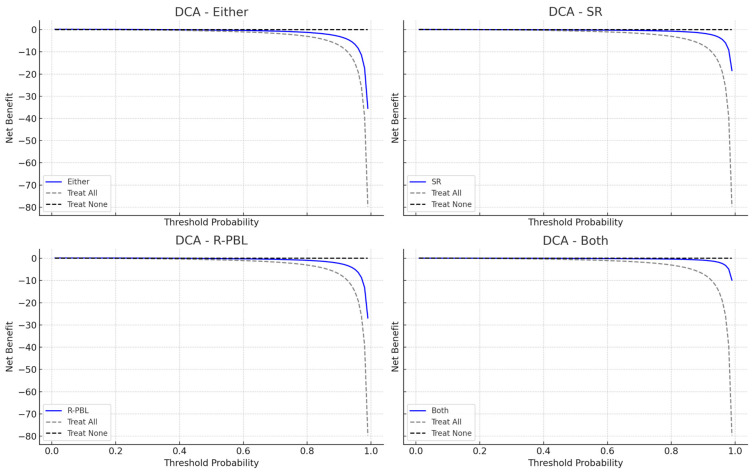 Figure 4
Figure 4- —national funds
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Dental Radiography and Imaging · Oral Health Pathology and Treatment
1. Introduction
Periodontitis represents one of the most prevalent chronic inflammatory conditions affecting adults globally [1,2,3]. It is estimated to affect nearly 62% of dentate people, with severe forms affecting nearly 25% of all cases [2]. This disease leads to tooth loss [4], has a detrimental economic effect [5,6], and has been increasingly linked to systemic conditions such as cardiovascular disease, diabetes, and adverse pregnancy outcomes [7]. Also, it affects more socio-economically deprived populations [3,8]. Thus, early screening and detection are crucial for timely intervention and enhanced patient outcomes [5,9,10].
Traditional diagnostic methods for periodontitis rely on clinical examination supplemented with radiographic assessment. Although effective, this diagnosis is time-consuming, operator-dependent, and not always accessible in community-based or resource-limited settings [11]. As a result, predictive models using simplified or digital tools have garnered attention for their potential to identify individuals at risk with greater efficiency and scalability [12,13]. In addition to clinical diagnosis, radiographic periodontal bone loss (R-PBL) (through periapical and/or panoramic X-rays) has been studied in the screening of periodontitis either by clinicians [14] or by machine learning [13,15].
In addition to radiographic screening, self-report tools have also emerged as valuable adjuncts in this triage, particularly in large-scale epidemiological studies and public health settings where clinical assessments may not be feasible [16]. These tools typically consist of structured questionnaires that capture an individual’s perception of their oral health status, symptoms (such as bleeding gums, tooth mobility, or halitosis), and behaviors related to oral hygiene and dental visits [17]. The appeal of self-report tools lies in their scalability, low cost, ease of administration, and capacity for remote or digital deployment [18], but at adequate levels of performance. This is then suited for population-level screening, triage in primary care, or integration into digital health platforms.
The integration of R-PBL with self-report tools may significantly enhance the effectiveness of periodontitis screening, particularly in large-scale or resource-limited settings. By leveraging the strengths of both, there is potential for improved risk stratification and targeted intervention. This study aimed to evaluate and compare the predictive performance and clinical utility of models combining R-PBL and self-reports in identifying individuals with periodontitis and severe periodontitis.
2. Materials and Methods
This performance study included a cross-sectional design and is reported following the TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis) statement [19], the checklist for which is available in the Supplementary Material to guarantee adherence to reporting standards. The Institutional Review Board granted approval for this study (Ethics Committee of Egas Moniz, IDs: 2024/1343 and 2025/1549), which adhered to the principles of the Declaration of Helsinki of 1975, as revised in 2024.
2.1. Source of Data and Participants
Data was collected at the Egas Moniz Dental Clinic (EMDC) (Portugal). The participants were incoming first-time patients attending a triage appointment; the study purpose was explained to them, and, then, they were invited to participate. Patient selection followed a consecutive sampling technique at the triage department. After obtaining informed consent, participants completed a questionnaire, and then underwent, in this order, panoramic X-ray (described in Section 2.3|Predictors) and a full-mouth periodontal examination (described in Section 2.2|Outcome).
Patients were included if they were 18 years old or older, able to respond to the questionnaires in Portuguese, and gave consent to participate in the study. Edentulous patients, pregnant or lactating women, or patients with the need of antibiotic prophylaxis before periodontal probing were excluded.
2.2. Outcome
Periodontal examination was performed by two trained and calibrated examiners (MN and CS). Intra-class correlation coefficients (ICC) were 0.86 and 0.79 for clinical attachment loss (CAL) and probing depth (PD), respectively. Intra-examiner ICC ranged from 0.90 to 0.85 for both PD and CAL, respectively.
Periodontal diagnosis was based on a full-mouth periodontal examination that included clinical parameters circumferentially using a CP-12 manual periodontal probe (Hu-Friedy^®^, Chicago, IL, USA). At six sites per tooth (mesiobuccal, buccal, distobuccal, mesiolingual, lingual, and distolingual), periodontal pocket depth (PPD), clinical attachment loss (CAL), and bleeding on probing (BOP) were recorded. The definition of these periodontal measures are as follows: PPD—distance from the free gingival margin to the bottom of the pocket; recession (REC)—distance from the cementoenamel junction (CEJ) to the free gingival margin; and a negative sign was assigned if the gingival margin was located coronally to the CEJ. Then, the CAL was calculated as the algebraic sum of the PPD and REC for each site. Measurements were rounded to the nearest whole millimeter. Tooth mobility was assessed according to Lindhe et al. [20], and furcation involvement using a Naber probe [21] and categorized accordingly.
After completing periodontal examination, data was uploaded to a database to categorize the periodontal status. Periodontitis cases were defined according to the American Academy of Periodontology/European Federation of Periodontology 2018 consensus, where a patient was a periodontitis case if interdental CAL was detected in ≥2 mm of non-adjacent teeth, or buccal or oral CAL ≥ 3 mm with pocketing > 3 mm was detected in ≥2 teeth [22]. Each case was then staged and graded accordingly. Severe periodontitis was then categorized as stage III or IV.
2.3. Predictors
A self-reported approach was implemented for periodontal status through a validated approach using thirteen questions, of which two had an area under the curve (AUC) of 0.8 of predictive ability [18,23].
Panoramic radiographs were obtained by a certified radiologist using the Viso G5 (Planmeca, Finland) according to the manufacturer’s instructions and stored at an internal cloud through an informatic software system database Romexis (Planmeca, Finland). For X-ray assessment calibration purposes, the same examiners (MN and CS) assessed 10 randomly selected panoramic radiographs and were in complete agreement in 10 of 10 observations (100%).
We then defined four possible screening routes:
- Confirmation from self-reported and R-PBL data (Both group);
- Confirmation through self-report (SR group);
- Confirmation with R-PBL (R-PBL group);
- Either self-reported or R-PBL confirmation (Either group).
2.4. Sample Size
To determine the necessary sample size for assessing our model’s diagnostic accuracy, we conducted a power analysis using the area under the receiver operating characteristic curve (AUC) as a basis. We assumed a null hypothesis AUC of 0.5, indicating no discriminative power, and aimed for a target AUC of 0.8, which suggests good performance. Our calculations identified the minimum number of participants required to achieve statistical significance with a two-sided alpha of 0.05 and a power of 90%. By applying the normal approximation method and converting the AUC to Cohen’s effect size, we found that at least 60 cases of periodontitis would be needed to detect the anticipated effect with the desired statistical power. This balanced design was intended to ensure a reliable evaluation of the model’s ability to discriminate.
2.5. Statistical Analysis
Data analyses were conducted using Microsoft Office Excel (Microsoft Corporation, USA), while modeling was performed in R (version 3.1). Four models were evaluated in relation to the organized groups and compared against clinical evaluations. Each model comprised each screening tour:
- Model Either (or model 1)—Code 1 if positive result for self-reported and R-PBL data; Code 0 if at least one or both of them negative.
- Model SR (or model 2)—Code 1 if positive result for self-reported; Code 0 if negative result for self-reported.
- Model R-PBL (or model 3)—Code 1 if positive result for R-PBL; Code 0 if negative result for R-PBL.
- Model Both (or model 4)—Code 1 if positive result for self-reported OR R-PBL data; Code 0 if both of them showed negative results.
Periodontitis cases were coded as 1, whereas healthy cases were coded as 0. Binary variables were coded as 0 = absence and 1 = presence for all relevant analyses. A subsequent analysis focused on severe periodontitis, with stage III and IV cases coded as 1, and all other cases coded as 0. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. The area under the curve (AUC) was then computed, accompanied by a 95% confidence interval (CI).
Decision curve analysis (DCA) was utilized to assess and compare the clinical utility of all four models [24]. DCA explicitly includes the clinical consequences of decision thresholds by quantifying the net benefit across a range of threshold probabilities [25,26].
Also, the expected/observed (E/O) ratio was computed. A significance level of p < 0.05 was used for all statistical tests.
Formal comparisons between the AUCs of different models were performed using DeLong’s test, as implemented in the ‘pROC’ package, and p-values for multiple comparisons were assessed using Bonferroni’s test.
3. Results
3.1. Participants
The inclusion of participants exceeded the sample calculation due to obtaining healthy patients before reaching the minimum number of periodontitis cases. A total of 75 cases and controls each were obtained. Overall, participants had an average age of 46.5 years old (±19.4), ranging between 18 and 83 years (Table 1). The study population had slightly more women (54.0% of females), and mostly consisted of never smokers (54.7%, n = 82) but with nearly a quarter of active smokers (27.3%, n = 41). Most participants reported having a medium education level (77.3%, n = 116). Following the planned 1:1 ratio, patients living with periodontitis were mostly affected with stage III (22.0%, n = 33) and stage IV (19.3%, n = 29). According to the distribution of grading and extent per staging (Table 2), this sample mostly comprised stage III–IV with a generalized extent and grade B and C.
3.2. Models Performance for Periodontitis
In the performance of the models for predicting periodontitis (Table 3), the model with ‘R-PBL’ alone showed the best discriminative ability for predicting periodontitis, with an AUC of 0.833 (95% CI: 0.771–0.892) (Figure 1). It achieved the highest precision (86.7%) among all models. The ‘Either model’ performed similarly, with an AUC of 0.827 (95% CI: 0.767–0.882), sensitivity of 86.7%, and specificity of 78.7%, with an E/O ratio of 1.08 indicating good alignment between predicted and observed cases. The SR and Both models demonstrated weaker performance, with AUCs of 0.613 (95% CI: 0.545–0.680) and 0.620 (95% CI: 0.565–0.675), respectively. DCA plots revealed the ‘R-PBL model’ had the highest net benefit across threshold probabilities, and the ‘Either model’ showed favorable net benefit at moderate thresholds, while SR and Both models offered limited benefits (Figure 2).
3.3. Models Performance for Severe Periodontitis
In the performance of the models for predicting severe periodontitis (Table 4), the ‘R-PBL model’ also showed the best discriminative ability for predicting periodontitis, with an AUC of 0.796 (95% CI: 0.724–0.853) (Figure 3). The accuracy, Youden’s index and precision values were lower than for periodontitis prediction models. The ‘Either model’ performed similarly, with an AUC of 0.742 (95% CI: 0.672–0.802), sensitivity of 86.7%, and specificity of 78.7%, with an E/O ratio of 1.08 indicating good alignment between predicted and observed cases. The SR and Both models demonstrated inadequate performance, with AUCs of 0.505 (95% CI: 0.420–0.599) and 0.559 (95% CI: 0.473–0.645), respectively. The clinical usefulness of the models revealed the R-PBL model to provide the highest net benefit across most threshold probabilities, highlighting its utility in guiding decisions around severe periodontitis detection. The Either model also showed favorable net benefit, while SR and Both offered limited clinical value (Figure 4).
DeLong’s test confirmed the results regarding the comparison of models’ AUC curves for periodontitis and severe periodontitis (Table 5).
4. Discussion
This study aimed to test the diagnostic performance and clinical utility of four predictive models towards periodontitis and severe periodontitis, using R-PBL and self-reported data alone or combined. In the models evaluated, R-PBL consistently showed superior discriminative performance in both scenarios, achieving AUC values deemed adequate (greater than 0.8). Its balanced sensitivity and specificity, along with the highest net benefit identified in DCA, emphasize its robustness and clinical relevance as a screening tool.
When self-reported measures were included in the predictive models, they did not demonstrate superior performance in their ability to capture subjective signs of disease. The “Either model”, which utilized self-reports with R-PBL, demonstrated high sensitivity and acceptable precision for periodontitis, performing on par with R-PBL across several metrics. These results support previous research indicating that well-designed self-report items can significantly enhance periodontal disease monitoring, especially in populations with limited access to clinical evaluations [17,18]. Although models based solely on simplified rules (SR) or conservative logic (both positive results to self-report and R-PBL) are user-friendly, they exhibited lower diagnostic accuracy and clinical benefit. These models demonstrated reduced sensitivity and Youden’s indices, indicating limited practical utility. Their net benefit was inferior to R-PBL and Either across most threshold probabilities, suggesting that their application may lead to missed cases or unnecessary interventions, contingent upon the clinical context.
The combination of R-PBL with self-reported data seems to present a promising path for scalable screening strategies at the population level, yet using solely R-PBL offers equal or superior performance and clinical utility. By integrating objective clinical guidelines with subjective symptoms and patient-reported behaviors, these hybrid models could enhance early detection and risk assessment. This is particularly significant when considering the global burden of periodontitis, with an estimated 54 billion USD/year in lost productivity and a major portion of the 442 billion USD/year cost for oral diseases [8].
This method aligns with the principles of precision in public health, utilizing accessible data sources to optimize prevention and resource distribution [27]. From a public health standpoint, employing models like R-PBL along with self-reporting could have a significant impact in community settings, primary care, or digital platforms [28]. Their straightforwardness, affordability, and strong performance make them excellent candidates for inclusion in national surveillance systems or targeted screening efforts in populations at risk. Additionally, incorporating DCA into the evaluation framework ensures that the models are assessed not only for statistical accuracy but also for their practical decision-making utility. Yet, our results do not exempt the requirement for clinical confirmation of the person’s periodontal status, as clinical examination is the gold standard. Nevertheless, such an approach could contribute to a more sustainable and accurate oral health primary care response in health systems, but the actual evidence remains limited to a specific clinical setting and requires cautious interpretation.
Strengths and Limitations
The main advantage of this study is its evaluation framework, which integrates conventional diagnostic performance metrics with decision curve analysis to determine its applicability in clinical settings. The study’s emphasis on the inclusion of self-reports meets the need for scalable screening solutions. However, it is important to acknowledge certain limitations. The models were tested within a specific demographic and context, and further validation in more diverse populations is required to ensure their applicability across different settings [29,30]. Additionally, as a binary model output, this may limit the precision of risk assessments [31]. Future studies shall be conducted to explore further significant risk indicators such as age, smoking habits, education level, living with diabetes, among others. And, while self-reports enhance the model value, they are susceptible to recall bias and subjective interpretation, which could affect the accuracy of predictions [30,32].
We acknowledge that the absence of internal validation (such as cross-validation or bootstrapping) and external validation represents a limitation of this study, which may affect the generalizability of our findings [29,30,31,33,34]. Future research will aim to address this through alternative validation techniques and testing model performance in independent cohorts.
5. Conclusions
R-PBL alone or combined with self-reports consistently demonstrated discrimination and clinical utility for predicting periodontitis, but for severe periodontitis, its sole use presents a better performance. Future studies should explore the integration and their performance in larger diverse populations to support personalized and preventive periodontal care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nascimento G.G. Alves-Costa S. Romandini M. Burden of Severe Periodontitis and Edentulism in 2021, with Projections up to 2050: The Global Burden of Disease 2021 Study J. Periodontal Res.20245982386710.1111/jre.1333739192495 · doi ↗ · pubmed ↗
- 2Trindade D. Carvalho R. Machado V. Chambrone L. Mendes J.J. Botelho J. Prevalence of Periodontitis in Dentate People between 2011 and 2020: A Systematic Review and Meta-Analysis of Epidemiological Studies J. Clin. Periodontol.20235060462610.1111/jcpe.1376936631982 · doi ↗ · pubmed ↗
- 3Bernabe E. Marcenes W. Abdulkader R.S. Abreu L.G. Afzal S. Alhalaiqa F.N. Al-Maweri S. Alsharif U. Anyasodor A.E. Arora A. Trends in the Global, Regional, and National Burden of Oral Conditions from 1990 to 2021: A Systematic Analysis for the Global Burden of Disease Study 2021 Lancet 202540589791010.1016/S 0140-6736(24)02811-340024264 · doi ↗ · pubmed ↗
- 4Slots J. Periodontitis: Facts, Fallacies and the Future Periodontol 200020177572310.1111/prd.1222128758294 · doi ↗ · pubmed ↗
- 5Botelho J. Machado V. Leira Y. Proença L. Chambrone L. Mendes J.J. Economic Burden of Periodontitis in the United States and Europe—An Updated Estimation J. Periodontol.20219337337910.1002/JPER.21-011134053082 · doi ↗ · pubmed ↗
- 6Jevdjevic M. Listl S. Global, Regional, and Country-Level Economic Impacts of Oral Conditions in 2019 J. Dent. Res.2025104172110.1177/0022034524128169839535193 PMC 11662506 · doi ↗ · pubmed ↗
- 7Botelho J. Mascarenhas P. Viana J. Proença L. Orlandi M. Leira Y. Chambrone L. Mendes J.J. Machado V. An Umbrella Review of the Evidence Linking Oral Health and Systemic Noncommunicable Diseases Nat. Commun.202213761410.1038/s 41467-022-35337-836494387 PMC 9734115 · doi ↗ · pubmed ↗
- 8Tonetti M.S. Jepsen S. Jin L. Otomo-Corgel J. Impact of the Global Burden of Periodontal Diseases on Health, Nutrition and Wellbeing of Mankind: A Call for Global Action J. Clin. Periodontol.20174445646210.1111/jcpe.1273228419559 · doi ↗ · pubmed ↗