Association of Percutaneous Endoscopic Gastrostomy (PEG) Tube Placement with Unplanned Hospitalization for Head and Neck Cancer
Sung Jun Ma, Jas Virk, Tyler V. Schrand, Jasmin Gill, Neil Almeida, Harshini K. Cheruvu, Vishal Gupta, Kimberly E. Wooten, Moni A. Kuriakose, Michael R. Markiewicz, Ryan P. McSpadden, Wesley L. Hicks, Mark K. Farrugia, Anurag K. Singh

TL;DR
This study finds that head and neck cancer patients with therapeutic PEG tubes are more likely to be hospitalized, which is linked to worse survival but not cancer outcomes.
Contribution
The study identifies unplanned hospitalization as an independent prognostic factor for survival, not cancer control, and links therapeutic PEG tube use to higher hospitalization risk.
Findings
Unplanned hospitalization is associated with worse overall and progression-free survival but not with cancer recurrence outcomes.
Therapeutic PEG tube placement increases the risk of unplanned hospitalization compared to prophylactic or no PEG use.
Patients who never needed PEG tubes had the lowest hospitalization rates.
Abstract
This study aims to answer the following question: are there differences in the outcomes among head and neck cancer patients with prophylactic versus therapeutic percutaneous endoscopic gastrostomy (PEG) tubes? We found that unplanned hospitalizations were associated with poor survival, but not oncologic outcomes. Compared to patients with a prophylactic PEG tube, those without a PEG tube were less likely to be hospitalized, while others with a therapeutic PEG tube were more likely to be hospitalized. These results indicate that unplanned hospitalization is an independent, adverse prognostic factor for poor survival. The hospitalization incidence was the lowest among those who never needed PEG tubes, while those with therapeutic PEG tubes were most likely to be hospitalized. Background/Objectives: There is a varying need for nutritional support among head and neck cancer (HNC) patients.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
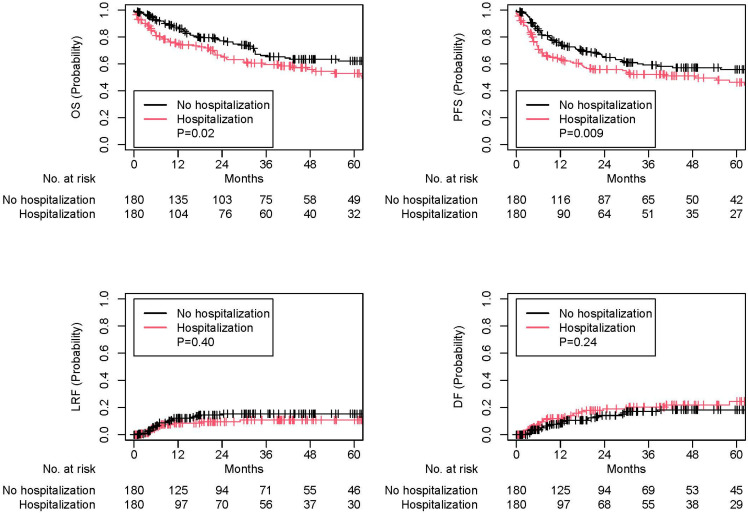 Figure 1
Figure 1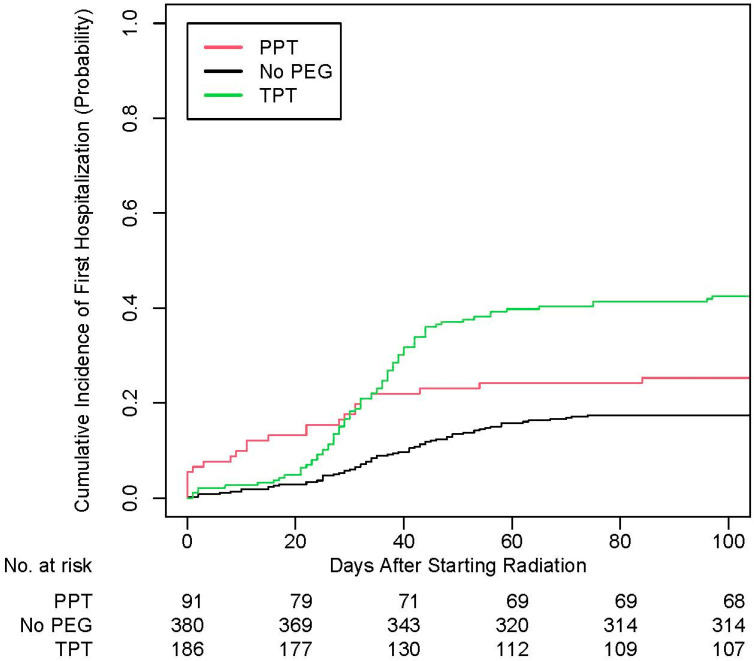 Figure 2
Figure 2- —National Cancer Institute Cancer Center Support Grant
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDysphagia Assessment and Management · Clinical Nutrition and Gastroenterology · Esophageal and GI Pathology
1. Introduction
Even in the modern era of intensity-modulated radiation therapy (IMRT) routinely utilized for patients with head and neck cancer (HNC), nearly two thirds of these patients experience severe oral mucositis associated with unplanned hospitalization, weight loss, and frequent opioid use [1]. As a result, many studies suggest that having prophylactic percutaneous endoscopic gastrostomy (PEG) tubes may reduce risks of malnutrition and hospitalization, while minimizing treatment interruptions [2,3,4,5,6]. This contrasts with less than 10% of patients having a prophylactic PEG tube in a recent national cooperative group clinical trial [7]. The current cooperative-group phase III protocol (ClinicalTrials.gov ID: NCT05050162) and the Multinational Association of Supportive Care in Cancer (MASCC) guideline [8] did not specify algorithms for the use of prophylactic PEG tubes. The National Comprehensive Cancer Network (NCCN) guideline recommends an individualized approach for the use of prophylactic PEG tubes based on each patient’s functional and nutritional status at the treating physician’s discretion [9].
In addition to the differences in practice patterns regarding the use of prophylactic PEG tubes, many studies did not compare those with a therapeutic PEG tube versus others who did not need a PEG tube at all [2,3,4,5,6]. As a result, it remains unclear whether increased hospitalization rates were largely driven by a subset of patients without a PEG tube at baseline and how these rates were different from patients with a prophylactic PEG tube. Furthermore, the association between unplanned hospitalization and oncologic outcomes was not previously reported. To address this knowledge gap, we performed an observational cohort study to evaluate the association of unplanned hospitalization with clinical outcomes and PEG tube use.
2. Materials and Methods
Our study was reviewed and approved by the Institutional Review Board at the Roswell Park Comprehensive Cancer Center (EDR 103707), following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Our single-institution database was queried for those diagnosed with non-metastatic HNC treated with definitive chemoradiation between June 2007 and April 2023. Everyone in our cohort underwent intensity-modulated radiation therapy with a total range of 69.96–70 Gy in 33–35 fractions [10]. Patients with metastatic cancer or treated with surgery, radiation alone, or palliative treatments were excluded.
Variables of interest included age, gender, race, smoking, primary cancer site, body mass index (BMI), cancer staging based on the American Joint Committee on Cancer (AJCC) 7th edition, p16 status, performance status, concurrent chemotherapy regimens, and PEG tube placement. Prophylactic PEG tube placement was defined as PEG tube placement prior to starting radiation, regardless of the patients’ baseline swallowing functions and nutritional status. Therapeutic PEG tube placement was defined as the PEG tube placement after starting radiation in the setting of a multidisciplinary evaluation based on patients’ swallowing function, nutritional status, significant weight loss, and severe mucositis pain among other factors. All variables were included for multivariable analysis (MVA) models, since they were considered clinically relevant. Missing values were coded as unknown prior to analysis.
Our primary endpoints were survival outcomes: overall survival (OS) and progression-free survival (PFS), defined as time intervals from diagnosis to death from any cause and to death from any cause or tumor progression, respectively. Other endpoints were locoregional failure (LRF) and distant failure (DF), defined as time intervals from diagnosis to tumor recurrence within and outside the head and neck, respectively. Another endpoint of interest was time to first unplanned hospitalization, defined as the time interval from the start of radiation to the date of unplanned admission.
Statistical Analysis
Baseline variables were evaluated and compared based on the Fisher exact test and the Mann–Whitney U test for categorical and continuous characteristics, respectively. Reasons for unplanned hospitalization were summarized using descriptive statistics. OS and PFS were analyzed using the Kaplan–Meier plots, log-rank tests, and Cox proportional hazards MVA. LRF and DF were analyzed using the Fine–Gray MVA with death as a competing event and cumulative incidence plots. To reduce selection bias and evaluate the robustness of our MVA findings, propensity score matching was also performed comparing those with or without unplanned hospitalization. All variables were included for matching using the nearest neighbor method, 1:1 ratio without replacement, and a caliper distance of 0.2 [11]. Exploratory subgroup analysis was performed to analyze OS, PFS, LRF, and DF by repeating Cox and Fine–Gray MVA stratified by p16 status. Logistic MVA was performed to evaluate variables associated with first and multiple unplanned hospitalizations. Time to first hospitalization was analyzed using Fine–Gray MVA and cumulative incidence plots comparing those with or without a PEG tube placement. Given the multiple comparisons (therapeutic PEG tube vs. prophylactic PEG tube; no PEG tube vs. prophylactic PEG tube), Holm–Bonferroni method was performed in this setting. In addition, logistic MVA was also performed to identify the variables associated with therapeutic PEG tube placement among those without a PEG tube at baseline.
All p values were two-sided and those equal to or less than 0.05 were considered statistically significant. All analyses were performed using R version 4.3.2 (R Group for Statistical Computing).
3. Results
A total of 657 patients were identified and met our criteria (Table 1). Most patients were Caucasian (n = 568, 86.5%), male patients (n = 535, 81.4%) with a median age of 61.2 years (interquartile range: 54.9–67.0), former smoking history (n = 374, 56.9%), and oropharyngeal cancer (n = 375, 57.1%), who underwent definitive chemoradiation with cisplatin (n = 550, 83.7%). Median follow up was 30.3 months (interquartile range: 10.0–60.8).
Of 657 patients, 188 patients (28.6%) were hospitalized at least once and 52 patients (7.9%) were hospitalized more than once. Median duration of hospitalization was 5 days (interquartile range: 3–9). The three most common reasons for such unplanned hospitalizations were dehydration, fever, and dysphagia/odynophagia (Table 2). Those with unplanned hospitalization had a worse OS (adjusted hazards ratio [aHR] of 2.07, 95% confidence interval [CI] of 1.53–2.81, p < 0.001) and PFS (aHR 1.83, 95% CI 1.38–2.41, p < 0.001), but not LRF (aHR 0.78, 95% CI 0.43–1.42, p = 0.41) or DF (aHR 1.42, 95% CI 0.84–2.42, p = 0.19; Table S1). Similar findings were noted on 180 matched pairs (OS: HR 1.51, 95% CI 1.08–2.12, p = 0.02; PFS: HR 1.52, 95% CI 1.11–2.09, p = 0.009; LRF: HR 0.75, 95% CI 0.39–1.46, p = 0.40; DF: HR 1.38, 95% CI 0.80–2.37, p = 0.24; Figure 1 and Table 1) as well as subgroup cohorts for 263 patients with p16-negative tumors and 340 patients with p16-positive tumors (Table 3).
On logistic MVA for the entire cohort, male patients (adjusted odds ratio [aOR] of 0.46, 95% CI 0.29–0.72, p < 0.001) and those without a PEG tube (aOR 0.48, 95% CI 0.27–0.86, p = 0.01) were less likely to be hospitalized, while others with a therapeutic PEG tube (aOR 1.96, 95% CI 1.10–3.54, p = 0.02) were more likely to be hospitalized (Table 4). Similar findings were noted when evaluated for time to first unplanned hospitalization (Table 5 and Figure 2). In addition, those who were overweight were also less likely to be hospitalized multiple times (aOR 0.36, 95% CI 0.15–0.82, p = 0.02; Table 4). Among 566 patients without a prophylactic PEG tube, 186 patients (32.9%) received a therapeutic PEG tube. On logistic MVA among these patients, those with p16-positive tumors were less likely to receive therapeutic PEG tube placements (aOR 0.51, 95% CI 0.28–0.92, p = 0.03; Table 6).
4. Discussion
To our knowledge, this is the largest single-institution study suggesting that unplanned hospitalization is an independent, adverse prognostic factor for survival, but not cancer control outcomes, regardless of p16 status. Among those without a prophylactic PEG tube, more than two thirds of these patients did not require a therapeutic PEG tube and had the lowest incidence of unplanned hospitalization. Unplanned hospitalization was largely driven by those who required a therapeutic PEG tube.
The association between unplanned hospitalization and poor survival outcomes in our study was consistent with our prior report [12]. Such a finding was noted regardless of p16 status in our study, and it may be in part due to the poor overall clinical and nutritional status as indicated by the frequent need for therapeutic PEG tubes. However, unplanned hospitalization was not associated with poor oncologic outcomes in our study. In our comprehensive cancer center, daily radiation can be often continued on inpatients, and less than 1% of patients experienced radiation treatment interruptions in our prior study [13]. In addition, less than 10% of patients had multiple hospitalizations in our study, so a limited number of patients were at risk for missing multiple cycles of chemotherapy.
In our study, among those without a prophylactic PEG tube, approximately a third of patients required therapeutic PEG tube placement. This placement rate was consistent with other institutional studies reporting 20–40% of patients requiring therapeutic PEG tubes [3,14,15,16], though it was far less than over 60% reported in a recent national cooperative group trial [7]. This discrepancy may suggest significant heterogeneity in practice patterns for utilizing PEG tubes.
After stratifying patients without prophylactic PEG tubes into those who did or did not require therapeutic PEG tubes, unplanned hospitalization was mainly driven by those with a therapeutic PEG tube. However, other studies did not stratify those without a prophylactic PEG tube [2,4,5,6]. As a result, multiple studies reported no statistically significant differences in unplanned hospitalization due to the presence or absence of a prophylactic PEG tube [3,5,17]
A prophylactic PEG tube may be insufficient for preventing unplanned hospitalizations. For instance, other methods of nutritional supplementation could similarly address weight loss, [18] and frequent intravenous hydration may also help with pain control [19] There was also a high rate of non-use (47%) or limited use (less than two weeks) among those with a prophylactic PEG tube [20]. In addition, a prior review suggested that up to 40% of patients with a PEG tube may experience a varying severity of complications, such as PEG tube site infection, leakage of gastric contents, PEG tube dislodgement and blockage, and diarrhea from dietary changes [21,22].
Nonetheless, dehydration was the most common reason for hospitalization; therefore, unplanned hospitalizations could have been potentially reduced if those with therapeutic PEG tubes received prophylactic PEG tubes instead. Predicting which patients are at greatest risk of therapeutic PEG tube placement and unplanned hospitalizations may help. For example, a machine learning-based algorithm was previously shown to identify high-risk patients for hospitalization, [23] and an ongoing INSIGHT trial is currently investigating the role of close symptom surveillance for reducing hospitalizations among patients receiving definitive chemoradiation (ClinicalTrials.gov ID: NCT05338905). Volume de-escalation in radiation treatments has also been shown to numerically reduce the incidence of therapeutic PEG tubes within 3 months after treatment in a phase III clinical trial [24]. In addition, a secondary analysis of three prospective trials demonstrated that wearable devices allowed the continuous collection of daily step counts, and a machine learning-based model based on step counts predicted hospitalization during chemoradiation with accuracy, specificity, and sensitivity scores of 82.1%, 83.0%, and 60.7%, respectively [25]. A pilot trial incorporating wearable devices also showed that a week-to-week reduction in daily steps was associated with a substantial decline in quality of life [26].
In our study, p16-negative status was the only variable associated with therapeutic PEG tube placement among those without PEG tubes at baseline. Our finding is consistent with another study suggesting a greater disease burden and a higher likelihood of therapeutic PEG tube placement among those with p16-negative tumors [27]. However, our finding is inconsistent with another report showing that those with p16-positive tumors were associated with significant weight loss and therapeutic PEG tube placement as a result [16]. This discrepancy may be due to the higher nodal disease burden and combined modality treatments seen among those with p16-positive tumors [16].
Our study also showed that patients with overweight BMI were less likely to receive multiple hospitalizations. Such findings are consistent with another study reporting higher baseline BMI being associated with reduced complications, hospitalizations, and adequate nutritional status [28]. As a result, such patients may be able to have more cycles of chemotherapy, leading to improved survival outcomes [29,30]. Regardless of PEG tube use, overweight BMI has been similarly shown to be a favorable prognostic factor in patients with HNC undergoing definitive chemoradiation [13,31].
The limitations include the retrospective nature of our study. In addition, other clinically relevant variables, such as baseline functional and nutritional status, medical comorbidities, weight changes, adherence to treatments, toxicity profiles and their etiologies, dietary intake, the actual usage of a PEG tube by patients, exact duration of PEG tube placement, and complications from PEG tube placement, were unavailable for analysis. Our findings may not be generalizable to those who received surgery or had limited access to supportive care services during treatment. In addition, though a multidisciplinary discussion and shared decision-making occurred regarding nasogastric tube placement prior to finalizing therapeutic PEG tube placement, the nasogastric tube placement outcome was not collected for analysis in our database. Furthermore, radiation dosimetric data, such as radiation doses to pharyngeal constrictor muscles, were not available for all patients for analysis.
5. Conclusions
Our study showed that unplanned hospitalization is an independent, adverse prognostic factor for survival, but not cancer control outcomes, regardless of p16 status. Among those without a PEG tube at baseline, more than two thirds did not need a therapeutic PEG tube. Patients without PEG had the lowest incidence of unplanned hospitalization. Unplanned hospitalization was mainly driven by those who required a therapeutic PEG tube.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iovoli A.J. Turecki L. Qiu M.L. Khan M. Smith K. Yu H. Singh A.K. Severe Oral Mucositis After Intensity-Modulated Radiation Therapy for Head and Neck Cancer JAMA Netw. Open 20236 e 233726510.1001/jamanetworkopen.2023.3726537819659 PMC 10568356 · doi ↗ · pubmed ↗
- 2Almeida N.D. Yu H. Iovoli A.J. Fang M. Schrand T.V. Pepin A. Singh A.K. Prophylactic gastrostomy tube during chemoradiation for head and neck cancer decreases weight loss but increases rate of tube use beyond six months Oral Oncol.202516010713610.1016/j.oraloncology.2024.10713639671770 · doi ↗ · pubmed ↗
- 3Lee J.H. Machtay M. Unger L.D. Weinstein G.S. Weber R.S. Chalian A.A. Rosenthal D.I. Prophylactic gastrostomy tubes in patients undergoing intensive irradiation for cancer of the head and neck Arch. Otolaryngol. Head Neck Surg.199812487187510.1001/archotol.124.8.8719708712 · doi ↗ · pubmed ↗
- 4Nguyen N.P. North D. Smith H.J. Dutta S. Alfieri A. Karlsson U. Sallah S. Safety and effectiveness of prophylactic gastrostomy tubes for head and neck cancer patients undergoing chemoradiation Surg. Oncol.20061519920310.1016/j.suronc.2006.12.00217280829 · doi ↗ · pubmed ↗
- 5Piquet M.A. Ozsahin M. Larpin I. Zouhair A. Coti P. Monney M. Roulet M. Early nutritional intervention in oropharyngeal cancer patients undergoing radiotherapy Support. Care Cancer 20021050250410.1007/s 00520-002-0364-112353130 · doi ↗ · pubmed ↗
- 6Wiggenraad R.G.J. Flierman L. Goossens A. Brand R. Verschuur H.P. Croll G.A. Vriesendorp R. Prophylactic gastrostomy placement and early tube feeding may limit loss of weight during chemoradiotherapy for advanced head and neck cancer, a preliminary study Clin. Otolaryngol.20073238439010.1111/j.1749-4486.2007.01533.x 17883560 · doi ↗ · pubmed ↗
- 7Gillison M.L. Trotti A.M. Harris J. Eisbruch A. Harari P.M. Adelstein D.J. Le Q.T. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial Lancet 2019393405010.1016/S 0140-6736(18)32779-X 30449625 PMC 6541928 · doi ↗ · pubmed ↗
- 8Alderman B. Allan L. Amano K. Bouleuc C. Davis M. Lister-Flynn S. Mukhopadhyay S. Davies A. Multinational Association of Supportive Care in Cancer (MASCC) expert opinion/guidance on the use of clinically assisted nutrition in patients with advanced cancer Support. Care Cancer 2022302983299210.1007/s 00520-021-06613-y 34665311 PMC 8857106 · doi ↗ · pubmed ↗