Exercise Specialists’ Evaluation of Robot-Led Rehabilitative Exercise for People with Parkinson’s Disease
Matthew Lamsey, Meredith D. Wells, Lydia Hamby, Paige E. Scanlon, Rouida Siddiqui, You Liang Tan, Jerry Feldman, Charles C. Kemp, Madeleine E. Hackney

TL;DR
Exercise specialists positively evaluated a robot-led exercise system for Parkinson's patients, noting its potential to improve engagement and consistency, but suggesting improvements in feedback and usability.
Contribution
A pilot study evaluating exercise specialists' perceptions of a robot-led rehabilitative exercise system for Parkinson’s disease, highlighting acceptance and areas for improvement.
Findings
Exercise specialists generally viewed the robot-led system as effective for augmenting traditional rehabilitative exercise.
The system was seen as beneficial for enhancing patient engagement and providing consistent exercise support.
Key areas for improvement included more human-like feedback and increased ease of use.
Abstract
Background/Objectives: Robot-led rehabilitative exercise offers a promising avenue to enhance the care provided by exercise specialists (ESs). ESs, such as physical and occupational therapists, prescribe exercise regimens to clinical populations to improve patients’ adherence to prescribed exercises outside the clinic, such as at home. Collaborative efforts among roboticists, clinical ESs, and patients are essential for developing interactive, personalized exercise systems that meet each stakeholder’s needs. This work builds upon research involving individuals with Parkinson’s disease (PD) that evaluated a robotic rehabilitative exercise system designed to address strength and flexibility deficits. Methods: To complement the findings of our previous work in people with PD (PWP), we conducted a pilot user study in which 11 ESs evaluated a novel robot-led exercise system for PWP, focusing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
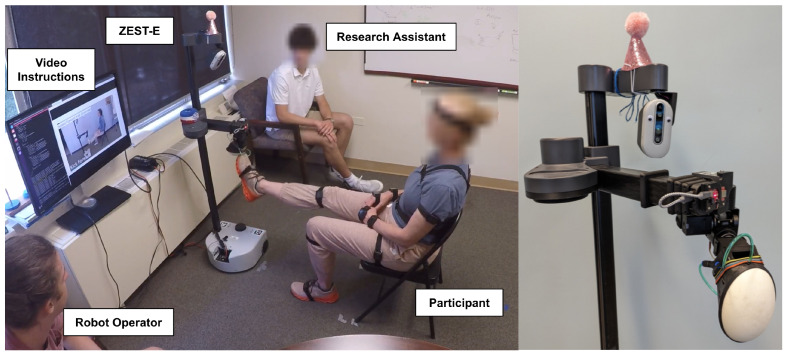 Figure 1
Figure 1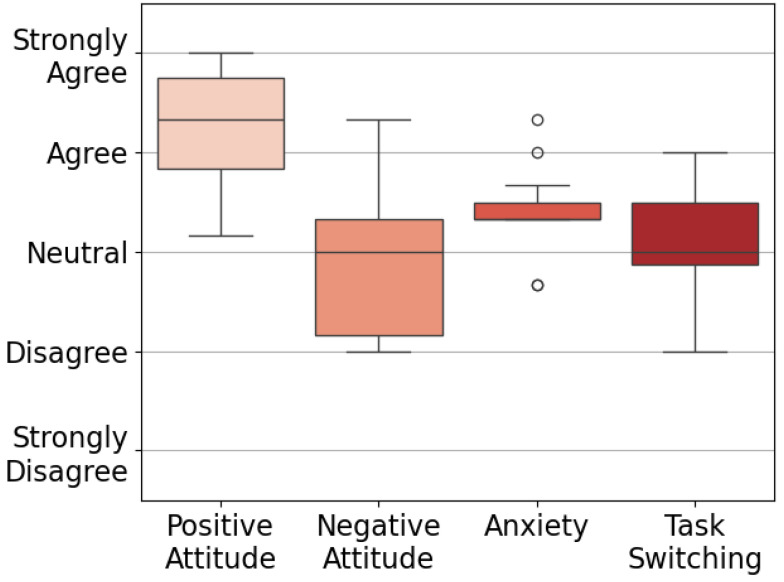 Figure 2
Figure 2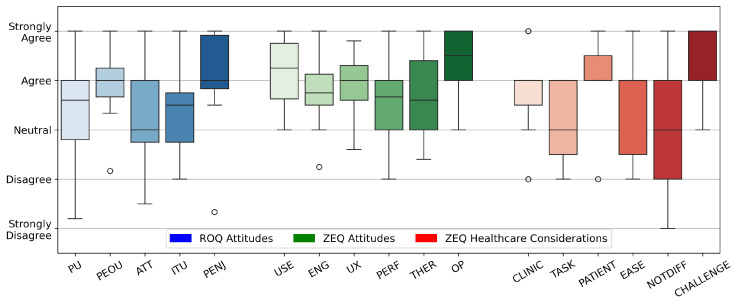 Figure 3
Figure 3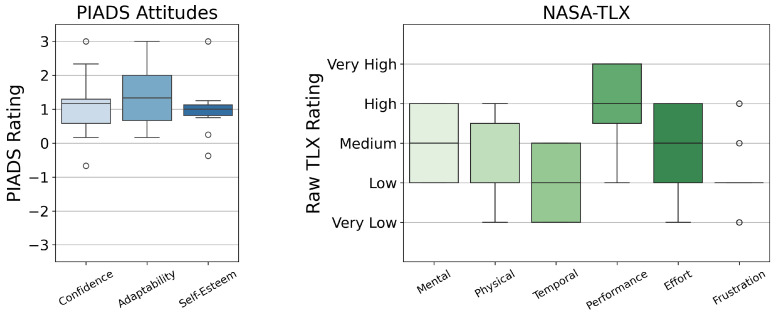 Figure 4
Figure 4- —Toyota Research Institute
- —McCamish Parkinson’s Disease Innovation Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Muscle activation and electromyography studies · Cerebral Palsy and Movement Disorders
1. Introduction
Due in part to a globally aging population [1], Parkinson’s disease (PD) is now among the fastest-growing neurodegenerative disorders in the United States [2]. As of 2020, over one million Americans are living with PD [3]. People with PD (PWP) often experience motor impairments such as bradykinesia, hypometria, and postural instability [4,5,6] as well as cognitive impairments and difficulty with dual-tasking [7,8,9] (i.e., conducting simultaneous cognitive and motor tasks). Physical and occupational therapists often treat these symptoms with progressive and tailored physical and cognitive exercises [10,11,12], which have been shown to mitigate symptom progression and improve individuals’ quality of life [13,14,15,16]. However, there are factors, including PWP’s difficulties with intrinsic motivation [17] and a general shortage of healthcare providers [18], that remain obstacles for achieving maximal benefits from correct exercise dosing [19].
Many types of exercise have been evaluated as treatments for PD. A review by Mak et al. discusses several types of exercise used as PD treatments, including gait training, walking exercise, balance exercise, tai-chi, dance, and “exergaming” [20]. These exercises target specific PD symptoms, including hypometria, freezing of gait, coordination, balance, and muscle strength. Research highlights the importance of personalized exercise interventions and innovative approaches to effectively deliver and optimize rehabilitative exercise for PD [21]. Some symptoms require more specific interventions, e.g., diverse exercise interventions spanning dance, aquatic, and cueing training have been shown to improve freezing of gait in PWP [22]. Gait training has been established as an effective method to reduce fall risk in PWP [23]. PWP’s performance of activities of daily living (ADLs) also showed the greatest improvement when training was specifically targeted at ADLs [24]. Yet, the required exercise dose for effective results often surpasses what a therapist can provide [19]. PWP engaging in physical therapy or rehabilitative exercise often are required to engage in the prescribed exercise several days a week when not in the presence of a physical therapist [25]. PWP typically see a physical therapist or other ESs on average one time per week, for e.g., 12 weeks, depending on the prescription by the provider [25]. Beyond challenges with intrinsic motivation, many barriers exist to PWP’s adherence to exercise prescriptions outside of the clinic, such as social stigma surrounding exercises performed in public [26], perceived lack of social and professional support [27], and low self-efficacy [27]. These facts suggest that supplementing human-supervised exercise with technology-based interventions may enhance motivation and adherence.
A wide array of technology-based supplements to human-led exercise therapy has emerged to address these challenges. For example, Augmented Reality (AR) and Virtual Reality (VR) have been used to supplement therapeutic exercise for PD. While head-mounted AR devices may improve exercise adherence [28], other work found that AR has limited utility in treating freezing of gait, and at times can worsen these symptoms [29]. Head-mounted VR systems [30,31] have been used in limited capacities for gait and balance training for PWP and may result in short-term improvements in motor performance [32]. Yet, VR and AR may induce discomfort and nausea in users [33,34], emphasizing the need for alternative interactive platforms.
Robotic exercise aids offer a promising solution to enhance therapeutic exercises facilitated by physical and occupational therapists. A 2024 review of robotics in physical rehabilitation [35] highlights the promise of robotic technologies such as exoskeletons, assistive training devices, and brain-computer interfaces for rehabilitation. Yet, this review cites consistent areas for improvement related to robots’ ease of use and high system cost. Physically interactive robotic therapy systems have been tested in interventions for specific impairments, such as post-stroke rehabilitation of gross motor skills [36,37] and fine motor skills [38,39], walking rehabilitation [40,41], and motor–cognitive rehabilitation [42]. These systems combine physical and visual feedback to guide therapeutic exercises, which has proven to be beneficial in alleviating users’ symptoms. However, they frequently incorporate purpose-built hardware that is too large, expensive, or complex for use outside of a clinical environment. Wearable rehabilitation robots, such as neck rehabilitation robots [43] and hand exoskeletons [44], are more portable, yet remain expensive and purpose-built for a single task.
Socially Assistive Robots (SARs) have also been studied as an often lower cost and more accessible form of robotic therapy, including seated exercise [45] and tabletop rehabilitation games [46]. Social–physical human–robot interaction (HRI) aims to combine the benefits of socially and physically interactive systems through exercises such as hand-clapping exercise games [47] and emotional support via hugging [48]. While socially and physically interactive systems are rated as highly engaging, they may present safety concerns due to the robots’ large sizes and heavy masses.
Understanding how individuals experience a new technology is crucial for developing effective solutions. Tools like Technology Acceptance Models (TAMs) [49,50] capture users’ attitudes, including Perceived Usefulness and ease of use. The NASA Task Load Index (TLX) [51,52] assesses mental and physical demands associated with a task, which can be applied to assistive technologies. Similarly, the Perceived Impact of Assistive Devices Scale (PIADS) [53] measures how an assistive device influences competence, adaptability, and self-esteem. Recent mixed-methods studies involving clinicians considering the administration of robotic therapy highlight critical factors for rehabilitation robots, such as telepresence, ease of use, reliability, and cost [54], and also report generally positive perceptions of these robots’ usefulness and ease of use in stroke rehabilitation [55].
Previous work [56] presented a personalized, socially and physically interactive robotic rehabilitative exercise system for PWP, originally named “Stretch with Stretch” (SWS) and now referred to as ZEST-E (Zesty Exercise System for Therapeutic Engagement). This study, involving 10 PWP, found that ZEST-E was engaging, and PWP perceived robot-led exercises to be moderately difficult, which aligns with recommendations for exercise-based interventions for PD [11]. At a Technology Readiness Level (TRL) [57] of 4, indicating successful demonstration in controlled laboratory settings, ZEST-E represents an early-stage prototype in the nascent domain of PD-specific rehabilitative exercise technology; our ongoing work focuses on maturing the system toward real-world clinical and home use.
The goal of this study was to build on this prior work by evaluating ZEST-E through a mixed-methods study with exercise specialists (ESs), which we defined as individuals who have professionally administered exercises to PWP. This definition includes physical and occupational therapists, exercise physiologists, and exercise instructors. ESs evaluated the system both from the perspective of a potential user and through the lens of potentially prescribing ZEST-E as a treatment for their patients. While ESs aren’t ZEST-E’s primary users, their role as secondary users who would be responsible for administering the technology offers key insights into real-world implementation. We aimed to explore the attitudes, perceptions, and beliefs of ESs regarding the usability of ZEST-E, and we expected to identify key factors that facilitate or hinder the adoption and improvement of systems like ZEST-E. Paired with our previous findings from PWP (the primary users), this clinician-focused evaluation highlights the need to balance patient-centered design requirements with clinicians’ workflow and clinical considerations to maximize both usability and clinical effectiveness. A preprint of this work is available in [58].
2. Materials and Methods
2.1. Robotic Exercise System
The design of ZEST-E was first described in [56], in which 10 PWP evaluated the system. ZEST-E consists of a mobile manipulator [59] equipped with a soft bubble end effector [60] that serves as an exercise target, or external cue, for users to reach towards and press on with different parts of their body during robot-led exercise games, as shown in Figure 1. ZEST-E is capable of leading ten stretching exercises involving different body parts and motions, directly targeting hypometria and bradykinesia typically associated with PD. ZEST-E personalizes the location of the exercise targets using three sources of information: (1) human kinematic models for each exercise based on an individual’s body dimensions, estimated with a human pose estimator [61]; (2) haptic samples of an individual’s range of motion along each exercise trajectory; and (3) dynamic adjustments based on an individual’s real-time performance. ZEST-E provides verbal and video instructions for completing each exercise and also includes audio cues in reaction to events, such as chiming each time a user scores a point by touching the robot’s end effector. A simultaneous cognitive challenge, such as naming a unique animal after each repetition, can also be included with each stretching exercise to address deficits in dual-tasking. Notably, ZEST-E requires no donning or doffing of peripheral equipment.
2.2. User Study
Eleven ESs, all of whom worked with PWP, participated in an exploratory trial to collect data regarding healthcare providers’ perceptions of ZEST-E. We purposively recruited ESs who had experience working with PWP in a variety of capacities, including physical therapy ( ) and strength training ( ). This study was approved by the Institutional Review Boards at the Georgia Institute of Technology (protocol H22359) and the Emory University School of Medicine (protocol STUDY00004909). All participants provided written informed consent prior to participation.
Each ES participated in one session lasting for approximately 2.5 h, following the same protocol as participants with PD [56]. The experimental setup for this study is shown in Figure 1. ZEST-E led each participant through an exercise session that lasted approximately one hour and consisted of four sets of six stretching exercises, totaling 24 sets. The six exercises were seated forward reaches, seated forward kicks, seated calf raises, standing reaches across the body, standing reaches down, and standing high knees. Two of the exercises involved a simultaneous cognitive task. For each exercise, ZEST-E first provided verbal and video instructions for completing the exercise. Then, ZEST-E guided users through a calibration of their right and left side ranges of motion in order to gather data regarding where to initially place the target for each exercise. Lastly, participants performed two 30 s sets of repetitions of the exercise with the right and left side for a total of four sets. ZEST-E automatically adjusted the difficulty of the exercise by moving the location of the target between each set based on the user’s performance. Each robot-led exercise set was manually initiated by a researcher. After the exercise session, we administered several surveys, and at the conclusion of the session, each participant was led through a semi-structured exit interview about their experience with ZEST-E.
2.3. Surveys
After the exercise session, we administered surveys (Table 1), including the Technology Attitudes Questionnaire [62], NASA TLX [51,52], the Psychosocial Impact of Assistive Devices Scale (PIADS) [53], and the Robot Opinions Questionnaire (ROQ) [63]. Responses to the Technology Attitudes Questionnaire were aggregated into four themes rated on a Likert-type scale from 1–5, where 1 indicates strong disagreement attitude towards technology and 5 indicates strong agreement with that attitude. For the NASA TLX, we computed the “Raw TLX” scores for each of the six task load metrics [52]. For PIADS, we aggregated the responses into three categories rated on a scale of −3 to +3, where −3 corresponds to “strongly decreases” and +3 corresponds to “strongly increases”. Each of the attitudes in the ROQ was rated on a Likert-type scale from 1–5, where 1 indicates strong disagreement or negative feelings towards an attitude, and 5 indicates strong agreement or positive feelings towards that attitude. Each questionnaire was scored according to the methodology in its corresponding original publication.
We also administered a custom survey, the ZEST-E Evaluative Questionnaire (ZEQ), to evaluate specific attributes of our system. This survey queries users’ engagement and motivation while using ZEST-E and adapts technology acceptance concepts, such as usability and usefulness, to an exercise-specific context. The ZEQ consists of questions from the perspective of both a user of the system as well as questions from that of a clinician who would administer robot-led therapy as part of treatment (Table 2). We categorized questions into six distinct themes to capture comprehensive insights into the participants’ experiences with the robot. Themes such as “Usability and Interaction”, “Engagement and Motivation”, and “User Experience” primarily focus on users’ perceptions and interactions with the system. Meanwhile, “Performance and Accuracy”, along with “Therapeutic Efficacy and Relevance”, assess the robot’s effectiveness in leading therapeutic exercises. “Healthcare Provider Considerations” directly assesses how the ESs perceive the value of the system in their practice. Each item in the ZEQ was rated on a Likert-type scale from 1–5, where 1 indicates strong disagreement or negative feelings towards an attitude, and 5 indicates strong agreement or positive feelings towards that attitude. For each theme in the generic (patient perspective) portion of the ZEQ, we computed Cronbach’s to determine the internal consistency. Highly consistent values (>0.61 [64]) allow us to compute an average response across individual items for each theme for each participant [63].
2.4. Exit Interviews
In addition to questionnaires, we conducted a semi-structured exit interview with each participant. Questions from the interview are provided in Table 3. The interview was conducted immediately following completion of the surveys. The intent of the interview questions was to identify ES’ perceptions of facilitators and barriers to the adoption of systems like ZEST-E.
Interviews were coded using NVivo 12 software. First, two independent raters performed inductive open coding to identify overarching themes. A third independent researcher compared the open coding in a group conversation to create the final codebook. During the group discussion, several themes related to TAMs [49,50] were identified, while other themes did not align with these models; yet, highlighting these additional themes was important to provide a holistic view of how ESs perceived and responded to ZEST-E. The final codebook was refined against one participant’s interview until 85% consistency [63] and Cohen’s kappa > 0.6 [64] were achieved. Two raters then independently coded the remainder of the interviews, and the third researcher provided clarifications during the process. Codes were organized as parent themes with sub-themes, as given in Table A1. Opinions of the ESs were often divided for each sub-theme, so we assigned a positive or negative valence to each coded instance of a sub-theme.
3. Results
3.1. Study Population
The demographic information for our participant population is given in Table 4.
3.2. Questionnaires
Results from the Technology Attitudes Questionnaire are shown in Figure 2, which indicate participants’ general attitudes towards technology. Outcomes from the ROQ [63] and ZEQ are given in Figure 3. Each theme in the ZEQ had a Cronbach’s alpha of 0.76–0.89, indicating strong internal consistency. Response distributions from the PIADS [53] and the NASA TLX survey [51,52] are presented in Figure 4. Outliers lying more than 1.5 IQR below the first quartile or above the third quartile are indicated with a small circle.
3.3. Exit Interviews
Insights and quotes from the semi-structured exit interviews are arranged by parent theme and sub-theme ID (Table A1). For clarity, quotes coded as suggestions are sorted into their corresponding parent themes. We indicate the number of participants whose responses were coded positively or negatively for each sub-theme; for example, sub-theme AD1 had two positive and three negative responses, and is notated below as (AD1; pos = 2, neg = 3). Participant IDs are specified in parentheses e.g., (S02).
3.3.1. Aesthetics and Design (AD)
(AD1; pos = 2, neg = 3): Two participants thought the robot’s appearance was unobtrusive, describing how its setup “didn’t feel crowded” in the experiment space (S06). These participants reported that the design was balanced and made them feel at ease. Two others expressed concern that the robot “doesn’t scream exercise” (S05) or that the robot “might be intimidating for some of my patients” (S11).
AD Suggestions: Improvements to the aesthetics of the system include making the robot’s end effector “more approachable” and adding target markings to the end effector (i.e., concentric circles) (S11).
3.3.2. Engagement and Motivation (EM)
(EM1; pos = 8, neg = 5): Several participants enjoyed the robot’s verbal cues to exercise at a specific rate. They also found the robot’s spoken encouragements, such as “you’re doing great” and “let’s make it harder”, to be engaging (S01). Others were more apprehensive about whether a robot would be used for exercise at home: “[my patients would] probably just occasionally talk to the robot and then just put it on the side, I think” (S08).
(EM2; pos = 5, neg = 3): Exercise specialists were optimistic that the robot could improve their patients’ adherence to at-home exercise plans. One participant said that using the robot at home would be their “number one” use case for the technology (S10), and others highlighted the potential for robotic exercise coaches to improve telemedicine for individuals who live far away from clinics (S04) or have difficulty leaving their homes (S01). Improving adherence to specific exercise instructions without supervision was a common theme:
This would be great… if they could have one (sic, robot) to go home with them to serve as motivation and also just give specific, clear instructions on how to perform a certain task because a lot of things about [exercise] form are often things that we can’t help them with when they’re not with us in person, especially with a home-based rehab program.(S07)
In contrast, one participant hypothesized that the robot would be less engaging once its novelty wore off: “I feel like if the system was set in someone’s home, they would probably use it one or two times and then it’d start getting [not so] interesting to interact with” (S08).
EM Suggestions: There were several suggestions for improving the engagement and motivating qualities of the system. These include adding accompanying music (S08), increasing the variability of the exercise pacing (S06), and adding more randomness to the motions that the robot directed (S08). One ES proposed adding more auditory and visual cues to the exercises (S03), and another suggested gamification improvements, e.g., adding a high score board, tracking performance between sessions, and adding a visual component to the dual-tasking exercises (S01).
3.3.3. Quality of Communication (QC)
(QC1; pos = 7, neg = 3): Feedback from ESs on the communication quality of ZEST-E was more positive than negative. Positive feedback highlighted that ZEST-E provided “clear, concise instructions” (S09) and offered good “encouragement and verbal cues” (S03) as well as good “auditory feedback” (S02).
On the other hand, participants who had negative views on the communication quality mentioned that they “had a hard time understanding some of the [robot’s] words clearly” (S06) and experienced confusion. One participant expressed that they “couldn’t figure out what [the robot] wanted from [them]” (S06).
(QC2; pos = 7, neg = 3): Participants generally had a positive outlook on the quality of the robot’s feedback. They appreciated that the feedback was “interactive,” “approachable,” and “not intimidating” (S02). One participant also found the robot’s “positive reinforcement” to be particularly “helpful” (S01). However, some participants felt that the robot’s feedback was too preprogrammed (S10).
QC Suggestions: Multiple ESs highlighted areas for improving the robot’s communication. Regarding the robot’s instructions, suggestions included creating a phone app to provide more exercise information (S07) and allowing the user to ask the robot to clarify or repeat instructions (S06). Accessibility concerns were raised, such as adding subtitles to the robot’s visual instructions, supporting other languages than English, and allowing the user to control the volume of the robot’s voice (S01). One participant wished the feedback could be “more dynamic” and “more like a trainer, rather than just passive like, [saying the same thing after every action, regardless of what’s going on]” (S10).
Specific improvements to the robot’s feedback include automatic detection of incorrect exercise form (S11), more nuanced feedback from the robot after sets beyond exercise score reporting (S06), and general improvements to the “sincerity” of the robot’s spoken feedback (S09) to make the interactions feel less “forced” (S10). One ES suggested that the robot should specifically encourage users to perform “full motions” during exercise sets (S11).
3.3.4. Usability and Reliability (UR)
(UR1; pos = 2, neg = 3): Three participants expressed concerns about the portability of the robot. One ES stated that the robot would not be accessible to patients in the home health community due to challenges with “lugging a robot around” (S01). Another highlighted the need to simplify or eliminate the “setup and breakdown” of the system (S02).
(UR2; pos = 8, neg = 4): Most participants thought that the system would be easy for ESs to set up and operate. They appreciated the combination of visual and verbal cues to teach the exercises. The system was reported to be “very easy to use, very easy to follow” (S08). However, some areas of improvement include further reducing user input during the exercise session (S03) and streamlining the robot setup process (S02).
(UR3; pos = 4, neg = 5): ESs less optimistic about PWP using the system.
I think how comfortable an individual is with technology is a huge component—that cannot be overlooked, especially [since] most Parkinson’s patients are older adults. There’s still a very large percentage of older adults that do not use smartphones, that do not use a lot of technology, so they may be very apprehensive if [the robot] is too much. That itself is too overwhelming. It doesn’t matter how great [the robot is].(S01)
Opinions were divided regarding the role of a caregiver operating the robot. One participant thought that “you could set it up in a way that someone could be pretty independent with using it with relatively low risk of injury” (S01), while another claimed that, “if somebody were to take it home at this stage, they wouldn’t be able to operate it independently. And I don’t even know that it would be able to be operated with a reasonably educated caregiver either” (S03).
UR Suggestions: Improvements to the usability of the system included making the robot voice-activated or operated with a single button press (S10). One ES expressed a general need for easier independent operation by patients (S03), and another requested the inclusion of “set workouts” that come with the robot (S05). Minimizing setup and breakdown complexity was also emphasized (S02). It was noted that there should be two versions of the system: one for use in a clinic and one for use at home (S10). That particular ES also proposed replacing the robot’s external screen with a tablet mounted on the robot (S10).
3.3.5. Function and Safety (FS)
(FS1; pos = 7, neg = 6): Opinions on the robot’s ability to adapt to individual physical capabilities were mixed. Some felt that “pretty much anybody could benefit from those exercises” (S03) due to their simplicity. However, others expressed concerns about performing the exercises incorrectly. One participant was unsure whether they should focus on speed or full range of motion, noting, “I felt myself not coming back fully on the chair or not standing up the whole way” (S11). Another participant worried that trying to complete more repetitions might lead to compromised movement quality, such as “not coming all the way back up” (S01) during exercises that required large vertical motions.
(FS2; pos = 3, neg = 4): There were differing opinions on how well the robot could serve PWP with varying symptoms. Some felt the robot could be effective if it could “calibrate the system or the programs based on the individual needs of the individual at that specific moment in time”, considering that PWP might have varying abilities throughout the day and at different “on/off” points in their medication cycles (S01). They also suggested that sessions might need to be “shortened” (S01) and adapted for those with severe mobility needs, allowing for breaks and assistance as required. Some participants felt that ZEST-E would be best suited for users who are “relatively cognitively intact” (S03) and that it should be designed for “someone at a high enough level to benefit from it, but not so advanced that the exercises would become unnecessary” (S03).
(FS3; pos = 3, neg = 1): Participants were split in their views on the robot’s safety. One participant felt that working with ZEST-E “could be pretty independent” with a “relatively low risk of injury” (S01). However, others raised concerns about fall safety. One participant feared that exercises like forward leaning could “throw [patients] off balance” or make them “dizzy,” and suggested that additional safety precautions and guidelines might be needed (S06).
(FS4; pos = 3, neg = 4): Participants were divided on whether the robot-led exercises were performed correctly. One participant appreciated the auditory feedback, saying it helped users realize they were using their full range of motion, which “you don’t normally get, just like typical exercise” (S02). However, others were concerned about the exercise speed, with one participant unsure if they should prioritize speed or full range of motion (S11). Another participant echoed this worry, expressing concern that focusing on repetitions might compromise the quality of movements, such as not fully returning to the starting position (S01).
FS Suggestions: Beyond the robot’s feedback system, ESs had several ideas for expanding the robot’s functionality. There was interest in using the robot to help people practice standing up (S01) and for gait training or as a walking aid (S03). One ES suggested having the robot monitor fall risks (S05), and multiple ESs expressed a general desire for an expanded repertoire of exercises, such as overhead reaching (S01), fine motor skill training (S01), or resistance exercises with a band (S07). Another ES requested a reduction in time between exercise sets to increase intensity (S10). Several ESs proposed further personalization options, such as more individualized difficulty and pace (S04), exercises in a larger workspace around the human (S08), calibrating the exercise difficulty based on outcome measures other than range of motion (S10), and automatically detecting the need to take a break (S01).
3.3.6. Healthcare Provider Considerations (HC)
(HC1; pos = 1, neg = 3): Several participants expressed concern that the system would be prohibitively expensive. Specifically, participants cited a need for robotic treatments to be covered by health insurance to appeal to most users.
Not everybody can afford their medications, so they’re not going to choose this versus pain meds or paying for groceries… It might be exclusionary from that regard.(S01)
(HC2; pos = 9, neg = 3): Most participants agreed that ZEST-E could improve their job efficiency inside and outside of the clinic. Helpful applications of a robotic exercise coach that were cited by participants included offloading repetitive tasks (S10), enabling a healthcare provider to work with many patients at once (S07), and serving as an instructional reference for patients to use during home exercise (S07). However, some participants expressed concern that the system would not offload enough work: “if it requires a bunch of input from me as a [physical therapist], I’d just rather do [the exercise coaching] myself” (S03).
(HC3; pos = 5, neg = 1): Exercise specialists were optimistic that the robot could improve their patients’ health outcomes. One participant highlighted the importance of external cues for exercise, stating that “[PWP] think that they’re doing full range of motion with things, but very often they’re not… [the robot has] that auditory feedback that you’re actually using your full range of motion” (S02). Another ES envisioned robot-led exercise as a useful starting point for individuals beginning exercise:
I think, at first, it would be easier to target the more sedentary people [with robot-led exercise]—get them to a level where they are comfortable, so then maybe [they will] seek out other resources, even just getting a gym membership or the personal trainer or things like that. Give them at least the ability to have a good foundation so they’re not starting cold, give them confidence to do that as well.(S04)
(HC4; pos = 4, neg = 2): Several individuals highlighted the potential for robots like ZEST-E to augment health data collection. It was noted by ESs that the performance measures that the robot collected may need to be improved and expanded to capture more comprehensive aspects of the exercise performance (S10).
HC Suggestions: Providing an interface for healthcare providers to customize the exercise sections (S11) and augmenting exercise statistics collected by the robot (S03) are two key areas for improvement. One participant noted that, “if it’s something that the patient can do without me, that’s great, but I don’t feel comfortable billing for that” (S06). In general, ESs “would have to know the cost” (S09) of the system; when one participant was told the price of the robot, they said that it “would have to be cheaper” (S01).
3.3.7. Expected Use Cases (EC)
(EC1; pos = 11, neg = 2): All participants in this study thought that the ZEST-E system would be useful for PWP. Several participants noted the system’s potential to help individuals with mobility issues (S02) and sedentary lifestyles (S04). Others thought that using ZEST-E would help PWP “maintain gains” made during physical therapy sessions (S01) and would help “promote” and “restore” physical activity (S10). Some highlighted the potential of the system to help individuals with cognitive impairments (S02), but noted that “you would have to determine what level on the MoCA [cognitive examination] that they would need [to understand the robot’s instructions]” (S11). One participant placed particular emphasis on the system’s ability to adapt to individuals’ needs:
Because people with Parkinson’s, a lot of times they may have time frames during the day where they can go out and ride a bicycle. Then, in the afternoon, if they’re taking medications—those are timed and really crucial—they could have trouble getting up and down from a chair. Being able to still have those different levels of activities based off of what their current needs are, I think, would be helpful.(S01)
(EC2; pos = 11, neg = 2): Additionally, all participants suggested that ZEST-E would be helpful for people with conditions other than PD. Suggestions were heavily focused on people with neurological conditions. Examples include, “any patient population—ortho, neuro” (S03), cardiology (S07), multiple sclerosis (S01), and stroke (S01, S08). In general, participants thought that robot-led exercise would be helpful for “anybody affected by any type of movement challenge” (S05), but others expressed concern that users “would have to be somebody who was relatively cognitively intact” (S03). Exercise specialists also expressed interest in using a system like ZEST-E as a gait assessment tool (S02, S03).
(EC3; pos = 7, neg = 2): Many exercise specialists noted the potential for ZEST-E to help healthy people as well. One participant claimed that “pretty much anybody could benefit from those exercises” (S03), and another thought that “there are plenty of patients that could use it just for the accuracy of the feedback on the exercise” (S06). In the context of telemedicine, it was noted that ZEST-E could be useful for “harder to reach population, [such as] rural populations” (S04). Beyond adults, a specialist hypothesized that, “I think it could be good for kids, but for the safety of the robot, maybe not. Kids tend to be kind of destructive in my experience” (S02).
Some participants thought that ZEST-E’s utility to healthy people might be limited. One participant said that ZEST-E would be useful for “more of a basic exercise, like just starting with warming up” (S08). Another expressed concern that, “as a healthy, independent person, there might not be a sincere need for me to use it… [unless] there was a very specific need within myself” (S07).
(EC4; pos = 11, neg = 2): All 11 participants thought that the robot would be useful in a clinic or home environment. In the clinic, specialists focused on how the robot could reduce their workload. Examples of integrating the robot into a clinical setting include using the robot for patient warm-ups (S08) and being “more efficient with the clinic time” (S04). Others expressed interest in offloading low-level coaching to the robot: “[while exercising with ZEST-E], the exercise prescription is out of the therapist’s hands and they’re more focused on the skill [that the patient is working on]” (S10) and “I could potentially be more productive, or doing something else at the same time but still being able to watch the qualitative nature of the exercise” (S06). Participants largely agreed that ZEST-E would fit naturally into a home health regimen. Several participants described the potential for ZEST-E to help people with exercises while they rest in bed (S03, S06). One person envisioned their use of ZEST-E as similar to existing home exercise protocols, but with better adherence reporting:
I think it could be useful as a home exercise program if the physical therapist could choose what exercises specifically that it wanted to perform and then getting some data or feedback in the clinic or how the patient has been doing at home. It could give some compliance feedback as well to see, did they actually do the exercises, and how did they perform when doing them?(S11)
Yet, there was concern that “if somebody were to take it home at this stage, they wouldn’t be able to operate it independently” (S03).
(EC5; pos = 5, neg = 1): Participants identified several locations other than a clinic or at home where a robot similar to ZEST-E could be useful. Some examples include, “small group workouts with everybody that’s familiar with [the robot]” (S05), “rehab space, research spaces” (S07), “a skilled nursing facility or… in a community center type of senior center” (S01), and gymnasiums inside of “assisted livings and independent living facilities” (S01).
4. Discussion
This study explored attitudes, perceptions, and beliefs of ESs about the usability of ZEST-E. It also sought to identify factors that facilitate or hinder the adoption of systems like ZEST-E in clinical and home environments. By combining quantitative measures from technology acceptance surveys with qualitative insights from semi-structured interviews, ESs described ZEST-E as having a high potential to enhance traditional rehabilitative exercise for PWP. ES participants highlighted key strengths, such as the ability of ZEST-E to provide personalized, engaging exercise sessions in various environments, and also offered concrete suggestions to improve ZEST-E: improving the quality of the robot’s instructional feedback and increasing the ease of use of ZEST-E for both clinicians and PWP.
4.1. Strengths of Robot-Led Exercise
ESs identified many strengths and promising potentials for robot-led physical therapy, which fell under several broad themes that are examined in the following sections.
4.1.1. Robots Like ZEST-E Have the Potential to Be Useful in Clinics, Homes, and Other Spaces
Several ESs described use cases for ZEST-E inside the clinic. Benefits of including a robotic exercise aid in clinical treatment included offloading coaching warm-up exercises and providing low-level feedback on specific motions. Incorporating robotic exercise aids would also enable ESs to work with more patients at the same time. Including a physical external target placed by the robot to “cue” stretching motions, as well as incorporating auditory feedback upon successfully reaching the target, encouraged participants to perform their full range of motion. Though, the effectiveness of auditory feedback in noisy environments, such as in group settings, remains to be evaluated. ESs also hypothesized that exercising with ZEST-E could be helpful for others without PD, such as stroke survivors or even healthy older adults.
ESs highlighted many scenarios in which they could imagine using a system like ZEST-E outside of the clinic. Multiple ESs thought that ZEST-E could be used for maintaining gains made in the clinic between clinic visits. ESs were interested in deploying ZEST-E in shared health and living spaces, as well as in telemedicine contexts, such as in their patients’ homes, and especially with rural populations. Also, using a robot to guide rehabilitative exercises creates an opportunity to collect and track rich, long-term health data inside and outside of the clinic, which can be used by ESs to improve treatment plans. ESs emphasized the ability of ZEST-E to work with people of varying degrees of mobility by leading seated as well as standing exercises, and they mentioned the possibility of including new exercises for individuals lying in bed. These results suggest that there are broad opportunities for robot-led rehabilitative exercise inside and outside of the clinic.
4.1.2. Robots Like ZEST-E Could Provide Effective and Personalized Care to PWP
Participants reported that the system was adaptable to individuals, as shown by positive PIADS ratings (Figure 4) and high ratings for performance and therapeutic efficacy in the ZEQ (Figure 3). Further, ESs expressed optimism that a system like ZEST-E would improve adherence to at-home exercise. Of specific interest was giving patients the ability to time their exercise sessions based on their on–off medication cycles throughout the day without having to leave their homes. These findings indicate that robots like ZEST-E could provide effective and personalized care to PWP.
4.1.3. ZEST-E Is Engaging
The multimodal interaction between ZEST-E and participants resulted in ESs rating the system as highly engaging. Sound effects, two-way verbal interactions, and video instructions were all cited as positive attributes of the system. ESs highlighted the importance of encouragement delivered by the robot during exercises to boost engagement. Perceived enjoyment was rated highly (Figure 3), which indicates that the robotic exercise system was effective at engaging patients, and engagement ratings from the ZEST-E evaluative questionnaire (Figure 3) were also positive.
4.2. Potential Improvements
A large focus of the ESs during the semi-structured interviews was on suggestions for improving the ZEST-E system. We categorized their feedback into two broad groups that address distinct sets of potential improvements: quality of exercise instruction and ease of use.
4.2.1. Improving the Quality of Robotic Exercise Coaching
ESs identified several features missing from ZEST-E that a human exercise coach would typically include. These enhancements could improve the ability of a robot exercise coach to guide sessions effectively, whether working under human supervision or operating independently.
First, ESs expressed the need for ZEST-E to monitor participants’ form during exercises and offer corrective feedback if form deviates from the ideal. Since each exercise was scored by ZEST-E based on the number of repetitions completed, users may be encouraged to cheat and not go through their full range of motion to score points more quickly. It was suggested that monitoring participants’ form would also indicate high fatigue levels, so that ZEST-E could automatically stop the set when exercise form degraded due to fatigue. Also, monitoring fall risks was a concern among several ESs, especially when considering deploying ZEST-E in environments outside of the clinic without someone to supervise present. Incorporating a computer vision or wearable sensor-based exercise form feedback and/or fall risk detection system would make ZEST-E a more effective and safe exercise instructor.
Some ESs thought that the current interaction scheme between ZEST-E and the user was “too robotic” or not interactive enough. All ZEST-E’s spoken phrases were chosen by investigators before the study; while ZEST-E varied its selection of the spoken phrases, some users felt that ZEST-E was behaving in a way that felt inauthentic and preprogrammed, which reduced engagement. Also, ZEST-E was unable to handle requests for repeating instructions or clarifying instructions to address exercise form deviations. ZEST-E also could not make small talk during a session, which led to some participants evaluating the human–robot interaction as too “forced”. Augmenting ZEST-E’s conversation engine using a more sophisticated language processing scheme, such as a large language model (LLM), and an improved tone of voice could improve users’ enjoyment and decrease confusion while interacting with ZEST-E.
While ESs remarked favorably about the exercise designs, many expressed a desire for ZEST-E to lead a wider variety of exercises. Specific exercise suggestions included gait training, seated to standing transitions, overhead reaching, fine motor skills, or resistance training. However, many of these exercise types are not as well suited to be led by a robot like ZEST-E. Because ZEST-E is lightweight and has a small footprint, exerting large forces on the robot would cause it to tip over [59]. This device is not suitable for resistance training, and it raises safety concerns for exercises such as gait and transfer training, which involve a higher fall risk, since the robot cannot catch a falling participant. Additionally, ZEST-E’s reachable workspace is between the floor and approximately 1.3 m above the ground [59], which limits the height at which ZEST-E can place the target for overhead reaching exercises. The development of mobile robots suitable for gait training warrants further investigation.
4.2.2. Improving Ease of Use
ESs identified many ways to improve the ease of use while operating ZEST-E. From the perspective of an ES using ZEST-E in a clinic, participants highlighted the need to minimize robot setup time and maximize ease of operation. This includes minimizing the number of inputs to the system that the operator must make, as well as increasing the robot’s level of autonomy from leading single exercise sets to leading entire routines. In addition, while ZEST-E is able to be transported by a single human without peripheral equipment [59], ESs expressed a desire for an even more portable robot. Despite these suggestions, the system in its current state had high ratings for its Perceived Ease of Use in the ROQ (Figure 3).
Several other key improvements were also identified to make the system easier for PWP to use on their own outside of the clinic. In this context, ESs provided further emphasis that ZEST-E should operate mostly autonomously, especially for older adults who have lower levels of technological literacy. Alternative modalities to interact with the robot, such as a direct voice interface to launch exercises, would reduce barriers for PWP using a system like ZEST-E independently. Including further accessibility options, such as adding subtitles to ZEST-E’s screen for spoken instructions and adding other languages, would further decrease barriers to adoption. These suggestions were supported by mixed ratings for ease of use for patients in the ZEST-E Evaluative Questionnaire and in the broad spread of Perceived Usefulness ratings from the ROQ (Figure 3).
4.3. Limitations and Future Work
While this study provides valuable descriptive insights into ESs perceptions of ZEST-E, several limitations must be acknowledged. Despite the small sample size ( ) recruited for this study, the consistency of responses among ES participants highlights ZEST-E’s potential and provides clear avenues for refinement. These preliminary findings lay the foundation for larger-scale studies to validate the usability and acceptance of ZEST-E and to guide iterative design improvements that further support clinicians and PWP in diverse settings. Additionally, our study does not compare ZEST-E against another robotic exercise system, nor does it compare two different configurations of ZEST-E. Future work should compare an exercise form feedback-enhanced ZEST-E to the current version, measure short-term flexibility gains before and after exercising with ZEST-E, and conduct fully powered A/B tests against standard rehabilitation protocols to confirm ZEST-E’s added value.
5. Conclusions
Integrating therapeutic robotic systems into established rehabilitation programs for PWP shows significant promise. Our mixed-methods study indicates that a platform such as ZEST-E can deliver engaging, personalized support in clinics, homes, and other environments. Yet, further refinement is needed to strengthen the robot’s instructional abilities and enable smooth integration into routine therapy. Future research, particularly on therapist–patient–robot triad interactions in a clinical setting, could reveal additional opportunities to improve robotic therapy for PWP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization World Report on Ageing and Health World Health Organization Geneva, Switzerland 2015
- 2Feigin V.L. Vos T. Alahdab F. Amit A.M.L. Bärnighausen T.W. Beghi E. Beheshti M. Chavan P.P. Criqui M.H. Desai R. Burden of neurological disorders across the US from 1990–2017: A global burden of disease study JAMA Neurol.2021781651763313613710.1001/jamaneurol.2020.4152 PMC 7607495 · doi ↗ · pubmed ↗
- 3Yang W. Hamilton J.L. Kopil C. Beck J.C. Tanner C.M. Albin R.L. Ray Dorsey E. Dahodwala N. Cintina I. Hogan P. Current and projected future economic burden of Parkinson’s disease in the US Npj Park. Dis.202061510.1038/s 41531-020-0117-132665974 PMC 7347582 · doi ↗ · pubmed ↗
- 4Factor S. Scullin M. Sollinger A. Land J. Wood-Siverio C. Zanders L. Freeman A. Bliwise D. Goldstein F. Freezing of gait subtypes have different cognitive correlates in Parkinson’s disease Park. Relat. Disord.2014201359136410.1016/j.parkreldis.2014.09.02325446341 PMC 12320556 · doi ↗ · pubmed ↗
- 5Pal G. O’Keefe J. Robertson-Dick E. Bernard B. Anderson S. Hall D. Global cognitive function and processing speed are associated with gait and balance dysfunction in Parkinson’s disease J. Neuroeng. Rehabil.2016139410.1186/s 12984-016-0205-y 27793167 PMC 5084375 · doi ↗ · pubmed ↗
- 6Stegemöller E.L. Nocera J. Malaty I. Shelley M. Okun M.S. Hass C.J. NPF Quality Improvement Initiative Investigators Timed up and go, cognitive, and quality-of-life correlates in Parkinson’s disease Arch. Phys. Med. Rehabil.20149564965510.1016/j.apmr.2013.10.03124291596 · doi ↗ · pubmed ↗
- 7Pretzer-Aboff I. Galik E. Resnick B. Parkinson’s disease: Barriers and facilitators to optimizing function Rehabil. Nurs.200934546010.1002/j.2048-7940.2009.tb 00249.x 19271659 · doi ↗ · pubmed ↗
- 8Litvan I. Aarsland D. Adler C.H. Goldman J.G. Kulisevsky J. Mollenhauer B. Rodriguez-Oroz M.C. Tröster A.I. Weintraub D. MDS Task Force on mild cognitive impairment in Parkinson’s disease: Critical review of PD-MCI Mov. Disord.2011261814182410.1002/mds.2382321661055 PMC 3181006 · doi ↗ · pubmed ↗