The 2025 European Cystic Fibrosis Society position statement on physical activity assessment in cystic fibrosis
Craig A. Williams, Brenda Button, Tiffany J. Dwyer, Elpis Hatziagorou, Kelly A. Mackintosh, Melitta A. McNarry, Dewi Paris, James Shelley, Helge Hebestreit, Judy Bradley, Mayara Silveira Bianchim

TL;DR
This paper updates guidelines for measuring physical activity in cystic fibrosis patients, emphasizing device-based metrics and validated questionnaires.
Contribution
The paper provides updated, evidence-based recommendations for assessing physical activity in cystic fibrosis clinical practice and research.
Findings
Device-based metrics should include time spent in different activity intensity categories and sedentary/sleep time.
Data resolution should be at least 1 second to accurately categorize physical activity patterns.
Validated questionnaires and diaries can supplement device-based assessments but serve different purposes.
Abstract
Recent advances in the measurement of physical activity have significantly enhanced the analyses and interpretation in relation to health and well-being. Thus, we sought to revise and expand the 2015 position statement on the measurement of physical activity and provide guidance to clinicians and researchers for measuring physical activity in cystic fibrosis (CF) clinical practice and research. This study was registered with the International Prospective Register of Systematic Review (PROSPERO) database (CRD42022292165). Three databases (Medline, Embase and Cumulative Index to Nursing and Allied Health Literature) were searched for studies investigating the measurement of physical activity and sedentary time in people with CF irrespective of age or duration. The Quality Assessment for Diverse Studies was used to assess methodological concern. A mixed-methods framework synthesis was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
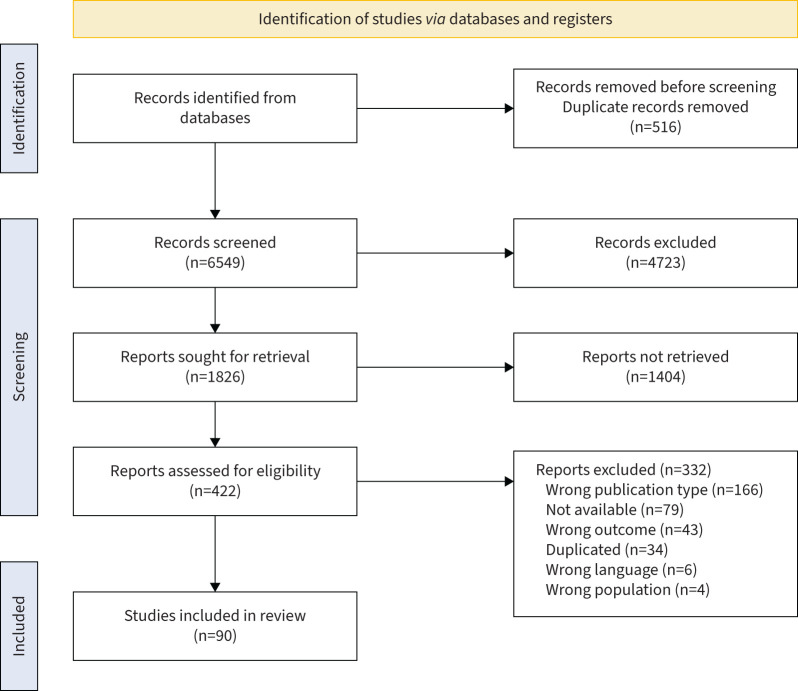 FIGURE 1
FIGURE 1| Study, year | Characteristics |
|---|---|
|
| |
| Methods | Design: RCT |
| Participants | 42 participants with CF |
| Intervention | Randomly selected into intervention (group A) or control (group B) groups |
| Outcomes | Functional capacity assessment (6MWT), echocardiographic studies and step count |
| Notes | A G1 (Garmin) WAT was used for the assessment of physical activity |
|
| |
| Methods | Design: cross-sectional |
| Participants | 47 participants with CF, 39 control subjects |
| Intervention | PA measured across 7 days on participant's right hip during the day |
| Outcomes | This study examined |
| Notes | The assessment of PA used an Actigraph GT3X |
|
| |
| Methods | Design: RCT |
| Participants | 16 participants with CF |
| Intervention | Each subject was studied twice, 3–7 days before administration of IVAT and 5–10 days after completion of 14 days IVAT |
| Outcomes | This study examined |
| Notes | This study was conducted in the Clinical Research Center of Lille, University Hospital (CIC-9301-INSERM-CHU). |
|
| |
| Methods | Design: observational study |
| Participants | 16 participants with CF, nine boys and seven girls, median weight of 33.7 kg (range 20.5–46.8 kg), FFM of 26.5% (18.0–41.7%) and height of 141 cm (range 118–157 cm) |
| Intervention | Each subject was studied twice before and after IVAT both in laboratory conditions in hospital and in free-living conditions during a school day |
| Outcomes | This study examined PA (counts·min−1), DEE (kJ·min−1·kg−1 FFM), PAEE (kJ·min−1·kg−1 FFM), PAEE/PA (kJ·min−1·kg−1 FM/counts), forced vital capacity, FEV1, PEF and FEF25–75% |
| Notes | This study was carried out in the Clinical Research Center of Lille, University Heart Hospital (CIC-9301-INSERM-CHU) |
|
| |
| Methods | Design: compositional analysis |
| Participants | 129 participants with CF |
| Intervention | Wrist-worn accelerometery was used to assess PA, SED and sleep |
| Outcomes | This study examined SED, LPA, MVPA and sleep |
| Notes | This study noted the importance of prioritising sleep as reductions in sleep were associated with detrimental effects in lung function |
|
| |
| Methods | Design: RCT |
| Participants | 71 participants with CF |
| Intervention | PA was assessed for 7 consecutive days using a nondominant wrist-worn ActiGraph GT9X |
| Outcomes | This study examined SED, LPA, MPA, VPA, MVPA and sleep |
| Notes | Aim to compare the use of generic and CF-specific cut-points to assess movement behaviours in children and adolescents with CF |
|
| |
| Methods | Design: retrospective study |
| Participants | 111 participants with CF |
| Intervention | Retrospectively reviewed clinical data, according to two periods: pre-lockdown (from October 2019–March 2020) and post-lockdown (from May 2020–October 2020) |
| Outcomes | This study examined weight, BMI, respiratory function and amount of PA |
| Notes | This study examined the effect of lockdown during the COVID-19 pandemic and reported improvements in weight and some stabilisation and improvement of lung function in some patients with CF |
|
| |
| Methods | Design: retrospective study |
| Participants | 115 participants with CF, 59 females, 56 males, 93.9% White, 3.5% Black and 2.6% other |
| Intervention | PA was assessed using questions from the Centers for Disease Control's Youth Risk Behaviour Survey |
| Outcomes | This study examined VPA, participation in school or community sports teams, participation in physical education |
| Notes | This work was prepared in conjunction with the Division of Innovation and development Services of the North Carolina Department of Public Instruction |
|
| |
| Methods | Design: controlled cross-sectional study |
| Participants | 153 participants with CF |
| Intervention | Bone densitometry measurements of TB, LS, femoral neck, cortical radius and ultra distal radius measured using DEXA |
| Outcomes | This study examined BMD, vitamin D status, PA, dietary intake, corticosteroid exposure, fracture incidence and associations with BMD in individuals with CF |
| Notes | The study was supported by Cystic Fibrosis Research Australia Pty Ltd and the Royal Children's Hospital Foundation |
|
| |
| Methods | Design: controlled longitudinal study |
| Participants | 40 participants with CF |
| Intervention | Areal BMD of the TB, LS and total femoral neck were repeatedly measured in 85 subjects aged 5–18 years with CF and 100 age- and sex-matched controls over 2 years |
| Outcomes | This study examined BMD, corticosteroid exposure and fracture incidence |
| Notes | This study examining bone density used DXA |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 60 participants with CF |
| Intervention | CPET was used to determine |
| Outcomes | This study examined mean CRF, CFRLD, IGT including CFRD, |
| Notes | Data presented earlier at the European Cystic Fibrosis Society Conference 2021 ( |
|
| |
| Methods | Design: cross-sectional, descriptive study |
| Participants | 46 participants with CF |
| Intervention | 7-day PA recall questionnaire, Twin City Walking Survey |
| Outcomes | This study examined PA level, exercise preference, exercise readiness and exercise barriers |
| Notes | A 7-day PA recall questionnaire during a structured interviewed assessed activity levels |
|
| |
| Methods | Design: prospective case–control study |
| Participants | 19 participants with CF |
| Intervention | Muscle strength assessment, spirometry and venous blood sampling were performed at the beginning (day 1) and at the end of IVAT (day 14) and 1 month after IVAT (day 40±3 days) |
| Outcomes | This study examined assessment of quadriceps strength, PA, spirometry, 6MWD and blood analysis |
| Notes | This study used a SenseWear Pro Armband to quantify PA |
|
| |
| Methods | Design: single-centre prospective cohort observational study |
| Participants | 31 participants with CF |
| Intervention | CF patients enrolled at the end of an inpatient admission at The Prince Charles Hospital, Brisbane |
| Outcomes | This study examined sputum supernatant and plasma concentration of IL-6, IL-8 and TNF-α |
| Notes | This study was registered with Physiotherapy Theory and Practice |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 30 participants with CF, 25 control participants |
| Intervention | A questionnaire assessing PA level and video games played on two consoles with 10-min intervals to assess physiological variables |
| Outcomes | This study examined exercise capacity values for resting, anaerobic threshold and peak exercise periods, HR, ventilation, |
| Notes | This study was registered as number |
|
| |
| Methods | Design: case series |
| Participants | Three participants with CF |
| Intervention | Participants completed an exhaustive maximal cardiopulmonary exercise test on a cycle ergometer to determine |
| Outcomes | This study examined FVC, FEV1, oxygen saturation, BMI, gas exchange, total PA and |
| Notes | In two of the three case studies a GENEActiv accelerometer was used to measure PA |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 114 participants with CF |
| Intervention | BMD measurements made at LS (L2–L4), right femoral neck and TB |
| Outcomes | This study examined BMD measurements, blood samples and nutritional data |
| Notes | Adult patients with CF showed a high prevalence of vitamin D insufficiency |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 26 participants with CF |
| Intervention | Participants completed seven PA tasks with simultaneous assessment of EE, a mix of static tasks and active tasks |
| Outcomes | This study examined EE and exhaled respiratory gases |
| Notes | EE from the SenseWear armband resulted in a moderate degree of agreement with EE measurements from indirect calorimetry |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 10 participants with CF |
| Intervention | Each subject logged into ActivOnline a mean± |
| Outcomes | Feasibility of software to encourage activity participation assessed by frequency of site access, number of activity sessions recorded and number of telephone consultations undertaken |
| Notes | This study utilised a specifically designed internet-based PA programme |
|
| |
| Methods | Design: observational study |
| Participants | 65 participants with CF |
| Intervention | PA monitoring at baseline and after 12 months |
| Outcomes | This study examined PA, pulmonary function, exercise capacity and CF-related QoL assessed during a stable phase |
| Notes | This study was registered as ACTRN12610000949088 at the Australian New Zealand Clinical Trials Registry |
|
| |
| Methods | Design: observational study |
| Participants | 65 participants with CF |
| Intervention | PA monitoring at baseline and after 12 months |
| Outcomes | This study examined PA, pulmonary function, exercise capacity and CF-related QoL assessed during a stable phase |
| Notes | This study is a secondary analysis of C |
|
| |
| Methods | Design: RCT |
| Participants | 107 participants with CF |
| Intervention | All participants received usual care and were provided with information, |
| Outcomes | This study examined change in device-based average daily MVPA from baseline to the end of the 12-week intervention period, measures of PA (self-reported), self-determination for exercise, HRQoL, psychological well-being, exercise capacity (MST) and lung function |
| Notes | This study was registered as ACTRN12617001009303 at the Australian New Zealand Clinical Trials Registry |
|
| |
| Methods | Design: observational study |
| Participants | 21 participants with CF |
| Intervention | Participants walked on a treadmill for 5 min at five pre-determined speeds and at three self-determined speeds along a corridor, accelerometers were worn |
| Outcomes | This study examined observer step count and device step count (×2) |
| Notes | This work was supported by Truck Run 4 Katie, the Health Research Institute and the University of Limerick |
|
| |
| Methods | Design: observational study |
| Participants | 33 participants with CF |
| Intervention | Participants were instructed to wear an accelerometer continually for 7 days, at the end of which, the participants returned to an adult CF unit, for exercise testing, spirometry and completion of questionnaires |
| Outcomes | This study examined PA, aerobic capacity, sleep and well-being |
| Notes | This observational study design followed the STROBE standardised reporting guidelines to conduct and report the study |
|
| |
| Methods | Design: pilot randomised trial |
| Participants | 33 participants with CF |
| Intervention | The 12-week intervention consisted of technology (Fitbit Charge 2) which was remotely monitored and participants set step count goals |
| Outcomes | This study examined PA, aerobic capacity, lung function, sleep, QoL and well-being |
| Notes | The study protocol is registered on ClinicalTrials.gov ( |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 18 participants with CF |
| Intervention | Adults with CFRD were recruited from a hospital-based CF clinic PA was measured using 7-day PA recall (telephone interview), adherence to CFRD management with the Self-Care Inventory–Revised (questionnaire) and blood glucose control from glycated haemoglobin levels documented in participants’ medical charts within 3 months |
| Outcomes | This study examined amount of time spent in different types of PA |
| Notes | First study to describe PA levels in individuals with CFRD |
|
| |
| Methods | Design: secondary analysis of a study cohort |
| Participants | 28 participants with CF |
| Intervention | FFM index measured using bioelectrical impedance, lung function using spirometry, number of shuttles as a measure of exercise tolerance and the reported PA in children |
| Outcomes | This study examined FFM, BMI, pulmonary function and respiratory muscle testing, HAES and the MST |
| Notes | The HAES assessed inactive and active periods of the day and included documentation of waking, sleeping and mealtimes |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 30 participants with CF |
| Intervention | During a consultation, a spirometry test was undertaken; then, participants were referred to perform an HRV assessment using a cardiofrequency meter |
| Outcomes | This study examined lung function, levels of daily activity, resting and peak exercise values |
| Notes | This study noted a sympathetic HRV predominance and normal physiological exercise response in children and adolescents with mild-to-moderate CF |
|
| |
| Methods | Design: RCT |
| Participants | 15 participants with CF |
| Intervention | Participants performed a maximal CPET and two localised calf muscle tests (maximal incremental and constant-load) using magnetic resonance spectroscopy |
| Outcomes | This study examined baseline characteristics, muscle energetic kinetics during and after calf exercises, maximal incremental plantar flexion test, and constant load plantar flexion test |
| Notes | The only study to measure phosphocreatine recovery, an indicator of maximal oxidative capacity and PA |
|
| |
| Methods | Design: method comparison study |
| Participants | Five participants with CF |
| Intervention | Spirometry testing was performed, as was a standardised incremental cycle ergometer |
| Outcomes | This study examined EE, |
| Notes | This study used both the SenseWear armband and an Actical accelerometer to assess PA |
|
| |
| Methods | Design: sub-analysis of a previous study |
| Participants | 109 participants with CF |
| Intervention | Sleep monitor worn for 4 weeks on the nondominant hand |
| Outcomes | This study examined steps·day–1, amount of sedentary/light/moderate/vigorous/very vigorous exercise, sleep efficiency, time in bed, total sleep time and waking after sleep onset |
| Notes | Sub-analysis of the CFmobil project, a 12-month partially supervised exercise programme for CF patients ≥6 years of age |
|
| |
| Methods | Design: case–control study |
| Participants | 22 participants with CF |
| Intervention | Participants completed a quality-of-life questionnaire, underwent polysomnography while breathing room air with evening and early-morning arterial blood gases, also on room air, and had neurobehavioral testing, before and after inpatient treatment of an exacerbation |
| Outcomes | This study examined sleep architecture, gas exchange and the Neurobehavioral Assessment Battery |
| Notes | This study demonstrated that exacerbations of lung disease in young adults with CF adversely affected sleep and neurobehavioral performance, irrespective of disease severity |
|
| |
| Methods | Design: Evaluation of Accuracy of SenseWear Activity Monitor |
| Participants | 17 participants with CF |
| Intervention | Spirometry testing prior to exercising |
| Outcomes | This study examined exercise intensity, EE and step count |
| Notes | The SenseWear armband significantly underestimated EE at higher exercise intensities |
|
| |
| Methods | Design: case–control study |
| Participants | 20 participants with CF |
| Intervention | Accelerometer was used for a period of 7 consecutive days. |
| Outcomes | This study examined time spent sitting, number of sitting bouts, time standing, time in PA, steps per 24 h, time spent sleeping, number of participants not meeting steps recommendation and not meeting sleep recommendation |
| Notes | The activPAL micro monitor was used to measure PA |
|
| |
| Methods | Design: observational, case–control study |
| Participants | 40 participants with CF, 22 males |
| Intervention | Body composition, pulmonary function and PA status were determined at initial screening |
| Outcomes | This study examined body composition, pulmonary function, PA status, FFM, diaphragm thickness, lung function, circulating CRP, PA and inspiratory muscle function |
| Notes | A loss of FFM coupled with worsening pulmonary disease resulted in inspiratory muscle function loss, which was associated with significant atrophy of the diaphragm and closely related to a reduction in PA in CF patients |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 51 participants with CF |
| Intervention | Nutritional and sleep questionnaires were answered by the participants |
| Outcomes | This study examined PASP, Epworth sleepiness scale, Pittsburgh sleep quality index score, sleep stage score, rapid eye movement, apnoea/hypopnoea index and 6MWD |
| Notes | A range of questionnaires, including the World Health Organization Quality of Life and the Cystic fibrosis Quality of Life, were utilised in this study |
|
| |
| Methods | Design: case–control study |
| Participants | 45 participants with CF |
| Intervention | Subjects completed two self-administered validated questionnaires, the Godin Leisure-Time Exercise Questionnaire and the DISABKIDS for QoL |
| Outcomes | This study examined QoL and PA |
| Notes | The Godin Leisure-Time Questionnaire was used in this study with the DISABKIDS questionnaire assessing QoL |
|
| |
| Methods | Design: cross-sectional observational study |
| Participants | 81 participants with CF |
| Intervention | Participants completed a variety of tests including anthropometric and lung function, estimation of maturity (self-report), HAES PA questionnaire, completion of a food frequency questionnaire for rapid assessment of calcium- and vitamins D- and K-rich foods, DEXA for whole body assessment of bone mineral content, resting blood measurements of analysis of calcium and alkaline phosphatase, serum analysis of CRP, 25OHD, parathyroid hormone, vitamin K, osteocalcin (total and undercarboxylated), and carboxy-terminal PICP (a marker of bone formation), and citrated plasma for citrated plasma for protein induced by vitamin K absence or antagonist-II |
| Outcomes | The primary outcomes were vitamin K and calcium status |
| Notes | Considering that PA is a potent determinant of bone health at this pre-pubertal and pubertal maturity status, little was mentioned about the influence of PA |
|
| |
| Methods | Design: RCT |
| Participants | 14 participants with CF |
| Intervention | The CFmobil project was initiated to establish sport and exercise as additional additions of CF therapy to further improve patients’ care |
| Outcomes | Anthropometric, lung function, cardiorespiratory fitness through a CPET, assessment of PA through an accelerometer and actigraphy reported as METs (light (<3 METs·min−1·day−1), moderate (3.0–5.9 METs·min−1·day−1) and vigorous (≥6 METs·min−1·day−1)) |
| Notes | Of the 14 children, only six children completed the partially monitored, 12-month exercise programme |
| Methods | Design: pre-experimental study one-group pre-test–post-test intervention study |
| Participants | 31 participants with CF |
| Intervention | Spirometry was carried out, followed by an incremental cycling test on a cycle ergometer |
| Outcomes | This study examined DMT, steps·day−1, SED, light/moderate-to-vigorous/vigorous intensity activity |
| Notes | This study was registered at ClinicalTrials.gov ( |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 25 participants with CF |
| Intervention | Habitual PA level and self-esteem data collected |
| Outcomes | This study examined exercise testing results, PA level, physical self-perception profile, pulmonary function and CFTR genotype |
| Notes | This study used the Adherence to Quantitative Activity Protocol questionnaire to assess PA |
|
| |
| Methods | Design: randomised control study |
| Participants | 52 participants with CF |
| Intervention | Maximal exercise testing done on a treadmill, with HR being monitored by a continuous ECG |
| Outcomes | This study examined whole body and LS BMD, pulmonary function, exercise capacity, daily PA and QoL |
| Notes | This study was registered with Clinical Trials Registry-India (REF/2013/01/004447) |
|
| |
| Methods | Design: single-centre prospective study |
| Participants | 40 participants with CF |
| Intervention | DEXA scans, spirometry measurements were performed |
| Outcomes | This study examined BMD and disease severity (measured as Shwachma–Kulczycki score) |
| Notes | This study used the Garmin Vívosmart 4 smart watch to measure PA |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 22 participants with CF |
| Intervention | 3-day weighed food diary and stool collection and fasting venous blood samples collected at time of body composition |
| Outcomes | This study examined energy intake, PA (J·day−1), DEXA fat-free soft tissue, height, weight and BMD |
| Notes | A 7-day diary and self-report questionnaire were completed within 2 weeks of body composition analysis to assess weekly EE based on type and duration of physical activities |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 74 participants with CF |
| Intervention | Skin fold thickness measured and spirometry undertaken |
| Outcomes | This study examined |
| Notes | This study monitored PA for 7 days using the MTI/CSA 7164 accelerometer |
|
| |
| Methods | Design: RCT |
| Participants | 23 participants with CF |
| Intervention | Patients given an HR monitor and were given an individualised activity plan |
| Outcomes | This study examined |
| Notes | This study had patients in the intervention group consent to increase their sport activities by a minimum of 3660 min·week−1 for the first 6 months of the study |
|
| |
| Methods | Design: cross-sectional analysis of separate intervention studies |
| Participants | 76 participants with CF |
| Intervention | QoL measure |
| Outcomes | This study examined HRQoL, reported PA, height, weight, BMI, body composition (percent body fat), pulmonary function (FEV1), short-term muscle power, maximal aerobic work rate, |
| Notes | Data for this project was taken from two intervention studies, one of which being H |
| Methods | Design: parallel-arm multicentre RCT |
| Participants | 1117 participants with CF |
| Intervention | Patients were seen twice within 4 weeks, then every 3 months for 1 year thereafter |
| Outcomes | This study examined change in predicted FEV1 from baseline, changes in PA, exercise capacity, pulmonary function, body composition, QoL, depression, anxiety and stress scales, exercise motives as well as glycaemic control and time to first exacerbation |
| Notes | This study was a parallel-arm RCT (Clinicaltrials.gov identifier: |
|
| |
| Methods | Design: case–control study |
| Participants | 22 participants with CF |
| Intervention | Venous blood samples obtained, spirometry undertaken, 24-h urine collected and 3-day food intake diary completed |
| Outcomes | This study examined body composition, bone metabolism, inflammatory status, clinical status and catabolic status |
| Notes | This study used a recall questionnaire for the month before the assessment when patients were clinically stable to measure PA |
|
| |
| Methods | Design: case–control study |
| Participants | 66 participants with CF |
| Intervention | Spirometry undertaken and an accelerometer worn for nine consecutive days on right hip |
| Outcomes | This study examined amount of strenuous activity |
| Notes | This study had participants wear an accelerometer (GT1M, ActiGraph, Pensacola, FL), with a minimum of 3 days of valid recordings including 1 weekend day, and at least 10 h of valid data each day for acceptable PA assessment |
|
| |
| Methods | Design: case–control study |
| Participants | 45 participants with CF |
| Intervention | Subjects receiving community treatment had baseline assessments performed in the clinic area immediately following the decision to start IVAT and follow-up assessments were performed when patients re-attended immediately after completing IVAT |
| Outcomes | This study examined activity level, energy balance, QoL, body weight and spirometry |
| Notes | This study used an Actigraph® GT3X activity monitor (tri-axial accelerometer), for 3 consecutive days during the first week and 3 consecutive days during the second week of IVAT |
|
| |
| Methods | Design: RCT |
| Participants | 20 participants with CF |
| Intervention | Randomly assigned to training group or control group |
| Outcomes | This study examined anaerobic performance, mean power, aerobic performance and QoL |
| Notes | The adherence was judged to be excellent with a 98% attendance level at the exercise sessions |
|
| |
| Methods | Design: cross-sectional study with age- and sex-matched control group |
| Participants | 18 participants with CF (10 males) confirmed by a sweat chloride >60 mmol·L−1 and genotyping (8 ΔF508 homozygote, 10 ΔF508 heterozygous; 4 CFRLD) |
| Intervention | Hip-mounted ActiGraph GT3X+ accelerometer (ActiGraph LLC, Pensacola, FL) worn by both groups to assess habitual PA level over 7 consecutive days |
| Outcomes | This study examined lung function, body stature and mass, waist circumference, SED, low LPA, high LPA, LPA, MPA and VPA |
| Notes | Besides summing MPA and VPA to classify MVPA, these authors also designated the remainder of the time as either low LPA (100−799 counts·min−1) or high LPA (800 counts·min−1 <4 METs) |
|
| |
| Methods | Design: cross-sectional study with age- and sex-matched controls |
| Participants | 25 participants with mild-to-moderate CF, confirmed by a sweat chloride >60 mmol·L−1 and genotyping (11 homozygote, 14 heterozygote; 3 CFRLD; 1 CFRD), recruited from a UK CF outpatient clinic |
| Intervention | PA and SED were measured using a hip-mounted ActiGraph GT3X+ accelerometer (ActiGraph LLC, Pensacola, FL) for 7 consecutive days, advised to remove it for water-based activities ( |
| Outcomes | This study examined lung function, body stature and mass, SED, LPA, MPA and VPA |
| Notes | A valid day was defined as at least 9 h of wear-time |
|
| |
| Methods | Design: cross-sectional study with control group |
| Participants | Participants with CF (nine boys, six girls) |
| Intervention | PA was assessed in the CF group using nonspecified questionnaire during both week and weekend days |
| Outcomes | This study examined body stature and mass, skinfold measurements, lung function, plasma biochemical measurements, |
| Notes | A highly technical protocol, the deuterium oxide (2H2O) dilution method, was used to assess TB water and FFM according to the appropriate hydration indices |
|
| |
| Methods | Design: cross-sectional study with control group |
| Participants | 29 participants with CF, recruited from CF outpatient clinics in the UK and Canada |
| Intervention | Participants wore a hip-mounted ActiGraph GT3X+ accelerometer (ActiGraph LLC) for 7 consecutive days and instructed to only remove the monitor for water-based activities ( |
| Outcomes | This study examined body stature and mass, lung function, SED, LPA, MPA, VPA, sleep duration, wake after sleep onset, and sleep efficiency |
| Notes | To be included in the PA analyses, data had to be available for a minimum of 10 h·day−1 of wake wear-time on any 3 days and daily sleep time had to be ≥160 min·night−1 with greater than 90% estimated wear-time |
|
| |
| Methods | Design: RCT of feasibility |
| Participants | 13 participants with CF |
| Intervention | The intervention developed an 8-week family-mediated PA counselling programme called CF Chatters |
| Outcomes | This study examined body stature and mass, lung function, feasibility of intervention, MVPA, and a paediatric QoL questionnaire |
| Notes | A 6 min·day−1 increase in MVPA was observed in the intervention group, from baseline to week 12 |
|
| |
| Methods | Design: cross-sectional study with control group |
| Participants | 30 participants with CF were diagnosed by an abnormal sweat test and either typical pulmonary or digestive symptoms or a positive family history |
| Intervention | Participants completed Kriska's Modifiable Activity Questionnaire |
| Outcomes | This study examined body stature and mass, lung function, PA, cardiorespiratory fitness |
| Notes | Relatively healthy children with CF engage in less vigorous PAs than their healthy, non-CF counterparts, despite having good lung function and nutritional status |
|
| |
| Methods | Design: cross-sectional design |
| Participants | 22 participants with CF (10 men, 12 women) |
| Intervention | Participants completed the Habitual Activity Estimation Scale, the Multidimensional Fatigue Inventory–20 and the Hospital Anxiety and Depression Scale |
| Outcomes | This study examined body stature and mass, lung function, PA estimation and fatigue domains |
| Notes | The authors reported higher level of PA is associated with a lower level of general and physical fatigue when controlling for lung function and level of depression |
|
| |
| Methods | Design: cross-sectional |
| Participants | 78 participants with CF |
| Intervention | A 2-month exercise regimen consisting of activities chosen by the participant designed with a clinic physical therapist |
| Outcomes | This study examined body stature and mass, lung function, exercise capacity (6MWT), habitual activity estimation scale, and the revised CF QoL questionnaire |
| Notes | The authors reported that girls recorded lower habitual activity and had poorer lung function than boys and that 68% of girls completing the study did not improve exercise capacity over a 2-month period |
|
| |
| Methods | Design: cross-sectional |
| Participants | 40 participants with CF |
| Intervention | Patients and families were invited to participate |
| Outcomes | This study examined feasibility, uptake rate (the percentage of patients with CF who agreed to participate, out of the total number of patients invited) and completion rate (the percentage of participants who successfully completed the ACT survey, PA survey and fitness test, out of the total number who consented to participate) |
| Notes | Completion rate for the fitness test was 55%, due to time constraints |
|
| |
| Methods | Design: prospective observational multiple cohort study |
| Participants | 52 participants with CF |
| Intervention | All treatments, including IVA, were managed by the subjects’ pulmonologists |
| Outcomes | This study examined areal BMD, body composition, volumetric BMD, bone microarchitecture and bone strength |
| Notes | Cortical volume, area and porosity at the radius and tibia increased significantly in adults in the IVA cohort |
|
| |
| Methods | Design: cross-sectional |
| Participants | 30 participants with CF |
| Intervention | Participants were requested to wear the pedometer during all waking hours for a total of 21 days, which comprised two “well” periods, each of 7 days duration and one “ill” period of 7 days |
| Outcomes | This study examined an adherence rate of using pedometer, step count, step rate, CF Respiratory Symptom Diary and lung function |
| Notes | This study reported that pedometer-recorded step rate correlated with self-reported PA items on the CF Respiratory Symptom Diary |
|
| |
| Methods | Design: cross-sectional |
| Participants | 103 participants with CF |
| Intervention | Add at least 3 h·week−1 of VPA to their baseline activity including at least 30 min·week−1 of strength-building exercises and 2 h·week−1 of aerobic exercise |
| Outcomes | This study examined CPET, pulmonary function, oral glucose tolerance test and PA |
| Notes | This study analysed baseline data from the ACTIVATE-CF trial, an international multi-centre RCT conducted between June 2014 and March 2016 |
|
| |
| Methods | Design: cross-sectional |
| Participants | 41 participants with CF |
| Intervention | A regular clinical visit and wore an accelerometer for 7 consecutive days |
| Outcomes | This study examined lung function, activity behaviour, accelerometry, questionnaires (the Habitual Activity Estimation Scale, the 7-day PA recall questionnaire and the Lipid Research Clinics questionnaire) and aerobic fitness |
| Notes | The 7-day PA recall questionnaire score (0.41<r<0.56) and “active” score (r=0.33) of the HAES correlated significantly with MVPA |
|
| |
| Methods | Design: cross-sectional with healthy control group |
| Participants | 20 participants with CF |
| Intervention | Patients and healthy controls wore an accelerometer to assess daily habitual PA and they were studied over 5 consecutive typical days (including 2 weekdays and 2 weekend days). |
| Outcomes | This study examined pulmonary function, 6MWT, CPET and HAES questionnaire |
| Notes | None of PA categories estimated by HAES questionnaire correlated with PA categories measured by an accelerometer |
|
| |
| Methods | Design: cross-sectional |
| Participants | 60 participants with CF |
| Intervention | Patients wore a multi-sensor armband for at least 5 full consecutive days |
| Outcomes | This study examined pulmonary function, PA and body composition |
| Notes | PA at moderate intensity (4.8–7.2 METs) or greater (>7.2 METs) was independently associated with gender and FEV1 % pred (p=0.007 and p=0.04, respectively) |
|
| |
| Methods | Design: observational, single-centre, pilot study |
| Participants | 24 participants with CF |
| Intervention | Static task was supine lying and active tasks comprised stair-climbing, stationary cycling and walking (modified 6MWT) Participants undertook stair-climbing in an indoor stairwell (24 steps) and were instructed to descend and ascend the stairs as they would in everyday life |
| Outcomes | This study examined lung function, BMI and PA |
| Notes | Participants were allocated into one of four arms according to their device (Smartwatch, Fitbit, Android smartphones and iOS smartphones) |
|
| |
| Methods | Design: prospective case–control study |
| Participants | 30 participants with CF |
| Intervention | Patients and controls wore an accelerometer to assess daily habitual PA over 5 consecutive days of their normal activities |
| Outcomes | This study examined an incremental CPET on a cycle ergometer, using the accelerometer to assessed PA |
| Notes | MPA (>4.8 METs) and MVPA (>7.2 METs) was related to |
|
| |
| Methods | Design: cross-sectional with control group |
| Participants | 34 participants with CF |
| Intervention | Used a PA monitor to assess habitual physical activities for a period of 5 days |
| Outcomes | This study examined CPET ( |
| Notes | 70% of patients responded to CPET with dynamic hyperinflation |
|
| |
| Methods | Design: case study |
| Participants | Three participants with CF |
| Intervention | The combination of the corrector LUM with the potentiator IVA |
| Outcomes | This study examined CPET and PA |
| Notes | This study performed incremental CPET and assessed PA pre- and post-2 years initiation of LUM–IVA |
|
| |
| Methods | Design: longitudinal (period of 2 years) |
| Participants | 109 patients: girls (n=56) and boys (n=53) |
| Intervention | Data were scheduled for collection for all study patients at each quarterly clinic visit over the 2-year period |
| Outcomes | Anthropometric measures, pulmonary function testing, HAES questionnaire, activity diary and aerobic cycle ergometer test |
| Notes | This study used the HAES questionnaire for a typical weekday (Tuesday, Wednesday or Thursday) and one weekend day (Saturday) to assess PA |
|
| |
| Methods | Design: cross-sectional analysis comparing the dietary intake, PA, and DXA body composition measures in adolescents and adults with CF and age-, race- and gender-matched healthy volunteers |
| Participants | 38 participants with CF (mean± |
| Intervention | A cross-sectional analysis comparing the dietary intake, PA and DXA body composition measures in adolescents and adults with CF and age-, race- and gender-matched healthy volunteers |
| Outcomes | Dietary intake, PA (using the Modifiable Activity Questionnaire), DXA body composition measures and pulmonary status (FEV1) |
| Notes | Participants were recruited from a single centre |
|
| |
| Methods | Design: RCT |
| Participants | 66 children participated in the study |
| Intervention | Compared groups performing aerobic and resistance training with a control group of children with CF admitted to hospital with an intercurrent pulmonary exacerbation |
| Outcomes | FEV1, FVC, |
| Notes | Four children initially consented, but were excluded prior to randomisation due to patient and/or parental concerns about the possibility to being randomised into the control group |
|
| |
| Methods | Design: cross-sectional study |
| Participants | A total of 148 children (75 girls and 73 boys) with CF and matched controls |
| Intervention | The control group was matched for age (±6 months), gender and Tanner pubertal stage, and consisted of healthy children from surrounding schools |
| Outcomes | Activity levels (using an activity diary), nutrition, pancreatic function, measure of fitness (aerobic capacity, anaerobic power, and activity counts) and quality of well-being score |
| Notes | A total of 159 children with CF agreed to participate in the study, but 11 were excluded on the basis of a recent pulmonary exacerbation |
|
| |
| Methods | Design: cross-sectional |
| Participants | CF group (n=31) mean± |
| Intervention | Compared PA between people with CF and non-CF peers and examined associations between PA, vascular function and health outcome measure |
| Outcomes | QoL (CFQ-R), PA (variables assessed using accelerometery, PA questionnaire and vascular function (flow-mediated dilatation)) |
| Notes | The novel PA assessment methods used in the current research may have limited clinical application owing to the cost of accelerometers and the level of expertise and time required for data analysis |
|
| |
| Methods | Design: cross-sectional |
| Participants | Control: n=11, mean± |
| Intervention | Fasting labs and an oral glucose tolerance test were performed |
| Outcomes | Continuous glucose monitoring, actigraphy, fasting labs and oral glucose tolerance test |
| Notes | The participants with CF in this study had relatively good lung function (FVC and FEV1) |
|
| |
| Methods | Design: validation study |
| Participants | 167 subjects aged 7–18 years with a diagnosis of either JA, JDM, moderate or severe HE A or B (up to 5% clotting factor), muscular dystrophinopathies (Becker, Duchenne or other IMD), CF or CHD who had undergone a heart repair (Fontan repair or Tetralogy of Fallot repair) and 29 healthy children |
| Intervention | Each 2-h ET session consisted of anthropometric measures, pulmonary function testing and three EE protocols: resting EE, activities of daily living and exercise |
| Outcomes | Indirect calorimetry, accelerometery and questionnaire |
| Notes | This study used both the Actical (Philips Respironics, Murrysville, PA) and Actigraph 7164 (ActiGraph, Pensacola, FL) accelerometers |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 50 patients (23 males and 27 females) |
| Intervention | TB, femoral neck and LS BMD were determined by DEXA and bone metabolism markers alkaline phosphatase, pro-collagen type 1 N-terminal pro-peptide, PICP and β-CrossLaps |
| Outcomes | Exercise tolerance and daily PA parameters and nutritional parameters |
| Notes | This study used the SenseWear armband to measure PA |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 50 CF patients ≥16 years, male sex (n=23) and female sex (n=27) |
| Intervention | PA was quantified with a portable motion monitor |
| Outcomes | Daily PA monitoring (using a portable monitor), maximal CPET (performed on a cycle ergometer), 6MWT, BMD and radiologic evaluation of the vertebral column |
| Notes | “To our knowledge, no previous study has analysed the level of PA of patients with CF in real time” |
|
| |
| Methods | Design: prospective cohort observational study |
| Participants | 35 participants were recruited for the study, out of which 27 completed the 1-year follow-up visit |
| Intervention | Assessment of PA was done in which subjects were provided with a pedometer that they were asked to wear for 3 consecutive days quarterly for 1 year |
| Outcomes | Mobility was assessed monthly by the Life-Space Assessment questionnaire and quarterly by a pedometer |
| Notes | One limitation of this study was the small sample size |
| Methods | Design: cross-sectional study |
| Participants | Nine participants with CF |
| Intervention | An 8-week video-call exercise intervention supervised three times per week by an exercise therapist |
| Outcomes | This study examined body stature and mass, lung function, LPA, MPA, VPA, SED, CF QoL questionnaire score and feasibility (demand, acceptability and implementation) |
| Notes | The authors noted the potential for reducing the time normally required between meeting patients in the same facility due to cross-infection risks and viewed this as an efficient use of clinical time, increasing the practical feasibility of using Skype for exercise delivery |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 64 participants with CF |
| Intervention | Measurement of PA over 5 full days using accelerometry and measurement of |
| Outcomes | This study examined body stature and mass, lung function, maximal pulmonary pressure, handgrip and quadriceps force, inspiratory and expiratory pressure, MPA, VPA, steps·day–1, and 6MWD |
| Notes | There was only a modest correlation between patients’ PA and fitness, which once adjusted for other covariates, |
|
| |
| Methods | Design: cross-sectional study |
| Participants | 44 participants with CF |
| Intervention | A sports participation survey, which was obtained from questions asking for the PA/sports practised |
| Outcomes | This study examined body stature and mass, lung function, type of sports participation, SED, LPA, MPA and VPA |
| Notes | CF patients did not differ in any level of PA or SED compared to their healthy control group |
|
| |
| Methods | Design: prospective pre–post-intervention |
| Participants | 39 participants with CF |
| Intervention | A 3-week residential rehabilitation on nutritional status for patients with CF |
| Outcomes | This study examined physical stature and mass, presence of malnutrition, DEXA bone status (bone mineral content, fat mass, FFM), pulmonary function and PA through SenseWear (estimated total EE, steps, estimated METs and time >3 METs) |
| Notes | The authors noted that the SenseWear Pro3 armband and its measured caloric expenditure could not be used to tailor the actual energy intake for patients with CF |
|
| |
| Methods | Design: cross-sectional with age- and sex-matched control group |
| Participants | Six participants with CF (part of a study across multiple groups with different chronic diseases, |
| Intervention | PA was measured using activity monitors but with a focus on assessing SED over 7 consecutive days |
| Outcomes | This study examined SED in h·day−1, min·h−1 and % of wear time, also classifications of hours spent watching television, computer and video games |
| Notes | This study found that there was not a significant difference in SED (min·h−1 or % wear time) between the control group or when compared to other disease conditions |
|
| |
| Methods | Design: prospective observational design |
| Participants | 24 participants with CF |
| Intervention | The SenseWear® Pro3 armband measured PA between days 3 and 5 of hospitalisation and again 1 month after hospital discharge |
| Outcomes | The primary outcome was the time spent performing PA over a 24-h period represented as total EE (kilocalories), total PA duration, time lying down and sleep duration, and time spent in sedentary/moderate/vigorous/very vigorous activity based on the MET values |
| Notes | Whilst 24 completed the study, 36 were recruited with 12 failing to complete the study including three who did not tolerate the armband |
|
| |
| Methods | Design: prospective observational study |
| Participants | Participants with CF recruited at admission for acute acerbation and 25 patients with CF attending routine follow-up clinics and a named stable cohort recruited as a comparison |
| Intervention | Within 48 h of admission, participants had lung function and body composition collected, an isometric strength quadriceps test, blood tests, respiratory muscle strength |
| Outcomes | This study examined FEV1/FVC, FFM, BMI, quadriceps maximal voluntary contraction, blood markers; CRP, albumin, full blood count, |
| Notes | This study used a novel, ultra-lightweight (5.6×3.5×1.0 cm, 7.4 g), activity recognition sensor device (e-AR), worn discreetly behind the ear to measure PA |
|
| |
| Methods | Design: prospective observational study |
| Participants | 14 participants with CF |
| Intervention | This study compared the habitual PA scores (HAES questionnaire) to an accelerometer activity monitor and an activity diary in adolescent and adult patients with CF |
| Outcomes | This study examined activity time at different intensities (inactive, somewhat inactive, somewhat active, active) in hours and at various times of day |
| Notes | This study reported that the HAES is clinically feasible due to its ease of administration and high compliance/completion compared to pedometers and accelerometers |
|
| |
| Methods | Design: pre-experimental one-group pre-test–post-test interventional study |
| Participants | 26 participants with CF |
| Intervention | The subjects participated in an individual training programme in collaboration with a sport and exercise scientist |
| Outcomes | This study examined anthropometry, lung function and physical fitness |
| Notes | This study was registered on ClinicalTrials.gov ( |
| Study, year | Theoretical or conceptual underpinning to the research | Statement of research aim(s) | Clear description of research setting and target population | Study design is appropriate to address the stated research aim(s) | Appropriate sample to address the research aim(s) | Rationale for choice of data collection tool(s) | Format and content of data collection tool is appropriate to address the stated research aim(s) | Description of data collection procedure | Recruitment data provided | Justification for analytic method selected | Method of analysis appropriate to answer the research aim(s) | Evidence that the research stakeholders have been considered in research design or conduct | Strengths and limitations critically discussed | Final rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| 3 | 3 | 3 | 3 | 2 | 2 | 2 | 2 | 3 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | 0 | 0 | No/minor concerns |
|
| 2 | 2 | 3 | 3 | 2 | 2 | 2 | 3 | 3 | 3 | 2 | 0 | 0 | Moderate concern |
|
| 2 | 2 | 3 | 3 | 2 | 2 | 2 | 3 | 3 | 3 | 2 | 0 | 0 | Moderate concern |
|
| 3 | 3 | 3 | 2 | 2 | 3 | 3 | 2 | 1 | 3 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 2 | 3 | 3 | 2 | 1 | 1 | 2 | 1 | 2 | No/minor concerns |
|
| 2 | 2 | 3 | 3 | 2 | 2 | 3 | 2 | 2 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 2 | 0 | 1 | 0 | 1 | 2 | 2 | 1 | 0 | 1 | 1 | 3 | 0 | Moderate concern |
|
| 2 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 2 | No/minor concerns |
|
| 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 0 | No/minor concerns |
|
| 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 2 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 3 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 3 | 2 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 1 | 2 | 0 | 0 | No/minor concerns |
|
| 3 | 3 | 3 | 3 | 2 | 2 | 3 | 2 | 2 | 2 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 2 | 2 | 2 | 2 | 3 | 2 | 3 | 2 | 2 | No/minor concerns |
|
| 3 | 3 | 3 | 2 | 0 | 2 | 3 | 1 | 1 | 1 | 0 | 0 | 1 | Moderate concern |
|
| 2 | 0 | 2 | 3 | 2 | 2 | 0 | 1 | 0 | 2 | 0 | 0 | 0 | Serious concerns |
| 3 | 2 | 2 | 3 | 0 | 2 | 3 | 3 | 0 | 2 | 3 | 0 | 2 | Moderate concern | |
|
| 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 0 | 3 | 2 | 2 | 0 | 0 | 2 | 1 | 1 | 2 | 3 | 2 | Moderate concern |
|
| 3 | 0 | 1 | 2 | 0 | 2 | 2 | 1 | 1 | 1 | 2 | 3 | 3 | Serious concern |
|
| 1 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 0 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 1 | 2 | 3 | 0 | 1 | No/minor concerns |
|
| 1 | 3 | 2 | 2 | 2 | 3 | 3 | 2 | 2 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 1 | 2 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | No/minor concerns |
|
| 3 | 3 | 3 | 2 | 2 | 2 | 2 | 3 | 3 | 2 | 2 | 0 | 3 | Moderate concern |
|
| 1 | 1 | 3 | 2 | 2 | 2 | 3 | 3 | 2 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 2 | 2 | 3 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 1 | Moderate concern |
|
| 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 1 | 3 | 3 | 0 | 0 | No/minor concerns |
|
| 3 | 3 | 2 | 2 | 2 | 2 | 2 | 3 | 1 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 1 | 2 | 3 | 3 | 3 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 3 | 3 | 3 | 2 | 0 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 2 | 3 | 2 | 2 | 2 | 2 | 1 | 2 | 3 | 0 | 1 | Moderate concern |
|
| 1 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 1 | 3 | 1 | 3 | 3 | 3 | 0 | 2 | 3 | 0 | 2 | Moderate concern |
|
| 1 | 3 | 2 | 3 | 3 | 3 | 2 | 2 | 3 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 1 | 3 | 3 | 3 | 2 | 2 | 2 | 3 | 2 | 2 | 2 | 0 | 1 | Moderate concern |
|
| 2 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 2 | 2 | 3 | 0 | 0 | Moderate concern |
|
| 1 | 3 | 2 | 2 | 2 | 2 | 3 | 2 | 1 | 1 | 1 | 0 | 2 | No/minor concerns |
|
| 1 | 3 | 3 | 1 | 3 | 3 | 3 | 3 | 1 | 1 | 1 | 0 | 1 | Moderate concern |
|
| 1 | 3 | 2 | 3 | 2 | 2 | 3 | 2 | 1 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 1 | 2 | 2 | 3 | 2 | 1 | 2 | 3 | 1 | 1 | 2 | 0 | 1 | Moderate concern |
|
| 2 | 3 | 2 | 3 | 2 | 3 | 3 | 2 | 2 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 3 | 3 | 2 | 3 | 2 | 2 | 3 | 2 | 1 | 1 | 2 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 1 | 3 | 2 | 3 | 3 | 2 | 1 | 3 | 3 | 0 | 1 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 1 | 2 | No/minor concerns |
|
| 1 | 3 | 2 | 3 | 1 | 2 | 2 | 3 | 2 | 2 | 2 | 0 | 2 | Moderate concern |
|
| 2 | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | 0 | 3 | No/minor concerns |
|
| 1 | 3 | 3 | 2 | 1 | 3 | 3 | 2 | 0 | 2 | 1 | 0 | 0 | Moderate concern |
|
| 0 | 3 | 2 | 2 | 3 | 3 | 3 | 3 | 1 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 3 | 2 | 2 | 2 | 3 | 3 | 1 | 2 | 2 | 0 | 2 | Moderate concern |
|
| 1 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 1 | 2 | 0 | 0 | Moderate concern |
|
| 1 | 3 | 3 | 3 | 1 | 3 | 3 | 2 | 0 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 1 | 3 | 3 | 2 | 0 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 2 | 1 | 2 | 2 | 1 | 3 | 3 | 3 | 0 | 1 | 1 | 0 | 2 | Moderate concern |
|
| 2 | 3 | 2 | 3 | 2 | 3 | 3 | 2 | 0 | 3 | 3 | 0 | 1 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 3 | 2 | 1 | 3 | 3 | 3 | 2 | 1 | 2 | 0 | 0 | No/minor concerns |
|
| 3 | 3 | 2 | 3 | 2 | 3 | 2 | 2 | 1 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 3 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 3 | 3 | 1 | 3 | 2 | 3 | 3 | 2 | 2 | No/minor concerns |
|
| 0 | 3 | 3 | 3 | 1 | 3 | 3 | 3 | 1 | 3 | 2 | 0 | 3 | No/minor concerns |
|
| 1 | 3 | 2 | 3 | 1 | 1 | 3 | 2 | 2 | 1 | 2 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 3 | 0 | 3 | No/minor concerns |
|
| 0 | 3 | 3 | 2 | 2 | 3 | 3 | 3 | 0 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 1 | 3 | 3 | 3 | 1 | 2 | 2 | 2 | 0 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 2 | 3 | 2 | 3 | 3 | 2 | 0 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 0 | 3 | 3 | 3 | 2 | 3 | 2 | 3 | 0 | 2 | 3 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 3 | 3 | 3 | 3 | 2 | 3 | 0 | 2 | 3 | 0 | 1 | No/minor concerns |
|
| 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 1 | 3 | 3 | 3 | 2 | 3 | 2 | 3 | 2 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 0 | 3 | 1 | 3 | 0 | 3 | 3 | 3 | 0 | 2 | 3 | 0 | 1 | No/minor concerns |
|
| 0 | 3 | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 2 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 3 | 3 | 3 | 3 | 2 | 1 | 2 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 1 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 1 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 1 | 3 | 3 | 3 | 1 | 2 | 3 | 3 | 3 | 2 | 3 | 0 | 3 | No/minor concerns |
|
| 2 | 3 | 3 | 2 | 1 | 3 | 3 | 3 | 2 | 2 | 2 | 0 | 3 | No/minor concerns |
|
| 3 | 3 | 2 | 2 | 3 | 3 | 3 | 2 | 1 | 3 | 3 | 0 | 2 | No/minor concerns |
|
| 1 | 2 | 2 | 2 | 2 | 3 | 3 | 2 | 0 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 3 | 3 | 2 | 2 | 1 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 2 | 3 | 2 | 2 | 1 | 1 | 2 | 0 | 1 | Moderate concern |
|
| 2 | 3 | 2 | 3 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 1 | 1 | Moderate concern |
|
| 1 | 3 | 2 | 3 | 2 | 3 | 2 | 3 | 1 | 3 | 2 | 0 | 2 | No/minor concerns |
|
| 2 | 3 | 2 | 3 | 2 | 3 | 3 | 3 | 1 | 2 | 2 | 0 | 1 | No/minor concerns |
|
| 1 | 2 | 1 | 3 | 2 | 2 | 3 | 3 | 1 | 2 | 3 | 1 | 1 | No/minor concerns |
|
| 1 | 3 | 2 | 3 | 0 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | Moderate concerns |
|
| 2 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 3 | 2 | 2 | 0 | 2 | No/minor concerns |
|
| 1 | 1 | 0 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 1 | 0 | 2 | Serious concerns |
|
| 0 | 2 | 0 | 0 | 2 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 3 | No/minor concerns |
| 0 | 0 | 0 | 0 | 3 | 1 | 0 | 1 | 3 | 2 | 1 | 3 | 1 | Moderate concern |
| Research question | Considerations | Setting |
|---|---|---|
|
| Clinical practice may benefit from the use of more affordable and easy-to-use devices, such as pedometers, smartwatches, diaries and questionnaires, depending on the expertise and resources available | Clinical practice |
|
| As stated in the 2015 position statement [ | Research |
|
| It is recommended that time spent in different physical activity intensities, being sedentary and asleep should be reported when using device-based monitors | Clinical practice and research |
|
| Despite substantial evidence published since the 2015 statement, including data from healthy populations and in people with CF, it remains clear that higher physical activity levels and reduced sedentary time are beneficial | Clinical practice and research |
|
| Research into physical activity and sedentary time is increasingly utilising raw data to enable more complex analyses, such as machine learning and compositional analysis | Clinical practice and research |
|
| We recommend that data resolution for physical activity analysis should be at least 1 s (minimum 30 Hz) to enable clinical teams to obtain a representative account of patients’ physical activity patterns | Clinical practice |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Asthma and respiratory diseases · Mobile Health and mHealth Applications
Introduction
In 2015, Bradley et al. [1], supported by the European Cystic Fibrosis Society (ECFS), published a position statement to inform the choice of physical activity assessment/measurement tools for cystic fibrosis (CF) research and clinical settings. Two physical activity monitors (SenseWear and ActiGraph) were endorsed for measuring energy expenditure (EE), step count, activity intensity and sedentary time [1]. The DigiWalker pedometer was noted as a low-cost alternative for assessing some physical activity components. Although several questionnaires were mentioned in the statement, only the Habitual Activity Estimation Scale (HAES) [2] was supported. Bradley et al. [1] concluded that “Future research should focus on providing additional evidence of clinimetric properties of these and new physical activity assessment tools, as well as further exploring the added value of physical activity assessment in CF”.
Since the 2015 position statement [1], research into physical activity measurement and interpretation of physical activity has increased substantially. Device-based assessment has advanced to include watch-worn, phone-based and clothing-embedded sensors, offering much higher data resolution than earlier tools [3]. High-resolution capture (≥100 Hz) enables analysis of activity in seconds rather than minutes [4], enhancing insight into the effects of varying intensities on health. Recently, physical activity has been conceptualised over a 24-h period, incorporating sedentary behaviour and sleep [5–7]. This has prompted the use of advanced statistical methods such as isotemporal substitution and compositional analysis [5–7].
In the general population, the type and volume of physical activity have a strong-to-moderate inverse association with morbidity and mortality [8]. In clinical groups, the importance of physical activity, even in those with complex conditions, is being increasingly recognised for physical, mental and social health benefits [9]. However, in CF, physical activity assessment is often not a routine clinical measure; with the transformational care and management of this disease and the latest cystic fibrosis transmembrane conductance regulator modulator drug therapies, the increased functional capability of this population warrants further investigation.
Rationale
The recent advancements, not only in the measurement tools for physical activity but also conceptualisation and analyses, necessitate an update regarding the use of physical activity within CF research and clinical settings. Moreover, the shift towards conceptualising physical activity as a 24-h construct encompassing physical activity categories (light, moderate and vigorous), sedentary and sleep, has enabled a more comprehensive analysis of the role of physical activity in the lives of clinical groups. Indeed, new devices, methods of analysis and interpretation can help to advance the integration of physical activity in the management and care of people with CF (pwCF).
Objectives
Therefore, the aim of this review was to systematically synthesise the literature on the measurement of physical activity, sedentary time and sleep in pwCF and provide guidance to clinicians and researchers.
Review questions
This systematic review sought to address the following research questions:
- 1) Which instruments (i.e. devices/questionnaires/diaries) represent the informed choice for the measurement of physical activity and sleep in clinical practice?
- 2) Which instruments represent the informed choice for the measurement of physical activity and sleep as an outcome measure in research?
- 3) What output(s) should be reported from device-based physical activity and sleep?
- 4) What is an important treatment effect for device-based physical activity and sleep?
- 5) What important consideration(s) should be made when collecting, processing and analysing device-based physical activity and sleep data in clinical practice and research?
- 6) Specifically for device-based measurement of physical activity and sleep, what are the measurement and processing properties/features that should be standard for feasible utility in a clinical setting?
Methods
This review was registered on the International Prospective Register of Systematic Review (PROSPERO) database (CRD42022292165) and conducted according to the Preferred Reporting items for Systematic Review and Meta-Analysis (PRISMA) [10, 11].
Eligibility criteria
Studies investigating the measurement of physical activity, sedentary time and sleep, irrespective of age, setting and monitoring/study duration, were included. Peer-reviewed studies published in English were included independent of their design (e.g., case studies and randomised controlled trials). Non-English-language, nonhuman and unpublished studies, book chapters, theses, dissertations, abstracts and monographs were not included. More specifically, studies investigating the association between the instrument used to measure physical activity with relevant health outcomes, such as lung function, body mass index (BMI) and quality of life, were included. Outcomes of any instrument that measures sedentary time and physical activity, either from devices or calculated from questionnaires (but excluding in-house nonvalidated questionnaires), but not limited to, min·week^−1^ of moderate physical activity, vigorous physical activity or/and sedentary time were reported.
Information sources
A systematic search for published studies was conducted in March 2022 and updated in March 2024 using the Medline, Embase and Cumulative Index to Nursing and Allied Health Literature electronic databases. The reference list of relevant studies was examined for additional studies and experts in the field were contacted for any additional studies.
Search strategy
As advised by the PRISMA checklist [10], a population–intervention–comparison–outcome framework was followed to structure the search strategy and a pilot search was performed to ensure the search strategy would be suitable. Limits and filters were applied to the search strategy for all databases to only include studies with humans that were published in English. As this review is not only updating the former ECFS position statement but expanding it, the year of publication was not restricted. The Medical Subject Headings (MeSH) were adopted to select the search terms, which were inserted as keywords into all three databases. The search terms were:
- 1) Questionnaire* OR accelerometer* OR “motion sensor*” AND cystic fibrosis
- 2) HAES OR IPAQ OR ActiGraph OR GENEActiv OR sensewear OR ActivPAL OR caltrac AND cystic fibrosis
- 3) Physical activity OR habitual activity AND cystic fibrosis
- 4) Sedentary time OR inactivity AND cystic fibrosis
Selection process
The searches were imported into EndNote X9 (Clarivate Analytics, US) and subsequently into Rayyan [12] for screening. Two authors (M.S. Bianchim and C.A. Williams) double-blind screened all titles and abstracts, using Rayyan, according to the inclusion criteria. All discrepancies were resolved by consulting a third author to reach a consensus (J. Shelley, M.A. McNarry or K.A. Mackintosh). Subsequently, all full texts were saved as .pdf files and screened according to the pre-established criteria by the same authors (M.S. Bianchim and C.A. Williams), with a third author consulted if necessary (J. Shelley, M.A. McNarry or K.A. Mackintosh).
Data collection process
A data extraction Excel spreadsheet was developed by two authors (M.S. Bianchim and C.A. Williams) based on preliminary data from the pilot and based on the main outcomes of interest. A total of seven reviewers (J. Shelley, M.A. McNarry, K.A. Mackintosh, T.J. Dwyer, B. Button, E. Hatziagorou and J. Bradley) collected data from each study independently using an online version of the spreadsheet. M.S. Bianchim resolved any disagreements and was responsible for managing the online data extraction spreadsheet making sure all data was extracted correctly. Supplementary information for each study was consulted when available or necessary and authors of the primary studies were consulted to obtain or confirm data.
Data items
The main outcomes included those from instruments measuring physical activity, sedentary time and sleep (e.g., minutes of moderate-to-vigorous physical activity, number of steps and EE (e.g., metabolic equivalent tasks (METs)). Secondarily, additional outcomes included the different types of physical activity measures, along with their associated strengths and weaknesses (e.g., participant compliance and differences between objective measures such as accelerometers and subjective measures such as questionnaires), any variables associated with collection, processing and analysis of physical activity data, and any data regarding the importance of physical activity and sedentary time measurement. Specifically, the following information was extracted from each included study: author, year of the study, sample information and characteristics (e.g., age, size of the sample, BMI, stature, body mass and sex), any other health-related variable (e.g., spirometry and heart rate), types of physical activity, duration and frequency of the protocol or intervention, and any variable related to collecting and processing of device-based physical activity (e.g., epoch, sampling frequency, wear-time criteria and cut-points).
Quality assessment
Each study was assessed independently by two reviewers (M.S. Bianchim, C.A. Williams, J. Shelley, M.A. McNarry, K.A. Mackintosh, T.J. Dwyer, B. Button, E. Hatziagorou or J. Bradley) using the Quality Assessment for Diverse Studies (QuADS) tool [13] and all disagreements were arbitrated by a third reviewer (M.S. Bianchim or C.A. Williams). The QuADS tool is composed of 13 domains and was specifically designed for the appraisal of mixed- or multi-methods studies, with strong inter-rater reliability (k=0.66) and substantial content validity [13]. The instrument was modified to assess the level of methodological concerns rather than the total numeric score [14]. Specifically, studies were rated as “no/minor”, “moderate”, “serious” or “very serious” methodological concerns. Findings from studies identified as serious and very serious concerns were interpreted with caution. Assessments were recorded using Microsoft Excel.
Synthesis methods
A mixed-methods framework synthesis was used to extract, map, chart, categorise and aggregate study findings [15]. An initial framework was developed using the research questions as key domains from which to extract data. Initially, studies had key text of interest highlighted and then extracted into the initial framework (see supplementary file 1). Following the population of the framework with data, mapping and charting were undertaken using the mixed-methods data in its original format. The outcomes of this process were descriptive-level findings and explanations, which were shared and discussed with a wider group of researchers and key stakeholders.
Results
In total, 7065 potentially relevant publications were identified from the three databases, with 6549 remaining after removing duplicates. Following screening of titles and abstracts, 422 full texts were retrieved and assessed for eligibility leading to the exclusion of 332 studies, primarily due to wrong publication type (n=166) (figure 1). This resulted in the inclusion of 90 studies (table 1) with a total of 4021 participants with CF aged between 6.7 and 65.0 years (mean±sd 21.1±17.4 years) and 48.9% were male (n=1968). 51 of the included studies were published after the 2015 position statement. All excluded studies are listed in supplementary file 2. 36 studies were in adults [16–51], 34 in young people [52–84] (27 included children, five children and adolescents, and two adolescents only) and 20 included both young people and adults [85–103]. Only 34 studies included a control group (n=5934) [16, 23, 26, 27, 30, 37, 43–45, 48, 52–54, 57, 59, 61, 62, 66, 68, 70, 72, 74, 75, 79–81, 91, 92, 94, 95, 98–100, 104]. The included studies measured physical activity using accelerometers (n=57) [16–38, 41, 50, 52–56, 58–69, 72, 86–93, 103–107], questionnaires (n=26) [40, 42, 43, 45, 47, 48, 51, 70–77, 79–84, 95, 96, 98–100], both accelerometers and questionnaires (n=11) [21, 26, 53, 54, 56, 60, 72, 87, 88, 92, 103], diaries (n=8) [58, 59, 78, 83, 88, 89, 96, 108], commercial smartwatches (n=5) (Garmin Vivosmart4® and Fitbit® Charge 2) [19, 41, 56, 94, 97], pedometers (n=3) [49, 101, 102] and interviews (n=1) [109].
Flowchart of the study.
There was wide heterogeneity in study designs. The majority of the studies were observational (n=57) [17, 19, 21, 23–28, 30, 32, 35, 37, 38, 40–46, 48–54, 59–63, 66, 68–73, 75, 76, 78, 80, 81, 86, 91, 93, 95–97, 99, 105, 108–111], eight were validation studies [16, 18, 19, 34, 47, 55, 88, 103], eight were intervention studies [31, 65, 77, 84, 85, 90, 94, 98], seven were feasibility/pilots [29, 33, 41, 67, 82, 89, 101], four were longitudinal studies [22, 74, 83, 87], three were randomised controlled trials [58, 79, 92] and two were case studies [56, 64]. Physical activity was the primary outcome investigated in 69 studies, with three studies identifying sleep as the primary variable [44, 46, 57]. 18 studies measured physical activity as the secondary outcome, which investigated factors associated with bone mineral density [48, 76–78, 96, 97, 100], cardiorespiratory fitness and exercise capacity [47, 66, 71, 72, 79, 102], mobility [49], body composition [48, 90, 109], CF-related diabetes (CFRD) [102], and lung function [109].
Methodological strengths and limitations of included studies
Most included studies (71.0%; n=64) had no or minor methodological concerns, whereas 23 (25.5%) and three (3.5%) studies had moderate and serious methodological concerns, respectively (table 2). For most studies, methodological concerns were due to the poor description of recruitment and/or justification of the recruited sample size. Similarly, most studies did not align or rationalise their study to any theoretical or conceptual framework that underpinned the study. However, the most common limitation was the lack of evidence of stakeholders or/and patient and public involvement in the design or conduct of the study.
Methods used to measure physical activity
Accelerometery was the most common method used to measure physical activity (n=57) [16–38, 41, 50, 52–56, 58–69, 72, 86–94, 103–107], with ActiGraph® (n=25) [21, 22, 26, 52–54, 57–59, 61–63, 66, 68, 69, 72, 85, 87, 88, 91–93, 103, 105, 112] and SenseWear® Pro Armband (n=20) [16, 18, 23–25, 27–33, 35–38, 50, 90, 107] being the most frequently used devices. Other accelerometers included ActivPal® (n=4) [19, 20, 41, 64], GENEActiv® (n=4) [56, 69, 89, 93], Actical® (n=1) [55] and Tritrac® (n=1) [60] and one study did not specify the accelerometer brand [67].
Questionnaires were the second most common method (n=35), with the HAES questionnaire (n=10) [30, 51, 73, 77, 79, 83, 84, 88, 103, 113] most frequently used, followed by the 7-day physical activity recall questionnaire [40, 42, 87, 96], the Modifiable Activity Questionnaire [81, 99, 100], a recall questionnaire (did not specify which one) [45, 48, 80], the Physical Activity Questionnaire for Older Children [74, 95], the Self-reported Baeke Questionnaire [43], the Transport Movements Questionnaire [60], the Use Risk Behaviour Survey [70], the International Physical Activity Questionnaire [72], the Adherence to Quantitative Activity Protocol Questionnaire [47], the Lipid Research Clinics questionnaire [103], the GODIN Physical Activity questionnaire [75], a validated habitual activity questionnaire adapted from that described by Hay et al. [2, 76], the Sport Participation Questionnaire [54] and the Sedentary Behaviour Questionnaire [53]. Four studies did not specify which questionnaire they used to measure physical activity [26, 71, 82, 98].
14 studies used other methods, including diaries (n=4) [58, 59, 78, 108], smartwatches (Garmin® and Fitbit®) (n=5) [19, 29, 41, 94, 97], pedometers (Omron HJ-322 U-E, Digi-Walker®) (n=4) [33, 49, 101, 102] and interviews (n=2) [33, 109].
Reporting physical activity measurement
Studies reported physical activity using a variety of units. Most accelerometer- and questionnaire-based studies focused on outcomes such as time spent in different physical activity intensities, METs per day, time spent in sedentary, low, moderate and vigorous physical activity, and sleep time. Minutes per day of moderate-to-vigorous physical activity was most commonly reported (n=24) [17, 23, 26–28, 32, 35, 36, 51, 52, 54, 55, 61–63, 66–69, 72, 86, 93, 103, 114], followed by sedentary time (n=24) [17, 20, 26–28, 30, 32, 51–55, 61–63, 66–69, 72, 89, 93, 105, 114], low physical activity (n=21) [17, 25–28, 30, 32, 51, 52, 54, 55, 61–63, 66, 68, 69, 89, 93, 105, 114], moderate physical activity(n=18) [17, 23, 25–28, 30, 32, 51, 54, 55, 61, 62, 65, 69, 89, 103, 105] and vigorous physical activity (n=19) [17, 26–28, 30, 32, 51, 52, 54, 55, 61, 62, 66, 69, 89, 93, 103, 105, 114]. Studies using pedometers [33, 49, 101, 102] and smart watches reported daily step counts as the main outcomes [19, 29, 41, 94, 112].
Other studies used time to report physical activity, such as time spent in specific EE (n=3) [37, 64, 80], hours spent being physically active (n=10) [33, 74, 76, 77, 81, 87, 92, 95, 97, 115], days spent being physically active (n=3) [40, 70, 71], activity spent in different percentages of time (n=4) [75, 79, 83, 84] and minutes of physical activity per week (n=1) [82]. The second most common unit used to report physical activity was EE as total EE/METs (n=21) [16, 18, 23, 24, 27, 29–32, 35, 38, 42, 45, 48, 50, 60, 78, 90, 96, 108, 116], followed by number of steps (n=16) [19, 22, 23, 25, 29, 30, 41, 49, 50, 64, 90, 94, 97, 101, 102, 105]. Others calculated an index for different categories (e.g., work, leisure and sport) (n=3) [43, 47, 50] or a mean score (n=3) [28, 99, 100], and two studies reported arbitrary categories (n=2) [88, 91].
10 studies measured and reported sleep; the most common unit used was total sleep duration in hours [64, 97] or minutes [27, 36, 44, 57, 68, 69, 93, 105]. Others also measured sleep onset latency (time to fall asleep) [57], wake after sleep onset (min of wake-up time after initial sleep onset) [36, 44, 57, 105], total time in bed [105] and sleep efficiency (percentage of time asleep out of total time in bed) [57, 105].
Collecting and processing device-based physical activity data
Most accelerometers were tri-axial (n=27) [16–21, 26, 52–54, 56, 60–66, 68, 69, 72, 89, 90, 93, 94, 104, 105], followed by bi-axial (n=15) [23–25, 27–31, 33–38, 55] and uni-axial (n=9) [49, 53, 58, 59, 86–88, 91, 103]. Devices were most commonly worn on the arm (n=20) [16–18, 23–25, 27–30, 32–38, 50, 90, 105] (two on the left side, five on the right side and seven nonspecified), followed by the waist (n=17) [21, 52–55, 60–63, 66, 68, 87, 88, 91, 97, 103, 104] (10 on the right side, one on the left side and two nonspecified), wrist (n=8) [26, 56, 57, 69, 89, 93, 94, 105], with six not specifying whether it was nondominant wrist, and mid-thigh (specifically to measure sedentary time) (n=3) [19, 20, 64]; six studies did not specify the placement [22, 59, 66, 67, 92, 108].
Regarding accelerometer data-processing, most studies used cut-points (n=15) [52–54, 56, 61, 62, 67–69, 86, 87, 89, 91, 93, 103], including Esliger et al. [117], Philips et al. [118], Freedson et al. [119], Evenson et al. [120] and Hildebrand et al. [121, 122], and arbitrarily absolute intensity cut-points (e.g. >1000 counts·min^−1^ used time spent in determined EE and MET thresholds to identify different physical activity intensities (>4.8 METS at least moderate-intensity; moderate-intensity activity >3 METs) [19, 20, 26, 54, 56, 61, 62, 68, 69, 93]. Only three studies used raw metrics such as Euclidean norm minus one and mean amplitude deviation to analyse their data [69, 93, 123].
The most common accelerometer wear duration was 7 days (n=22) [20, 23, 26, 29, 36, 50, 53–58, 61, 62, 64, 68, 69, 85, 89, 90, 93, 103], although this ranged from 1 day (n=2) [17, 60] to 1 year [94] (i.e. 3 days (n=1) [33], 4 days (n=3) [30, 52, 67], 5 days (n=9) [24, 25, 27, 28, 31, 32, 63, 86, 87], between 5 and 7 days (n=2) [35, 38], 9 days (n=1) [91], 12 days (n=1) [59], 14 days (n=1) [88], 28 days (n=2) [22, 65, 66, 105], up to 40 days (n=1) [37], and 12 weeks (n=1) [92]). Most studies instructed continuous wear, removing devices only for water-based activities [23, 27–29, 32, 54, 61, 62, 67–69, 88, 93, 124]. Wear-time inclusion criteria varied, with many requiring ≥3 days of ≥9–10 h·day^−1^ [33, 35, 52–54, 62, 69, 86, 89, 91, 93, 103, 104]. Some studies also specified whether measurement should include weekdays and weekends (n=10) [19, 25, 28, 31, 35, 53, 62, 69, 93, 104].
Four studies used accelerometers during structured protocols [16, 18, 19, 34], although approaches varied. Protocols included treadmill or self-paced walking [16, 19], structured physical tasks (e.g., sitting, standing, cycling and stair-climbing) [34] and lifestyle-type activities (i.e., walking on flat surfaces, walking on incline, sit-to-stand and lift-bend tests), followed by a sub-maximal steady-state cycling test [18].
Health outcomes
Most studies also measured health outcomes, with lung function measured via spirometry being the most common. Specifically, 72 studies reported forced expiratory volume in 1 s (FEV_1_) (% predicted) [16–20, 22–30, 33, 35–38, 41–47, 49–51, 53, 57–63, 66–69, 71, 72, 74, 76, 77, 79, 81, 83–93, 95–97, 99–103, 105, 107, 114, 115], 24 reported FEV_1_ in litres [17, 18, 22, 26, 27, 30, 32, 35–37, 42, 43, 47, 50, 63, 69, 72, 75, 78, 89, 92, 93, 97, 105], 45 studies reported forced vital capacity (FVC) (% predicted) [16, 18–20, 22–30, 41, 43, 44, 46, 47, 50, 51, 57, 58, 60–63, 65, 68, 69, 72, 74, 75, 77, 85, 86, 88–90, 92, 93, 97, 102, 103, 105, 115] and five reported the FEV_1_/FVC ratio [22, 27, 28, 43, 47, 63, 72, 94]. Commonly reported demographic outcomes included CFRD (30 studies) [22, 24, 26, 27, 29, 32, 33, 35–37, 42, 47, 57, 62, 69, 71–74, 91–93, 95, 96, 98–100, 102, 105, 107, 125] and pancreatic insufficiency (25 studies) [22, 25, 27–29, 32–34, 36, 37, 42, 47, 63, 72–74, 78, 83, 91, 94, 95, 97, 99, 104, 105, 126]. Finally, included studies also measured maximum exercise capacity (24 studies) [18, 23, 25, 27, 28, 30, 31, 43, 47, 52, 58, 59, 71, 72, 77, 79, 81, 83, 85–88, 103, 115] and heart rate (seven studies) [18, 22, 47, 63, 72, 77, 94].
Discussion
This review investigated the measurement of physical activity, sedentary time and sleep in children and adults with CF, including 90 studies, with 9955 participants, 4021 of whom had CF. While research on physical activity in CF has grown since 2015 (i.e., 51 publications since), high heterogeneity amongst studies was observed. Most studies focused on the association between physical activity and lung function, such as FEV_1_ (% pred), but there were very few longitudinal studies monitoring these health outcomes. The increasing recognition of the importance of sleep has resulted in seven studies examining this in pwCF. While most included studies were assessed as no/minor methodological concerns, none included stakeholders in the research design or conduct. Future research should consider including patient and public involvement to ensure the needs and priorities of pwCF are being addressed [127–129]. We have established key considerations for clinical practice and research based on review findings and expertise from the research team (table 3).
Research question (RQ) 1: instruments (i.e. devices, questionnaires and diaries) for measuring physical activity and sleep in clinical practice
The choice of physical activity measurement depends on its clinical purpose. Since 2015, the cost of accelerometers, smart watches and phone apps have significantly decreased making their use more popular. This can be observed in accelerometers being the most common choice of device in research, but their use in clinical practice is limited. Other devices such as smartwatches and phone apps have made measuring physical activity more accessible but remain unadopted as part of the clinical care and management of CF. Further clinical validation of the physical activity metrics related to pwCF and their movement behaviours are still required. For example, few devices calibrate the movement behaviours in line with the disease-specific physiological consequences of CF [130, 131]. The increasing interest in the 24-h movement behaviours with information on sleep and sedentary behaviour is a new and emerging field, which has an important role to contribute to the health and well-being of pwCF. Device-based monitors are well placed to fill this gap. However, a technological skills gap exists in data analysis, which hinders ease of use in clinical settings. More work is needed to make physical activity data more user-friendly [132]. While device-based monitors have evolved, questionnaires like the HAES and 7-day recall remain valid methods for assessing activity perception. Combining these methods with devices can provide a detailed picture of physical activity. However, recommending a device-based monitor is challenging due to regulatory requirements, although some devices (e.g., ActiGraph®, GENEActiv® and Garmin®) have met regulations in North America and the EU. While most algorithms for these devices are validated in healthy populations, there are some physical activity thresholds for CF available for ActiGraph and GENEActiv.
RQ 2: instruments for measuring physical activity and sleep as an outcome measure in research
The choice of measurement should align with the research purpose and method, with properties such as calibration, validity, reliability and feasibility being critical to both clinicians and researchers. Whilst questionnaires are useful to estimate physical activity and help with a discussion about what types of physical activity are undertaken, device-worn monitors offer more scope to quantify physical activity domains, sedentary time and sleep. In quantifying the patterns, intensities, time and volume of physical activity, device-worn monitors are more likely to unravel the relationships to health status (morbidity and mortality) for pwCF. Therefore, it is recommended that device-worn monitors be promoted to better understand and provide a more comprehensive assessment of physical activity. Currently, models such as ActiGraph®, GENEActiv® and SenseWear® are commonly used in research, though no single device is clearly superior. However, SenseWear®, which uses skin conductance to gauge intensity and may be influenced by CF-related sweat electrolyte abnormalities, is no longer commercially available. Research efforts to standardise operating and reporting procedures in the context of clinical outcomes should be made a priority.
RQ 3: recommended outputs for reporting physical activity and sleep measurements
To assist researchers and clinical teams, descriptions of the measurement, such as the resolution of data capture or wear time, should be explicitly described to enable replication. Devices that also measure step count are recommended for their ease of use and understanding (i.e. total number of steps to be achieved in 1 day). Devices that calculate EE should be used with caution as the algorithms to calculate the EE are based on small sample sizes and lack cross-validation studies in pwCF. Whilst questionnaires remain an excellent source of qualitative data, care must be taken when estimating time or EE.
RQ 4: important treatment effects for physical activity and sleep measurements
There currently is no consensus on what constitutes an important treatment effect for change to occur in pwCF. More information is required on the volume and its components of frequency, intensity and duration to affect a clinically meaningful change. More information on how physical activity responds to periods of stability and exacerbations in relation to health status, the influence of new drug treatments and its relationship to changes in established patient-reported outcomes (i.e., lung function, body composition and quality of life). Despite that, it is important to acknowledge that global guidelines on physical activity and sedentary behaviour are available for children (age 5 years and older), adolescents and adults [133].
RQ 5: important considerations for collecting, data reduction and analysing device-based physical activity and sleep data in clinical practice and research
Key considerations for collecting device-based physical activity data include device type, placement and measurement duration. Smartwatches and pedometers, which offer visual feedback and are easy to use, suit clinical settings, while accelerometers provide more detailed data but require technical expertise [19, 29, 41]. Regarding placement, waist-worn accelerometers have slightly better performance, while wrist-worn devices were shown to increase compliance [132]. In addition, thigh-worn devices have been used to measure sedentary time. It is also relevant to consider whether the device is positioned on the dominant or nondominant side [131]. Length of measurement is relevant as it can affect the availability of data for processing. Considerations regarding the inclusion of both weekend days and weekdays, as well as ensuring at least 9–10 h of data daily, should be made [61, 62, 68, 69, 93].
Few of the included studies using accelerometers provided detailed descriptions of the processing features and type of analysis used. To improve transparency and replicability, it is essential that studies clearly report and justify accelerometer settings and signal processing decisions. For example, studies should specify the sampling frequency and epoch used, whether any filters were applied (e.g., ActiGraph low-frequency filter) and what type of data was used for processing (i.e. count versus raw) [134, 135]. Finally, the data reduction and analysis methods (e.g., cut-point and equations, compositional analyses, or machine learning) should be evidence-based and transparently reported. It is noteworthy that although CF-specific cut-points were developed for young people [130], to date there are still no specific cut-points available for older adults with CF.
RQ 6: measurement and processing features for device-based physical activity measurement and sleep in clinical settings
To be acceptable in a clinical setting, all device-based instruments must meet the relevant national, regional or local regulatory health and safety requirements. In the case of device-worn accelerometers such as those worn on the wrist, hip or leg, the opportunity to calibrate the device is a necessity to ensure reliable and valid results. The presentation of the data is expressed predominantly as minutes per day and this aligns with national or international physical activity guidelines that present achieving a set number of minutes per day or across a week as the norm.
Potential biases in the review process
We documented and justified deviations from our registered protocol. We believe this is the most comprehensive systematic review to date of physical activity in pwCF. Specifically, a lack of standardised protocols reduced the opportunity to synthesise the data objectively. Additionally, given the volume and complexity of data, synthesis was conducted collaboratively by the author team, with methodological frameworks guiding the process.
A limitation of the current data is that most studies have a cross-sectional design while assessing long-term health outcomes relative to physical activity. There are also likely to be large variations in fitness and health status, which are often not reported. This reporting is important because even between patients who have the same disease status, the relationship of physical activity with health can be affected. Future studies should adopt a standardised and function-based assessment of fitness coupled with a device-based assessment of physical activity to examine its interaction with health status. This will help clinical teams to better understand which types of patients respond better to interventions and improve the evidence base for individualising physical fitness and activity interventions [136].
Practical applications
Currently, there are no international or national guidelines outlined for physical activity and exercise prescription in CF. The usual recommendation is for pwCF to follow their national guidelines for healthy children, young people and adults. Clinical teams are encouraged to develop service pathways to embed exercise and physical activity habits into practice. By embedding this pathway into healthcare infrastructures, it increases the chances that better health and health behaviours will track from childhood and adolescence into adulthood, thus reducing hospital admissions, future morbidity and contributing to increasing survival rates.
Future research
This review highlights a marked rise in physical activity research in pwCF since 2015, reflecting growing interest in its role as a health indicator. However, variation in assessment methods, data processing and analysis limits the clarity of its long-term prognostic and rehabilitation value. An international, large-scale prospective study is needed to assess outcomes such as mortality, morbidity, cost-effectiveness and quality of life. Future interventions should explore the prognostic potential of physical activity to support its integration into both clinical care and daily life.
Conclusion
This review highlights the rapid growth in physical activity research in pwCF since 2015, particularly through device-based assessments. Despite these advancements, most devices are used in research settings due to the time and expertise required for data analysis and the limited evidence linking physical activity metrics to long-term clinical outcomes. Standardisation in data collection and processing remains a key challenge, especially for populations with complex health needs. Where feasible, raw-data-sampling devices (e.g., ActiGraph, GENEActiv) worn for ≥7 days at ≥30 Hz are recommended; otherwise, validated self-report tools such as the HAES can offer practical alternatives. Clinical teams have a critical role in promoting physical activity, reducing sedentary time and supporting sleep. By continuing to work together, researchers, clinicians and their support teams can help advance the cause in understanding the role of physical activity and health in the lives of pwCF.
Questions for future research
- Improving tools for clinical use
- How can more affordable and user-friendly tools (e.g., devices or questionnaires) be adapted for clinical use in CF and other specific populations?
- Better outcome measures
- What are the most effective and reliable ways to capture motivation and adherence when devices or advanced tools are unavailable?
- Refining reporting standards
- How can reporting standards for all movement behaviours evolve to better capture the qualitative and quantitative aspects of these behaviours in clinical and research settings?
- CF-specific guidelines
- What specific physical activity recommendations can be developed for CF populations, given the current lack of tailored guidelines?
- Advanced analytics for data processing
- How can machine learning and raw data analytics be applied to provide more actionable insights in physical activity research?
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bradley J, O'Neill B, Kent L, et al. Physical activity assessment in cystic fibrosis: a position statement. J Cyst Fibros 2015; 14: e 25–e 32. doi:10.1016/j.jcf.2015.05.01126219990 · doi ↗ · pubmed ↗
- 2Hay JA, Brock University, Cairney J. Development of the habitual activity estimation scale for clinical research: a systematic approach. Pediatr Exerc Sci 2006; 18: 193–202. doi:10.1123/pes.18.2.193 · doi ↗
- 3Tokuçoğlu F. Monitoring physical activity with wearable technologies. Noro Psikiyatr Ars 2018; 55: Suppl. 1, S 63–S 65. doi:10.29399/npa.2333330692859 PMC 6278615 · doi ↗ · pubmed ↗
- 4Rowlands AV. Moving forward with accelerometer-assessed physical activity: two strategies to ensure meaningful, interpretable, and comparable measures. Pediatr Exerc Sci 2018; 30: 450–456. doi:10.1123/pes.2018-020130304982 · doi ↗ · pubmed ↗
- 5Tremblay MS, Carson V, Chaput JP, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab 2016; 41: Suppl. 3, S 311–S 327. doi:10.1139/apnm-2016-015127306430 · doi ↗ · pubmed ↗
- 6Rollo S, Antsygina O, Tremblay MS. The whole day matters: understanding 24-hour movement guideline adherence and relationships with health indicators across the lifespan. J Sport Health Sci 2020; 9: 493–510. doi:10.1016/j.jshs.2020.07.00432711156 PMC 7749249 · doi ↗ · pubmed ↗
- 7Loo BKG, Okely AD, Pulungan A, et al. Asia-Pacific consensus statement on integrated 24-hour activity guidelines for children and adolescents. Br J Sports Med 2022; 56: 539–545. doi:10.1136/bjsports-2021-10452734750119 · doi ↗ · pubmed ↗
- 8Wang Y, Nie J, Ferrari G, et al. Association of physical activity intensity with mortality: a national cohort study of 403 681 US adults. JAMA Intern Med 2021; 181: 203–211. doi:10.1001/jamainternmed.2020.633133226432 PMC 7684516 · doi ↗ · pubmed ↗