A Novel Treatment Strategy for Unresectable Locally Recurrent Rectal Cancer—Upfront Carbon-Ion Radiotherapy Followed by Surgical Resection of the Irradiated Intestines
Kei Kimura, Hirotoshi Takiyama, Shigeru Yamada, Kazuma Ito, Mizuki Koba, Ayako Imada, Jihyung Song, Kozo Kataoka, Takako Kihara, Ikuo Matsuda, Naohito Beppu, Yuki Horio, Kazuhiro Kitajima, Motoi Uchino, Hiroki Ikeuchi, Masataka Ikeda

TL;DR
A new treatment for hard-to-surgery rectal cancer involves radiation followed by removing the treated intestines, showing potential safety and effectiveness.
Contribution
A novel treatment strategy combining upfront carbon-ion radiotherapy with subsequent surgical resection of irradiated intestines for unresectable rectal cancer.
Findings
All patients completed treatment without acute adverse events from carbon-ion radiotherapy.
Late complications were mild, with no severe surgical complications in most patients.
The approach showed potential for managing unresectable rectal cancer with acceptable outcomes.
Abstract
R1/R2 resection for locally recurrent rectal cancer (LRRC) has a poor prognosis, comparable to that of nonsurgical treatments. Given the high invasiveness and its association with quality of life deterioration, carbon-ion radiotherapy (CIRT) is considered a feasible treatment option for unresectable LRRC in Japan. CIRT offers a narrow dose distribution that spares normal organs and increases the rate of cell apoptosis. However, LRRC occurs within the narrow pelvis and often adheres to adjacent intestines, making CIRT unfeasible. To maintain a safe distance between the tumors and intestines, surgical spacer placement has been performed; however, this intervention carries the risk of secondary tumor dissemination and iatrogenic injury to the intestinal tract. In this study, we evaluated the feasibility of a novel treatment strategy, namely, upfront CIRT followed by surgical resection of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
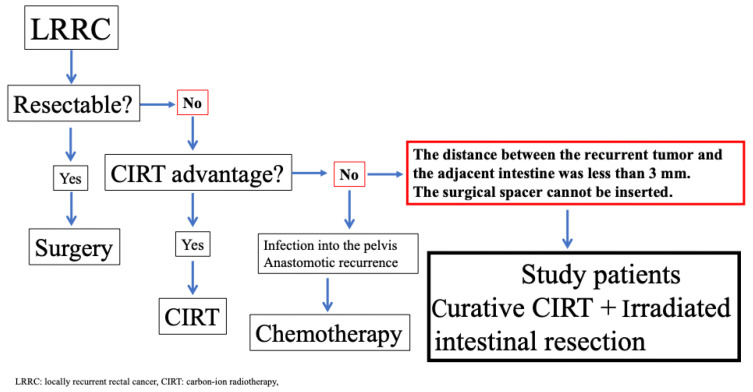 Figure 1
Figure 1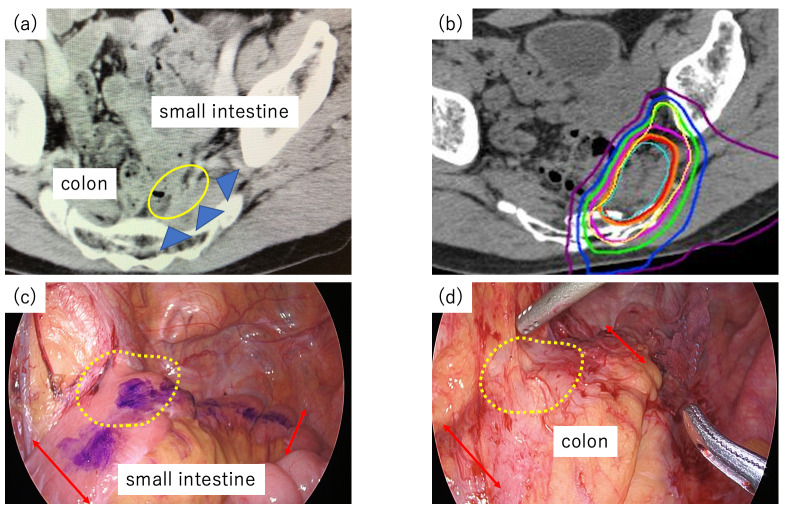 Figure 2
Figure 2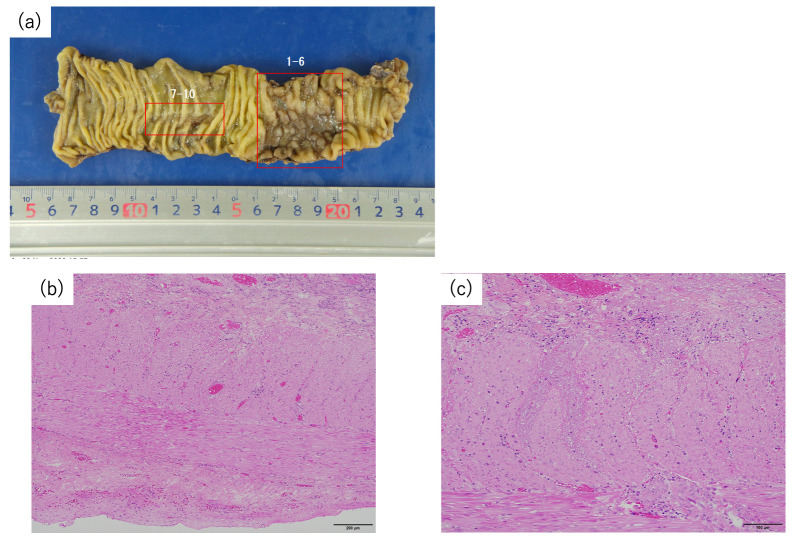 Figure 3
Figure 3| Surgery Type | Operating Time | Blood Loss (mL) | Postoperative Hospitalization (Days) | Surgical Complications (C/D Grade) | Surgical Complications | |
|---|---|---|---|---|---|---|
| 1 | LAR | 457 | 70 | 21 | II | Bleeding from anastomosis |
| 2 | Small intestine resection | 247 | 0 | 8 | 0 | − |
| 3 | LAR | 359 | 200 | 18 | 0 | − |
| 4 | Small intestine resection | 162 | 15 | 7 | 0 | − |
| 5 | LAR | 613 | 152 | 22 | II | Urinary dysfunction |
| 6 | LAR | 425 | 50 | 26 | II | Ileus |
| 7 | Small intestine resection | 245 | 1015 | 10 | 0 | − |
| 8 | LAR | 470 | 100 | 28 | 0 | |
| 9 | LAR | 240 | 0 | 14 | 0 | |
| 10 | Small intestine resection | 245 | 60 | 13 | 0 | |
| 11 | LAR | 267 | 0 | 30 | II | Ileus |
| 12 | LAR | 523 | 385 | 38 | IIIa | Pancreatitis |
| Patients | In-Field Recurrence | Time to Recurrence (Months) | Out-of-Field Recurrence | Time to Recurrence (Months) | Distant Recurrence | Time to Recurrence (Months) | Recurrence Site | Mortality | Follow-Up Duration (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | − | + | 12 | + | 17 | Lung | Yes | 60 | |
| 2 | − | − | − | − | No | 60 | |||
| 3 | − | − | − | No | 60 | ||||
| 4 | − | + | 25 | No | 57 | ||||
| 5 | − | − | + | 6 | Lung | No | 36 | ||
| 6 | − | − | − | − | No | 39 | |||
| 7 | − | − | − | − | No | 36 | |||
| 8 | − | + | 8 | + | 28 | Lung | No | 46 | |
| 9 | + | 12 | − | + | 20 | Lung | No | 28 | |
| 10 | − | − | No | 36 | |||||
| 11 | − | − | − | No | 20 | ||||
| 12 | − | − | − | No | 27 |
- —Hyogo Medical University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Advanced Radiotherapy Techniques · Colorectal and Anal Carcinomas
1. Introduction
For locally recurrent rectal cancer, surgical resection is the first choice of treatment and often requires the combined resection of adjacent organs [1,2,3,4,5]. However, the complicated pelvic anatomy of the lateral pelvic compartments limits the indications for surgical resection and makes it challenging to achieve R0 resection [6,7,8]. Recently, carbon-ion radiotherapy (CIRT) has received attention as a promising treatment option for unresectable locally recurrent rectal cancer (LRRC) in Japan [9,10,11,12]. It is characterized by a narrow dose distribution that protects healthy organs and includes frequent DNA double-strand breaks, leading to a relatively high rate of cell apoptosis. Unfortunately, CIRT is contraindicated for patients with recurrent tumors attached to the surrounding intestines due to radiation-induced adverse events (AEs), such as ulcers, bleeding, or intestinal perforation [13,14]. For unresectable LRRC near the intestine, we place a surgical spacer between the tumor and adjacent intestines to allow adequate irradiation via CIRT [15]. In prostate cancer treatment, spacer placement ensures an effective margin from the rectum [16,17,18,19]. Local recurrent tumors typically occur within the narrow pelvis, which often adhere to the adjacent intestines, making CIRT unfeasible, because performing a spacer placement procedure increases the risk of secondary tumor dissemination and iatrogenic intestinal injury. The use of spacers is not recommended in cases involving bowel resection due to the increased risk of infection. Therefore, alternative treatment approaches involving CIRT are needed. Here, we demonstrate a novel treatment strategy involving upfront curative-dose CIRT targeted at recurrent tumors to ensure curability and address the potential risk of severe adverse events (AEs) by planned surgical resection of the irradiated intestine. This study aimed to evaluate the safety of our new combination treatment.
2. Materials and Methods
2.1. Patients
Patients were selected from the locally recurrent rectal cancer database of Hyogo Medical University Hospital between April 2019 and December 2023. This study was approved by the institutional review board of Hyogo Medical University (No. 4440). LRRC was defined as recurrence in the pelvis after prior treatment, with patients required to have been disease-free for at least six months between the initial surgery and the diagnosis of LRRC. All computed tomography (CT) and magnetic resonance imaging (MRI) images were assessed by gastrointestinal radiologists and colorectal surgeons. Our treatment strategy for LRRC patients is shown in Figure 1. CIRT was recommended for patients with LRRC if radical surgery was contraindicated, such as in cases of unresectable distant metastasis, unfit medical status, sacral involvement above the S2 vertebra, invasion into the lateral pelvic compartments extending beyond the internal obturator muscles, or when patients declined extensive surgery [20]. On the other hand, CIRT is contraindicated for patients with recurrent tumors located less than 3 mm from the adjacent intestine [21]. In such cases, spacer placement is generally indicated to ensure an appropriate distance from the recurrent tumor [15]. However, in patients with LRRC, spacer placement is contraindicated when preoperative imaging suggests severe adhesion between the tumor and the adjacent intestines, as mobilizing the adjacent intestine may increase the risk of tumor dissemination or intestinal injury. The eligibility criteria for this study were that the distance between the unresectable recurrent tumor and the adjacent intestine was less than 3 mm and that the surgeons could not insert the surgical spacer. Patients with anastomotic recurrence or LRRC invading the bowel lumen were excluded.
2.2. Treatment
Treatment strategies for LRRC were defined for each patient, following an interdisciplinary online meeting between Hyogo Medical University and the National Institutes for Quantum Science and Technology (QST) Hospital. CIRT was administered to the enrolled patients using the methods described by Yamada et al. at QST Hospital [10,22]. The treatment dose for CIRT was set at 73.6 gray relative biologic effectiveness (Gy (RBE)) for patients without a history of prior irradiation or at 70.4 Gy (RBE) for patients with a history of previous irradiation to the pelvic area, and it was delivered in 16 fractions without concurrent chemotherapy [21]. The treatment was performed daily, four days a week. The target field included the gross tumor volume and the surrounding clinical target volume with a 10 mm margin to the tumor. Therefore, the field partially included the adjacent intestines in the planned irradiation field. Within approximately eight weeks after the completion of CIRT, intestinal tracts irradiated with more than 46 Gy were considered for resection [23]. The extent of the irradiated intestines was carefully discussed at the two hospitals.
A key concept of this study was that the surgery was not intended for tumor excision, but for the removal of irradiated intestines that carried a high risk of severe complications such as massive bleeding, obstruction, or perforation. The LRRC itself was treated with curative intent through CIRT and was not included in surgical resection. During surgery, we marked the extent of intestinal resection using crystal violet following the distribution map by identifying local adhesions of the intestine on the pelvis and the small intestine dropping down into the pelvic cavity before shifting the patient to the surgical position. When the neorectum, including the anastomotic site, was resected, the LRRC itself remained in the pelvis, and only the irradiated intestines were removed. In addition, careful attention was required to prevent intestinal injury, as it could lead to severe postoperative pelvic sepsis. Resection of the neorectum was minimized, while a wider resection of the small intestine was performed when it adhered to the tumor, since the irradiated area of the small intestine was often unclear. If the recurrent tumors were firmly fixed to the mesentery, only the irradiated intestinal wall was resected without dissecting the mesentery. Finally, an omental pedicle flap was placed between the recurrence site and the intestine to enable reirradiation in cases of tumor re-recurrence [24,25].
2.3. Follow-Up
Acute and late AEs of CIRT were defined according to the National Cancer Institute-Common Toxicity Criteria for Adverse Events version 5.0 [26]. Acute AEs were defined as toxicity persisting within 90 days after the completion of CIRT. Late AEs were defined as the presence of toxicity observed 3 months or later after irradiation. Severe AEs of CIRT were defined as those that were Grade 3 or higher [27]. Postoperative complications were assessed using the Clavien–Dindo classification [28]. All resected samples were investigated by specialized GI pathologists.
For follow-up, the standard protocol included carcinoembryonic antigen (CEA) and carbohydrate antigen (CA19-9) measurements every three months and thoracoabdominal computed tomography (CT) once every six months for five years after surgery. If suspected systemic recurrence was found, further examination to ensure an accurate diagnosis was performed using magnetic resonance imaging (MRI) or positron emission tomography–CT, depending on the site of recurrence. Regarding local re-recurrence, we also defined “in-field recurrence” as an enlarged recurrent tumor inside the planning target volume and “out-of-field recurrence” as an enlarged recurrent tumor outside the planning target volume.
Clinical data, including patient characteristics, previous history of rectal cancer, CIRT details, irradiated intestine resection details, postoperative complications, histopathological findings, and prognosis, were collected. Survival and disease recurrence were described to determine oncologic outcomes.
3. Results
A total of twelve patients were included in this study; the patient characteristics are summarized in Table 1. Among these 12 patients, 10 were male, and the median age was 64 years (range, 38–78 years). Curative surgery was contraindicated in ten patients because of the necessity of bilateral S1 nerve resection, in one patient with lateral recurrence infiltrating beyond the internal obturator muscles, and in one patient who declined extensive surgery because of intolerable deterioration in postoperative quality of life. Details of CIRT for patients who underwent this novel treatment are shown in Table 2. All patients completed the scheduled treatment course. Nine patients were administered 73.6 Gy (RBE) in 16 fractions; on the other hand, three patients with prior pelvic X-ray radiotherapy were administered 70.4 Gy (RBE) in 16 fractions. Figure 2 shows a case of LRRC adjacent to the neorectum and small intestine.
Regarding AEs, no severe acute AEs, such as general, gastrointestinal, or skin disorders, were noted. On the other hand, three patients had sciatic neuralgia as a late AE, including two with Grade 1 and one with Grade 3. The patient with Grade 3 late AEs was prescribed nonsteroidal anti-inflammatory drugs, pregabalin, and opioids postoperatively for sciatic neuralgia. He had a limp in his left leg but could ambulate with assistance. However, no improvement in symptoms was observed during the follow-up period. The median interval between completing CIRT and surgery was four weeks (range, 3–8). The operative details and postoperative morbidities are presented in Table 3. All procedures were conducted using a laparoscopic approach. Seven patients underwent low anterior resection (LAR) with combined resection of the anastomotic site. Four patients underwent adjacent small intestine resection, and one patient underwent low anterior resection with small intestine resection. Patients who underwent LAR had diverting ileostomy. The median operating time was 313 min (range, 162–613), and the intraoperative blood loss volume was 85 mL (range, 0–1065). One patient developed Grade III pancreatitis during the mobilization of the splenic flexure, while no other patients experienced Grade III or higher postoperative complications. The duration of postoperative hospitalization was 20 days (range, 7–50). Pathology revealed severe damage to the muscle layer in the irradiated intestine, and no residual cancer cells were found (Figure 3). The median follow-up duration was 40 months (range, 20–60), and one patient was diagnosed with in-field recurrence 12 months after CIRT. The other three patients were diagnosed with out-of-field recurrence after CIRT. All patients with local re-recurrence later received reirradiation with CIRT. At the completion of the study, four patients experienced lung recurrence, and one patient died due to rectal cancer-specific causes. The 3-year overall survival (OS) rate was 90%, and the 3-year recurrence-free survival rate was 57.1%. The 3-year in-field recurrence-free survival rate was 90%, and the 3-year out-of-field recurrence-free survival rate was 72.2% (Table 4).
4. Discussion
In this study, we demonstrated the safety of a novel treatment strategy for patients with LRRC located less than 3 mm from the intestine, where CIRT would otherwise be contraindicated. This method involves CIRT as a curative treatment for recurrent tumors, accepting the risk of AEs affecting the adjacent intestinal tracts, followed by resection of “high-risk” irradiated intestines. Crucially, the core principle of this treatment strategy is that CIRT is not used as neoadjuvant therapy, but as the definitive curative treatment. The purpose of surgery is not tumor resection, but the removal of irradiated intestines with a high risk of severe AEs. With respect to the safety of this treatment strategy, all twelve patients did not experience severe acute AEs, but three patients experienced neuralgia as late AEs (one Grade 3 and two Grade 1), and one severe postoperative complication was deemed acceptable. With respect to the efficacy of this treatment strategy, one patient experienced in-field recurrence, and three patients experienced out-of-field recurrence. They received reirradiation with CIRT, which resulted in local control. To our knowledge, our study is the first to report the findings of this novel treatment strategy.
The advantage of our novel strategy is that full-dose CIRT provides better therapeutic effects [29]. In this study, the median tumor size was relatively small, at 24 mm. In Japan, high sacrectomy above the lower edge of the S2 vertebra is typically contraindicated, as it requires the removal of the sacroiliac joint and bilateral S1 nerves. Thus, CIRT is increasingly regarded as a promising therapeutic alternative for such patients. Prior to intestinal resection, all tumor cells had already been irradiated with curative doses, which could result in apoptosis [14]. Thus, it was hypothesized that the irradiated intestine was removed without the risk of dissemination. In a phase I/II trial, Yamada et al. revealed that irradiation at 70 Gy (RBE) or greater resulted in an overall 5-year local control rate of approximately 80% [10]. Similarly, Takiyama et al., in a cohort of 473 patients with LRRC, reported that patients without prior radiation within the pelvis (n = 390) received a dose of 73.6 Gy (RBE), whereas those with prior radiation within the pelvis (n = 83) received 70.4 Gy (RBE). The 3-year OS rates for the prior radiation-negative and prior radiation-positive groups were 73% (95% CI; 68–77%) and 76% (65–84%), respectively, with both groups achieving 3-year local control rates of 80% (75–84%) and 80% (68–88%), respectively [21]. These findings demonstrate that delivering curative doses can provide a valuable treatment option. Although CIRT achieves a high rate of local control, dose reduction is necessary when the recurrent tumor is near the intestines to minimize the risk of severe radiation-induced AEs [13]. As reported by Barcellini et al., this dose reduction resulted in approximately 80% in-field recurrence occurring at the tumor edge near the adjacent intestine. Regardless of prior RT status, a dose of at least 70.4 Gy (RBE) is essential for curative intent [24]. The results of our study suggest that our novel treatment strategy using CIRT may achieve definitive local control.
For patients with unresectable LRRC, the most important aspect is ensuring the safety of this treatment strategy. Among the AEs associated with CIRT, severe late AEs occurred in one of the twelve patients. Yamada et al. reported that acute severe AEs occurred in 10% of patients treated with CIRT, and the late severe AE rate was 21%. Therefore, these numbers of severe AEs in CIRT patients were similar to those reported in this study [22]. The patient with the severe late AE in our study developed lower limb pain, along with a left leg limp. However, this deterioration in the patient’s quality of life seemed to be within tolerance because he was able to ambulate with the assistance of a cane. Thus, we considered this case acceptable. In addition, regarding the safety of surgery for the irradiated intestine, only one patient experienced a Grade 3 complication during the postoperative course. The patient developed pancreatitis and a gastropancreatic fistula; however, endoscopic transgastric drainage was later performed successfully. Despite the low postoperative complication rates, the length of hospital stay remains long in Japan. This is because patients need to acquire stoma self-care skills before discharge due to an insufficient post-discharge support system.
The third consideration involves whether resection of the irradiated intestine is necessary. On the basis of the histopathological findings of this study, damage to muscle layers, such as fibrosis, eosinophilic changes, hyalinization, and thinning, was more severe in our patients than in those receiving conventional chemoradiotherapy (CRT). Thus, perforation of the irradiated intestines may have occurred after a certain period. Matsushita et al. reported that, compared to conventional CRT, CIRT was associated with a higher incidence of AEs occurring relatively late after irradiation (9–18 months) [23,30]. To date, the optimal period for the planned resection of the irradiated intestine is not clear. Therefore, we determined that the planned resection of the irradiated intestine within 8 weeks would provide favorable therapeutic benefits, similar to those of conventional treatment involving a long course of neoadjuvant CRT [31,32,33], thus avoiding late-onset AEs. Despite performing irradiated intestine resection within 8 weeks after the completion of CIRT, two patients exhibited severe damage to the muscle layers; therefore, early irradiated intestine resection is recommended. In addition, since we were able to transect the intestine before inflammation induced fibrosis, the removal of the irradiated intestines was not difficult. Hence, this treatment strategy is beneficial in terms of safety.
Nonetheless, our study has several limitations, mainly due to its small sample size and short observation period, and our study results are limited to the Japanese population. One patient experienced in-field recurrence, and three patients experienced out-of-field recurrence. Thus, comprehensive follow-up is needed. Moreover, further improvement of preoperative diagnostic assessments using multimodal imaging is essential to develop a better, more effective treatment strategy for LRRC patients. More data are necessary to validate the efficacy and safety of this approach.
5. Conclusions
In conclusion, our study revealed that a novel strategy combining CIRT followed by surgical resection of the irradiated intestine can provide favorable outcomes for patients with unresectable LRRC. This approach can represent a feasible treatment option for future patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moriya Y. Akasu T. Fujita S. Yamamoto S. Total pelvic exenteration with distal sacrectomy for fixed recurrent rectal cancer in the pelvis Dis. Colon Rectum 200447204420532047–2053, discussion 2044–205310.1007/s 10350-004-0714-915657653 · doi ↗ · pubmed ↗
- 2Kelly M.E. Aalbers A.G. Aziz N.A. Abraham-nordling M. Alberda W. Antoniou A. Austin K.K. Baker R. Bali M. Baseckas G. Changing outcomes following pelvic exenteration for locally advanced and recurrent rectal cancer BJS Open 201935165203138864410.1002/bjs 5.50153 PMC 6677093 · doi ↗ · pubmed ↗
- 3Solomon M.J. Brown K.G.M. Extended Radical Resection: The Standard of Care for Patients with Advanced Pelvic Malignancy Ann. Surg. Oncol.20202732332410.1245/s 10434-019-07817-731520207 · doi ↗ · pubmed ↗
- 4Platt E. Dovell G. Smolarek S. Systematic review of outcomes following pelvic exenteration for the treatment of primary and recurrent locally advanced rectal cancer Tech. Coloproctol.20182283584510.1007/s 10151-018-1883-130506497 · doi ↗ · pubmed ↗
- 5Aiba T. Uehara K. Tsuyuki Y. Ogura A. Murata Y. Mizuno T. Yamaguchi J. Kokuryo T. Yokoyama Y. Ebata T. Minimum radial margin in pelvic exenteration for locally advanced or recurrent rectal cancer Eur. J. Surg. Oncol.2022482502250810.1016/j.ejso.2022.06.01535768314 · doi ↗ · pubmed ↗
- 6Boyle K.M. Sagar P.M. Chalmers A.G. Sebag-Montefiore D. Cairns A. Eardley I. Surgery for locally recurrent rectal cancer Dis. Colon Rectum 20054892993710.1007/s 10350-004-0909-015785880 · doi ↗ · pubmed ↗
- 7Rokan Z. Simillis C. Kontovounisios C. Moran B.J. Tekkis P. Brown G. Systematic review of classification systems for locally recurrent rectal cancer BJS Open 20215 zrab 02410.1093/bjsopen/zrab 02433963369 PMC 8105621 · doi ↗ · pubmed ↗
- 8Sakata S. Karim S.M. Mathis K.L. Kelley S.R. Rose P.S. Dozois E.J. Posterior-First Two-Stage Approach to En Bloc Resection of Locally Recurrent Rectal Cancer Involving the Pelvic Sidewall Dis. Colon Rectum 202164 e 465e 47010.1097/DCR.000000000000209134214058 · doi ↗ · pubmed ↗