Treatment and Outcomes in Advanced Gastroesophageal Adenocarcinoma in the Pre-Immunotherapy Era Based on the Spanish AGAMENON-SEOM Registry
Paula Jimenez-Fonseca, Alberto Carmona-Bayonas, Jaime Álvarez-Cañada, Amy Storfer-Isser, Marta Martin-Richard, Tamara Sauri, Juana María Cano, Elia Martínez Moreno, Pablo Pérez-Wert, Javier López, Francisco Garcia Navalon, Lucía Gómez-González, Maribel Ruiz Martín

TL;DR
This study compares treatment and survival outcomes for HER2-negative and HER2-positive advanced gastric/gastroesophageal junction cancer patients in Spain before immunotherapy was available.
Contribution
The study highlights the survival gap between HER2-negative and HER2-positive patients and emphasizes the need for targeted therapies in the HER2-negative group.
Findings
HER2-negative patients had shorter progression-free and overall survival compared to HER2-positive patients.
Most HER2-positive patients received trastuzumab as part of first-line treatment.
Approximately 70% of patients with advanced G/GEJa were HER2-negative.
Abstract
There is an unmet need for targeted therapy for human epidermal growth factor receptor 2–negative (HER2-negative), locally advanced or metastatic gastric/gastroesophageal junction adenocarcinoma (advanced G/GEJa), which is associated with poor survival outcomes. This study aimed to describe the characteristics, treatment, and survival of HER2-negative and HER2-positive patients with advanced G/GEJa in Spain. Among 1357 patients from the Spanish AGAMENON-SEOM registry who initiated first-line polychemotherapy for advanced G/GEJa between 2015 and 2019 (inclusive), 70.1% had HER2-negative disease. Overall, 56.3% of patients with advanced G/GEJa received only one line of therapy, and most (92.7%) HER2-positive patients received targeted therapy (trastuzumab) as part of first-line treatment. HER2-negative patients had significantly shorter progression-free survival (median of 5.92 months vs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
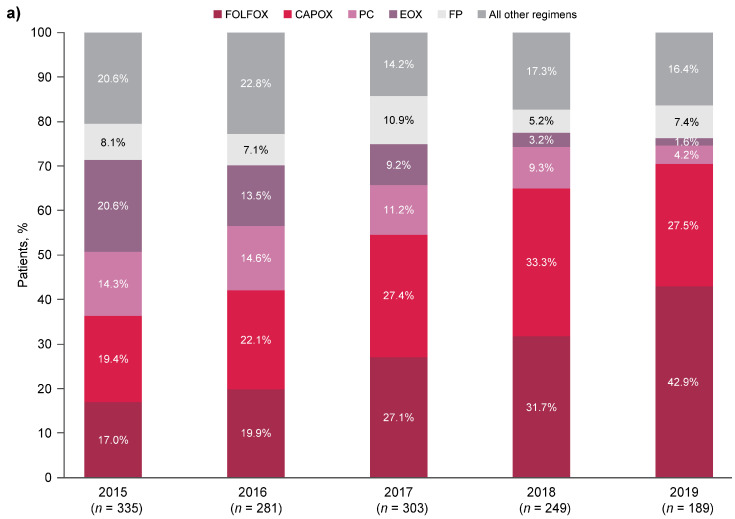 Figure 1
Figure 1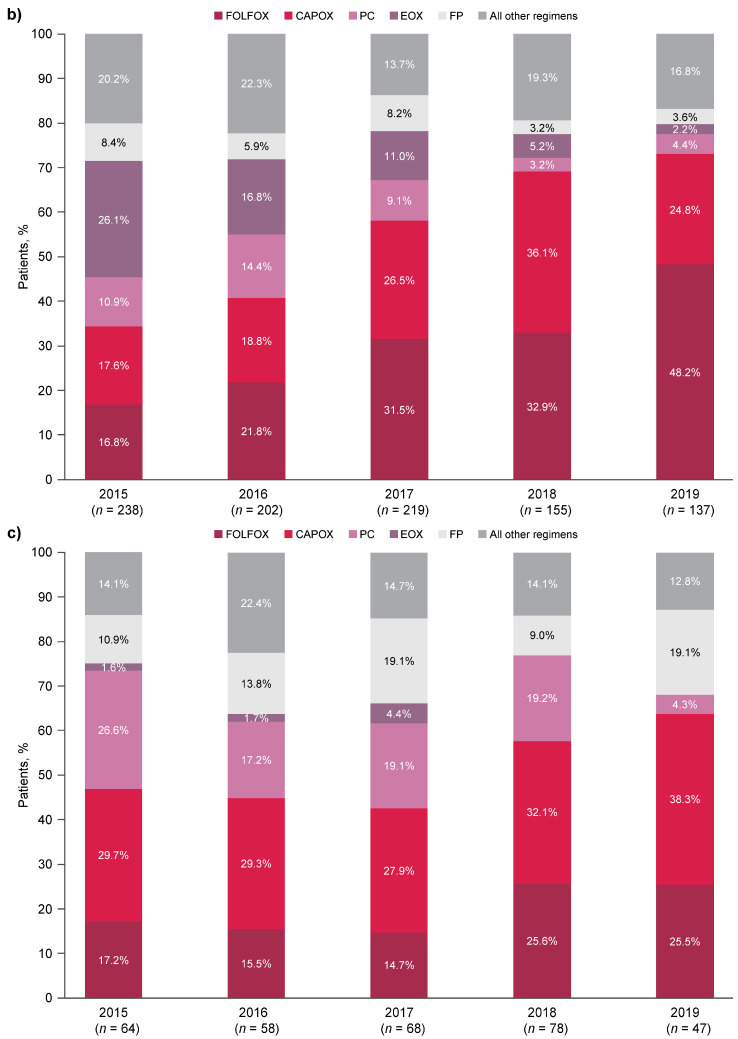 Figure 2
Figure 2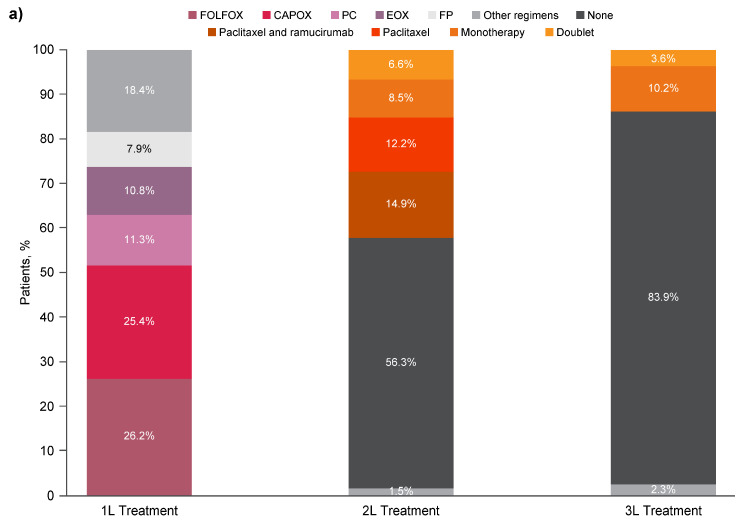 Figure 3
Figure 3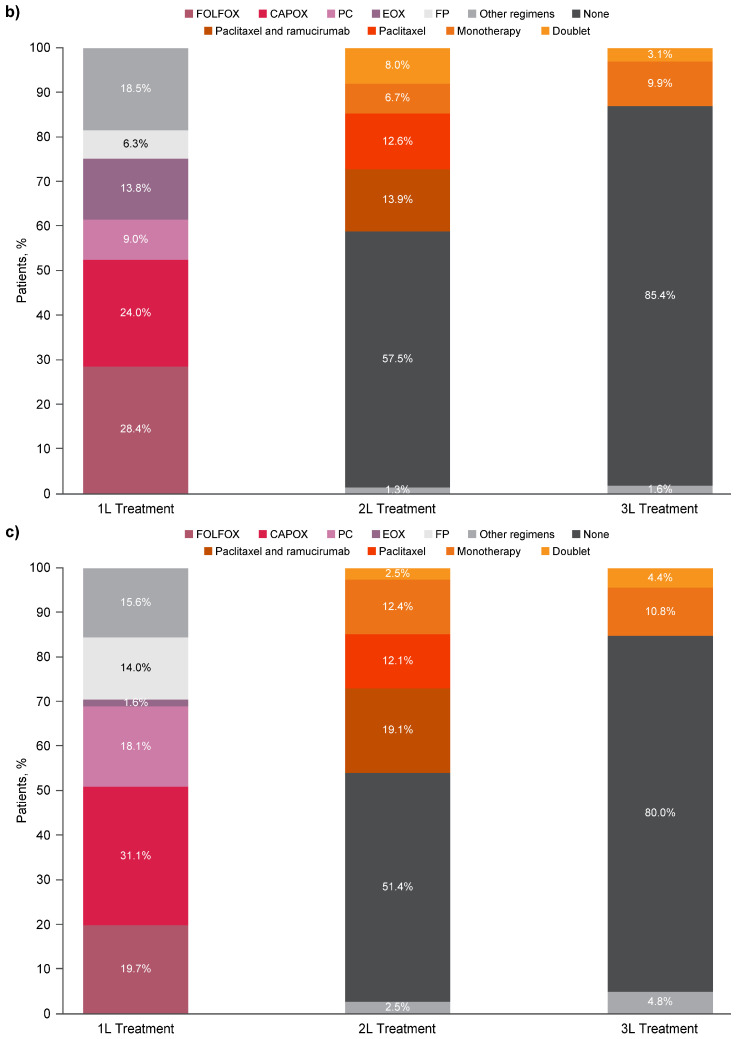 Figure 4
Figure 4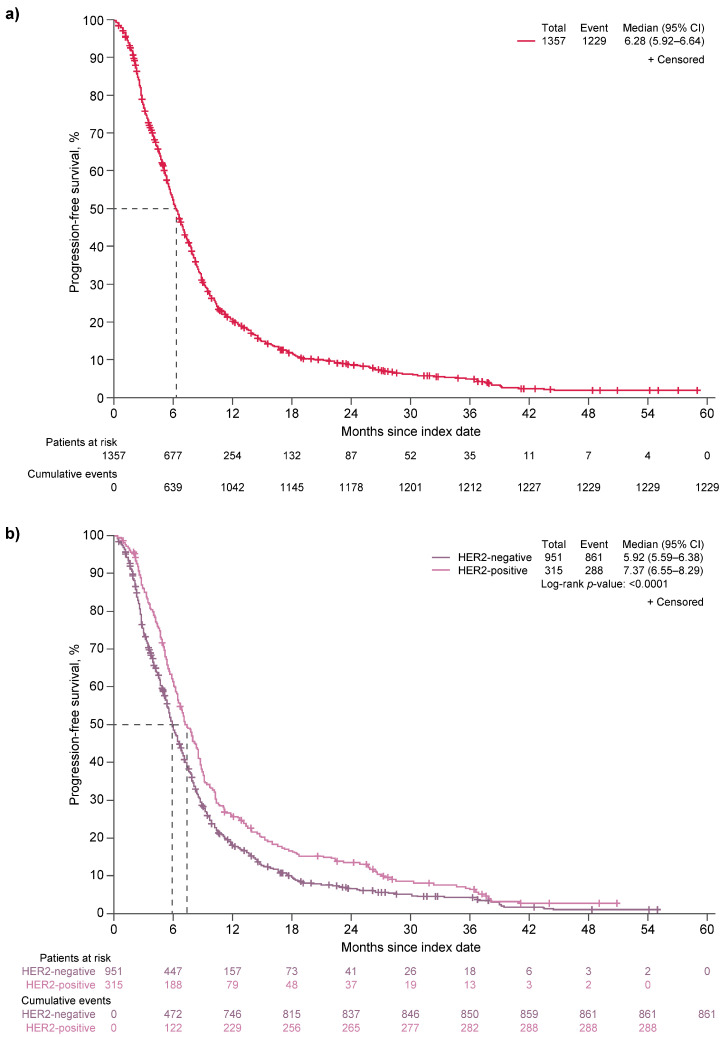 Figure 5
Figure 5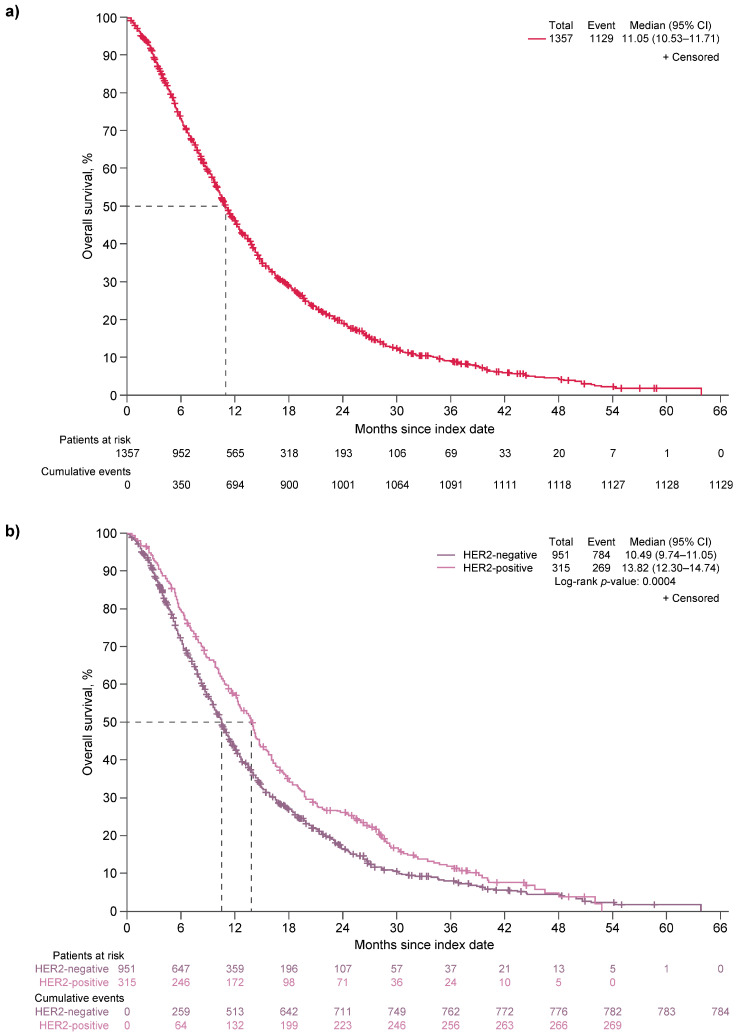 Figure 6
Figure 6- —Astellas Pharma Europe Ltd.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Colorectal and Anal Carcinomas
1. Introduction
Gastric cancer is the fifth most common cancer worldwide and a leading cause of cancer-related death, with nearly a million new cases globally and more than 650,000 deaths in 2022 [1]. The worldwide age-standardized 5-year survival rate for stomach cancer was 20–40% in 2000–2014 [2], and patients with locally advanced or metastatic gastroesophageal junction (GEJ) adenocarcinoma have a median survival of 7–11 months [3]. The incidence rate of gastric adenocarcinoma is higher than that of GEJ adenocarcinoma; for example, in an analysis of real-world data from patients with advanced gastric, GEJ, or esophageal adenocarcinoma in the Spanish AGAMENON-SEOM registry, the primary tumor location was the stomach in the majority of patients (78%), compared with the GEJ (13%) or esophagus (9%) [4]. However, data demonstrate a decline in gastric adenocarcinoma and an increase in GEJ adenocarcinoma since the 1970s [1,5,6]. In Spain, gastric cancer was the ninth most common cancer in 2021 and the eighth most common cause of cancer-related death in 2020 [7]. Although mortality rates in Spain are lower than global rates, there are still over 5000 deaths in Spain every year due to gastric cancer [7], and the 5-year net survival rate between 2008 and 2013 was 27.4% among patients with gastric cancer [8]. The burden of gastric and gastroesophageal junction adenocarcinoma (G/GEJa) is high, even compared with other cancers, with increasingly severe symptoms, worsening health-related quality of life, and accelerating healthcare resource utilization and cost as the disease advances [9].
There have been therapeutic advances for patients with human epidermal growth factor receptor 2–overexpressing (HER2-positive) G/GEJa. Notably, trastuzumab is a monoclonal antibody that binds to the extracellular domain of the transmembrane receptor protein HER2, inhibiting proliferation of HER2-expressing tumors and activating antibody-dependent cellular cytotoxicity [10]. Trastuzumab, in combination with chemotherapy, significantly improved overall survival (OS) and progression-free survival (PFS) in patients with HER2-positive, locally advanced unresectable or metastatic G/GEJa (advanced G/GEJa) compared with chemotherapy alone in a clinical study [11] and subsequently became a standard treatment for this disease [12]. Prior to the advent of trastuzumab, patients with HER2-positive G/GEJa had outcomes similar to, or worse than, patients with HER2-negative disease [10,13,14]. However, they now have a survival advantage because of their eligibility for targeted therapy and trastuzumab deruxtecan as second-line (2L) therapy [13,15,16].
Subsequently, therapies targeting programmed death receptor 1 (PD-1), an immune checkpoint protein, became available. Pembrolizumab is a PD-1 inhibitor recently approved, in conjunction with trastuzumab and chemotherapy, for first-line (1L) treatment of patients with HER2-positive G/GEJa expressing programmed death-ligand 1 (PD-L1; combined positive score [CPS] ≥ 1) [17,18,19]. For patients with HER2-negative G/GEJa, pembrolizumab and nivolumab (another PD-1 inhibitor) are approved for 1L treatment of adults with HER2-negative advanced or metastatic G/GEJ or esophageal adenocarcinoma whose tumors express PD-L1 [17,18,20]. When used in combination with chemotherapy in patients with HER2-negative disease, nivolumab and pembrolizumab significantly improved PFS and OS compared with chemotherapy alone [21,22]. Because PD-L1 is not ubiquitously expressed in G/GEJ tumors (~50%) [23,24,25], there remains an unmet need for more effective, targeted treatment for patients with HER2-negative advanced G/GEJa who are not candidates for immunotherapy. Overall, approximately three-quarters of patients with advanced G/GEJa have HER2-negative disease [10,26].
This study was conducted using real-world data from the AGAMENON-SEOM registry to describe the clinical characteristics, treatment patterns, and survival outcomes (PFS and OS) in Spanish patients with advanced G/GEJa. Additionally, this study compared PFS and OS by HER2 status and estimated the number of patients in Spain with HER2-negative advanced G/GEJa who were eligible for 1L polychemotherapy.
2. Methods
2.1. AGAMENON-SEOM Registry
AGAMENON-SEOM is an observational, clinicopathological registry managed by the Spanish Society of Medical Oncology (SEOM). Its purpose is to describe the diagnosis and treatment approaches for G/GEJa in a clinical practice setting according to each participating center’s usual practice [27]. The registry contains data on over 4000 patients from 40 Spanish hospitals, including 2470 patients who received 1L polychemotherapy [4]. Sixteen of the 17 regions in Spain are represented, allowing geographical coverage across the country, with more participating centers located in regions with greater population density.
Eligibility criteria for patients included in this analysis of the AGAMENON-SEOM registry are summarized in Table 1. Briefly, eligible patients are adults (≥18 years) with histologically confirmed advanced gastric, GEJ, or distal esophageal adenocarcinoma who were treated with at least one cycle of 1L polychemotherapy and were followed for at least 3 months (except for patients who died sooner than 3 months after treatment initiation) [28,29,30]. Patients are excluded from the registry if they participated in a clinical trial without standard chemotherapy; received prior systemic therapy for advanced gastric, GEJ, or distal esophageal adenocarcinoma; completed prior neoadjuvant or adjuvant chemotherapy, radiotherapy, or chemoradiotherapy less than 6 months earlier; or were diagnosed with any cancer other than G/GEJa.
The data were gathered using a web-based data collection tool and managed through a website (http://www.agamenonstudy.com/) using filters and a system of queries to guarantee data reliability and control for inconsistent data [31].
2.2. Study Design
This longitudinal cohort study included patients from the AGAMENON-SEOM registry who initiated 1L polychemotherapy for advanced G/GEJa in Spain between 1 January 2015 and 31 December 2019 (Table 1). The study period was between 1 January 2015 and 31 December 2021, allowing at least 2 years of follow-up data for each patient. Patients were excluded from the study if they had distal esophageal cancer (primary site).
2.3. Objectives
Using this cohort of patients who received 1L polychemotherapy for advanced G/GEJa, the objectives of this study were (1) to describe the disease management for all patients and stratified by HER2 status; (2) to describe the sociodemographic and disease characteristics of all patients and stratified by HER2 status; (3) to compare PFS and OS by HER2 status for all 1L regimens, and OS for the subsets of patients who received 1L FOLFOX (folinic acid, fluorouracil, and oxaliplatin) or 1L CAPOX (capecitabine and oxaliplatin); and (4) to estimate the number of patients in Spain with HER2-negative advanced G/GEJa who were eligible for 1L polychemotherapy.
2.4. Statistical Analysis
Descriptive statistics were used to summarize disease management and patient sociodemographic and disease characteristics. PFS was defined as the time from the index date, defined as the initiation date of 1L polychemotherapy for advanced G/GEJa, until the date of progressive disease or date of death by any cause (whichever occurred first). OS was defined as the time from the index date to date of death by any cause. Patients were censored at the date of their last contact or the end of the study (whichever occurred first).
PFS and OS were summarized using Kaplan–Meier estimates. The log-rank test was used to compare PFS and OS for patients with HER2-positive disease and HER2-negative disease. p-values < 0.05 were considered statistically significant. Accelerated failure time (AFT) models with a generalized gamma distribution [32] were used to compare OS for patients with HER2-negative disease and HER2-positive disease, as the proportional hazards assumption was violated for HER2 status. AFT models were fitted without confounders (unadjusted) and with adjustment for confounders that were preselected by study investigators: Lauren histological subtype (intestinal; diffuse; mixed; not available/not classifiable), number of metastatic sites (0–3; ≥4), Eastern Cooperative Oncology Group performance status (ECOG PS: 0; 1; ≥2), presence of bone metastases (yes; no), presence of ascites (yes; no), and neutrophil-to-lymphocyte ratio (NLR) category (<4; 4 to <8; ≥8). The results from the AFT models included the coefficient, standard error, time ratio (TR), 95% confidence interval (CI), and p-value. A TR < 1 indicates that HER2-negative status was associated with shorter survival (accelerated failure) compared with HER2-positive status (the reference category).
Six parameters were required to estimate the number of patients in Spain with HER2-negative advanced G/GEJa who were eligible for 1L polychemotherapy. Since there is no single data source representative of the Spanish population that includes all six parameters, information from the literature and the results of this study were used. The values of each parameter and their data sources were as follows: the number of new cases of G/GEJ cancer in Spain in 2024 (6868 patients; parameter 1 [33]) with advanced disease (84%; parameter 2 [34]) that was adenocarcinoma (90%; parameter 3 [35]) who were eligible for polychemotherapy (78.7%; parameter 4 [30]), were tested for HER2 (93.3%; parameter 5 [results from this study]), and had HER2-negative disease (75.1%; parameter 6 [results from this study]). Probabilistic sensitivity analyses (PSAs) were conducted to account for the plausible variation across parameters 2–6. Each parameter was considered a random variable and was assumed to have a beta distribution. Parameters were simultaneously changed, with values drawn by random sampling from the beta distribution. The PSA was repeated 10,000 times to generate new parameter values, quantify the uncertainty of the parameters, and produce an average estimate and 95% CI.
3. Results
3.1. Disposition
Of 4479 patients with advanced G/GEJa assessed for participation in the AGAMENON-SEOM registry, 3315 patients fulfilled all eligibility criteria and 1164 patients were excluded for the following reasons: 1065 patients did not receive combination chemotherapy using at least two drugs, 50 patients were not followed for at least 3 months, and 49 patients had completed prior neoadjuvant or adjuvant chemotherapy, radiotherapy, or chemoradiotherapy less than 6 months earlier. Of the 3315 patients fulfilling all eligibility criteria for the registry, 1513 patients initiated 1L polychemotherapy for advanced G/GEJa between 1 January 2015 and 31 December 2019. After excluding 156 patients with distal esophageal adenocarcinoma, the final study population included 1357 patients.
3.2. Sociodemographic and Disease Characteristics
Of the 1357 patients with advanced G/GEJa who were included in this study, 951 (70.1%) patients had HER2-negative disease, 315 (23.2%) patients had HER2-positive disease, and 91 (6.7%) patients had unknown HER2 status (Table 2). The median age (range) of all patients at 1L treatment initiation was 64.7 years (19.9–88.5); most patients were male (67.3%), just under half were aged 65 years or older (48.9%), and just over half had a body mass index of 18.5 to <25 kg/m^2^ (53.9%). Most patients had an ECOG PS of 0–1 (85.5%), a primary tumor site of the stomach (71.6%), and de novo disease (84.5%). The proportions of patients with diffuse (38.5%) and intestinal (37.1%) histologies were similar. Just over half of patients had ≥2 metastatic sites (51.6%), and the most common sites were locoregional lymph nodes (63.3%), peritoneum (48.6%), and non-locoregional lymph nodes (44.2%). Metastatic ascites was reported in 23.6% of patients, and 11.6% of patients had bone metastases. The median (range) NLR was 3.4 (0.3–102.0). Most patients (60.4%) had a low NLR (<4); 27.3% had a moderate NLR (4 to <8); and 10.5% had a high NLR (≥8).
There were some notable differences between patients with HER2-negative disease and patients with HER2-positive disease in terms of sociodemographic and disease characteristics. Compared with patients with HER2-positive disease, patients with HER2-negative disease were slightly younger (median age, 63.8 vs. 65.8 years) and fewer were male (64.7% vs. 75.6%); additionally, their primary tumor site was more likely to be gastric (75.6% vs. 58.1%) and to have diffuse histology (45.4% vs. 18.4%).
3.3. First-Line Treatment
Most patients (56.3%) received only one line of therapy. Between 2015 and 2019, the median (interquartile range) duration of 1L treatment was 4.8 months (2.8–7.2), and patients received a median (interquartile range) of 6 (4–11) chemotherapy cycles during 1L treatment (Table 3). Of the 315 patients with HER2-positive disease, 292 (92.7%) received trastuzumab as part of their 1L treatment regimen. Use of FOLFOX and CAPOX increased during the 2015–2019 period, as these therapies became commonly used 1L regimens for advanced G/GEJa from 2017 onward (Figure 1a). In the overall population and HER2-negative subgroup, the most common 1L chemotherapy regimen in 2019 was FOLFOX (Figure 1a,b); CAPOX was the most common 1L chemotherapy regimen in 2019 for patients with HER2-positive disease (Figure 1c).
3.4. Second- and Third-Line Treatment
As previously noted, a majority of patients (56.3%) received only one line of therapy; 27.6% of patients received two lines of therapy; and 16.1% received three lines of therapy. The most common 2L regimens during the 2015–2019 period were paclitaxel alone and paclitaxel in combination with ramucirumab (Figure 2a). Most patients who received third-line (3L) therapy were treated with monotherapy (Figure 2a). Similar trends for 2L and 3L treatment regimens were observed across HER2-negative and HER2-positive subgroups during the 2015–2019 period (Figure 2b,c).
3.5. PFS
Median PFS for all patients was 6.28 months (95% CI, 5.92–6.64; Figure 3a). Patients with HER2-negative disease had significantly shorter median PFS compared with those who had HER2-positive disease (5.92 months [95% CI, 5.59–6.38] vs. 7.37 months [95% CI, 6.55–8.29]; p < 0.0001; Figure 3b).
3.6. OS
Median OS was 11.05 months for all patients (95% CI, 10.53–11.71; Figure 4a). Patients with HER2-negative disease had a significantly shorter median OS compared with those with HER2-positive disease (10.49 months [95% CI, 9.74–11.05] vs. 13.82 months [95% CI, 12.30–14.74]; p = 0.0004; Figure 4b).
Results from AFT models showed that patients with HER2-negative disease had significantly shorter OS than those with HER2-positive disease (unadjusted TR, 0.790; 95% CI, 0.701–0.890; p = 0.0001 (Table S1); adjusted TR [aTR], 0.812; 95% CI, 0.722–0.913; p = 0.0005 (Table S2)). In the adjusted AFT model, the overall p-value for each confounder was statistically significant. Prognostic factors associated with worse OS included diffuse vs. intestinal histological subtype (aTR, 0.838; 95% CI, 0.742–0.946); ≥4 vs. 0–3 metastatic sites (aTR, 0.749; 95% CI, 0.622–0.900); ECOG PS of 1 vs. 0 (aTR, 0.852; 95% CI, 0.754–0.963) and ECOG PS ≥ 2 vs. 0 (aTR, 0.507; 95% CI, 0.429–0.598); bone metastases (aTR, 0.783; 95% CI, 0.670–0.916); ascites (aTR, 0.744; 95% CI, 0.657–0.841); NLR 4 to <8 vs. <4 (aTR, 0.789; 95% CI, 0.704–0.885) and NLR ≥ 8 vs. <4 (aTR, 0.636; 95% CI, 0.539–0.750; Table S2).
3.7. Comparison of OS by HER2 Status Among Patients Receiving 1L FOLFOX
Median OS was significantly shorter for the 270 patients with HER2-negative disease receiving 1L FOLFOX compared with the 62 patients with HER2-positive disease receiving 1L FOLFOX (10.72 months [95% CI, 9.28–11.55] vs. 16.61 months [95% CI, 11.18–21.09]; p = 0.0009; Figure S1). Patients with HER2-negative disease had significantly shorter OS in the unadjusted AFT model (TR, 0.664; 95% CI, 0.520–0.848; p = 0.0010; Table S3) and after adjusting for confounders (aTR, 0.675; 95% CI, 0.525–0.868; p = 0.0022; Table S4) than patients with HER2-positive disease. In the adjusted AFT model, ECOG PS and NLR were significantly associated with OS. Prognostic factors associated with worse survival included ECOG PS of ≥2 vs. 0 (aTR, 0.619; 95% CI, 0.450–0.852), NLR 4 to < 8 vs. <4 (aTR, 0.731; 95% CI, 0.590–0.905), and NLR ≥8 vs. <4 (aTR, 0.633; 95% CI, 0.477–0.840).
3.8. Comparison of OS by HER2 Status Among Patients Receiving 1L CAPOX
Median OS did not significantly differ between the 228 patients with HER2-negative disease and 98 patients with HER2-positive disease who received 1L CAPOX (11.02 months [95% CI, 8.62–14.44] vs. 13.98 months [95% CI, 11.88–16.09]; p = 0.54; Figure S2). HER2-negative disease was not significantly associated with OS in the unadjusted or adjusted AFT analyses (TR = 0.888; 95% CI, 0.695–1.135; p = 0.34; Tables S5 and S6). In the adjusted AFT model, histological subtype, number of metastatic sites, ECOG PS, and NLR were significantly associated with OS. Prognostic factors associated with shorter OS were diffuse vs. intestinal histological subtype (aTR, 0.631; 95% CI, 0.487–0.817); ≥4 vs. 0–3 metastatic sites (aTR, 0.462; 95% CI, 0.311–0.687); ECOG PS of 1 vs. 0 (aTR, 0.686; 95% CI, 0.523–0.900) and ECOG PS ≥ 2 vs. 0 (aTR, 0.357; 95% CI, 0.238–0.536); NLR 4 to <8 vs. <4 (aTR, 0.609; 95% CI, 0.479–0.773) and NLR ≥ 8 vs. <4 (aTR, 0.642; 95% CI, 0.450–0.915; Table S6).
3.9. Number of Patients with HER2-Negative Disease Eligible for 1L Polychemotherapy
Using PSA, the average estimated number of patients with HER2-negative advanced G/GEJa in Spain who were eligible for 1L polychemotherapy in 2024 was 2856 (95% CI, 1619–4134; Figure S3).
4. Discussion
Advanced G/GEJa is associated with severe symptoms, significant healthcare resource utilization and cost, and poor prognosis, particularly for HER2-negative disease, which lacked targeted therapies before the approval of pembrolizumab and nivolumab for advanced G/GEJa [3,9]. This study aimed to describe the clinical characteristics, treatment patterns, and survival outcomes of patients in Spain with advanced G/GEJa; to compare PFS and OS by HER2 status; and to estimate the number of patients in Spain with HER2-negative advanced G/GEJa who were eligible for 1L polychemotherapy. A majority of patients (56.3%) received only one line of therapy; 27.6% received two lines; and 16.1% received three lines. FOLFOX and CAPOX were the most common 1L regimens from 2017 onward, and paclitaxel alone and paclitaxel in combination with ramucirumab were the most common 2L regimens. Median OS was similar with FOLFOX and CAPOX for patients with HER2-negative G/GEJa (10.72 vs. 11.02, respectively) but was longer with FOLFOX vs. CAPOX for patients with HER2-positive disease (16.61 vs. 13.98, respectively). Median PFS (6.28 months overall) was significantly shorter for patients with HER2-negative vs. HER2-positive disease (5.92 vs. 7.37 months). Median OS (11.05 months overall) was also significantly shorter for patients with HER2-negative vs. HER2-positive disease (10.49 vs. 13.82 months). In adjusted models for all 1L treatment regimens, prognostic factors associated with worse OS included HER2-negative vs. HER2-positive status; diffuse vs. intestinal histological subtype; ≥4 vs. 0–3 metastatic sites; ECOG PS of 1 or ≥2 vs. 0; bone metastases; ascites; NLR 4 to <8 vs. <4; and NLR ≥ 8 vs. <4.
In this cohort of patients, most had de novo disease, a low ECOG PS (0–1), and a low NLR (<4). Over half of patients in this study received only 1L treatment, perhaps reflecting delayed diagnosis and poor prognosis [36,37]. The emergence of FOLFOX and CAPOX as the most common 1L chemotherapy regimens between 2015 and 2019 is consistent with the European Society for Medical Oncology (ESMO) guidelines for gastric cancer, which recommend platinum-fluoropyrimidine doublet chemotherapy for 1L treatment of advanced G/GEJa [36]. Paclitaxel alone and paclitaxel in combination with ramucirumab as the most common 2L treatments also aligns with the most recent ESMO guidelines [36,38].
Consistent with previous estimates that approximately three-quarters of advanced G/GEJa cases are HER2-negative [10,26], 70.1% of patients in this study had HER2-negative disease. Compared with patients with HER2-positive disease, patients with HER2-negative disease were slightly younger and less likely to be male. They were also more likely to have primary gastric (vs. GEJ) tumors with diffuse (vs. intestinal) histology. Male predominance of HER2-positive gastric cancer has been noted previously [39,40,41], as have associations between HER2 overexpression and older age, GEJ primary tumor site, and intestinal histology [10,41,42].
The observed differences in survival between HER2-positive and HER2-negative subgroups (i.e., significantly shorter PFS and OS in patients with HER2-negative disease, and significantly shorter OS after adjusting for confounders in patients with HER2-negative disease, including those receiving 1L FOLFOX) may be mainly attributed to the lack of targeted therapies for patients with HER2-negative disease in the 1L setting during the time period studied (2015–2021). HER2 is a transmembrane receptor tyrosine kinase that is activated by heterodimerization with other members of the human epidermal growth factor receptor family, initiating signal transduction pathways that stimulate proliferation, differentiation, and survival of tumor cells [43]. Targeted therapy for HER2-positive disease, including antibodies that inhibit HER2-mediated signaling by reducing HER2 receptor expression or dimerization (e.g., trastuzumab, which was received by 92.7% of patients with HER2-positive disease as part of their 1L treatment regimen), has contributed to improved survival in that population [13,43]. The differences between HER2-positive and HER2-negative populations may increase further with the advent of trastuzumab deruxtecan [15,16].
In 2021, the immune checkpoint inhibitors nivolumab and pembrolizumab were approved in Europe for 1L treatment of adults with HER2-negative advanced or metastatic gastric, GEJ, or esophageal adenocarcinoma whose tumors express PD-L1 with a CPS ≥ 5 for nivolumab and ≥10 for pembrolizumab [21,22]. The approval for pembrolizumab was updated in 2023 to allow a CPS ≥ 1 [44]; however, in Spain, pembrolizumab financing is restricted to patients whose tumors express PD-L1 with a CPS ≥ 10 [45]. There remains an unmet need for personalized targeted therapy to improve survival outcomes in patients with HER2-negative G/GEJa [36], as not all G/GEJa tumors express PD-L1 [23,24,25] or enough PD-L1 to receive financing (CPS ≥ 5 for nivolumab or CPS ≥ 10 for pembrolizumab in Spain [46]). Furthermore, the estimated 2856 patients with HER2-negative advanced G/GEJa in Spain who were eligible for 1L treatment with polychemotherapy in 2024 represent a substantial proportion of the total number of new cases of G/GEJ cancer in Spain in 2024 (6868 patients), underscoring this unmet need.
This study has several strengths. It is a large-scale, real-world study based on the AGAMENON-SEOM registry database, with broad representation of regions across Spain. The study design allowed for each patient to have at least 2 years of follow-up. The data reflect evolving trends in contemporary disease management over recent years, including shifts in polychemotherapy regimens. Altogether, the study provides detailed, up-to-date information on a large cohort of patients with advanced G/GEJa in Spain.
This study also has limitations. First, the treatment landscape has changed markedly since the introduction of immunotherapies and later treatment lines in HER2-positive disease (trastuzumab deruxtecan). Second, it is retrospective and therefore subject to potential for bias and missing information. Third, it is not a population-based study because the AGAMENON-SEOM registry only includes centers that opt to participate. Access to 2L and 3L treatment may have been limited in some centers. Fourth, there was a minority of patients (6.7%) whose HER2 status was unknown. Fifth, it is not known how many of the patients receiving polychemotherapy would also be suitable for new agents combined with polychemotherapy. When estimating the number of patients with HER2-negative advanced G/GEJa who were eligible for 1L polychemotherapy, there was no single data source representative of patients in Spain with HER2-negative advanced G/GEJa that included all of the required parameters; therefore, multiple sources of data were used for this estimation. To address this limitation, PSA was used to quantify the uncertainty of each parameter and estimate the number of eligible patients.
5. Conclusions
This study is based on a robust analysis of the largest cohort of patients with advanced G/GEJa in Spain, describing clinical characteristics, treatment patterns, and survival outcomes. Comparisons of PFS and OS between patients with HER2-negative and HER2-positive disease provide further evidence that there is a treatment gap for HER2-negative disease, which represents the majority (approximately three-quarters [10,26]) of advanced G/GEJa cases. Irrespective of HER2 status, the aggressiveness of this disease is apparent in the minority of patients who receive subsequent lines of therapy beyond 1L treatment. More effective treatments are critically needed. Findings from this study may help inform new healthcare policies and spur further research toward improving disease management and treatment outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Allemani C. Matsuda T. Di Carlo V. Harewood R. Matz M. Niksic M. Bonaventure A. Valkov M. Johnson C.J. Esteve J. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries Lancet 20183911023107510.1016/S 0140-6736(17)33326-329395269 PMC 5879496 · doi ↗ · pubmed ↗
- 3Gil-Delgado M.A. Lucidarme O. Bachet J.B. Mahi N. Khayat D. Long-term survival in gastroesophageal junction adenocarcinoma: Ramucirumab Case Rep. Gastroenterol.20181253253910.1159/00049090630283289 PMC 6167727 · doi ↗ · pubmed ↗
- 4Gallego Plazas J. Arias-Martinez A. Lecumberri A. Martinez de Castro E. Custodio A. Cano J.M. Hernandez R. Montes A.F. Macias I. Pieras-Lopez A. Sex and gender disparities in patients with advanced gastroesophageal adenocarcinoma: Data from the AGAMENON-SEOM registry ESMO Open 2022710051410.1016/j.esmoop.2022.10051435714478 PMC 9271495 · doi ↗ · pubmed ↗
- 5Agarwal S. Bell M.G. Dhaliwal L. Codipilly D.C. Dierkhising R.A. Lansing R. Gibbons E.E. Leggett C.L. Kisiel J.B. Iyer P.G. Population based time trends in the epidemiology and mortality of gastroesophageal junction and esophageal adenocarcinoma Dig. Dis. Sci.20246924625310.1007/s 10620-023-08126-637914889 PMC 10926253 · doi ↗ · pubmed ↗
- 6Buas M.F. Vaughan T.L. Epidemiology and risk factors for gastroesophageal junction tumors: Understanding the rising incidence of this disease Semin. Radiat. Oncol.2013233910.1016/j.semradonc.2012.09.00823207041 PMC 3535292 · doi ↗ · pubmed ↗
- 7Spanish Society of Medical Oncology (SEOM) Las Cifras del Cáncer en España [Cancer Figures in Spain] 2021 Available online: https://seom.org/images/Cifras_del_cancer_en_Espnaha_2021.pdf(accessed on 21 April 2025)
- 8Guevara M. Molinuevo A. Salmeron D. Marcos-Gragera R. Carulla M. Chirlaque M.D. Rodriguez Camblor M. Aleman A. Rojas D. Vizcaino Batlles A. Cancer survival in adults in Spain: A population-based study of the Spanish network of cancer registries (REDECAN)Cancers 202214244110.3390/cancers 1410244135626046 PMC 9139549 · doi ↗ · pubmed ↗