Multi-Detector Helical Computed Tomography, Transrectal Ultrasonography, and Histology of the Sacroiliac Joint: A Comparative Study in Adult Warmblood Horse Cadavers
Rebecca A. Mathys, Thomas R. Schmitz, Hans Geyer, Nicole Borel, Monika Hilbe, Stefanie Ohlerth, Andrea S. Bischofberger

TL;DR
This study compared imaging techniques and histology in horse sacroiliac joints, finding common structural changes that may be part of normal aging or training adaptation.
Contribution
The study provides a comparative analysis of transrectal ultrasonography, CT, and histology in equine sacroiliac joints, revealing correlations between imaging and degenerative changes.
Findings
Computed tomography showed abnormalities in all 25 joints, with the most severe changes in the caudal third.
Histological analysis confirmed degenerative changes in cartilage, subchondral bone, and joint capsule.
Strong correlations were found between CT findings and histology, but not between ultrasound and CT grades.
Abstract
Sacroiliac joint (SIJ) disease is a common cause of poor performance in horses, but diagnosis is challenging due to the joint’s deep anatomical location. A common diagnostic method is transrectal ultrasound and nuclear scintigraphy. Newer techniques, such as computed tomography, may provide a more complete evaluation, but their diagnostic value in assessing the sacroiliac joint in horses is still unclear. This study evaluated 25 sacroiliac joints of 15 adult Warmblood horses without reported pain using post-mortem transrectal ultrasonography, computed tomography, and histological examination. All joints showed structural changes on computed tomography, and most also presented abnormalities on ultrasonography. The most severe changes were observed in the caudal third of the joint, which is the region accessible by transrectal ultrasonography. Histological analysis revealed degenerative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
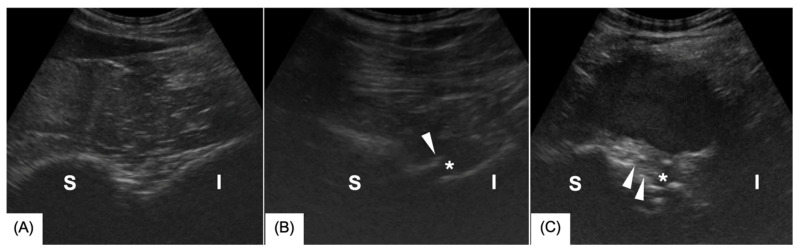 Figure 1
Figure 1 Figure 2
Figure 2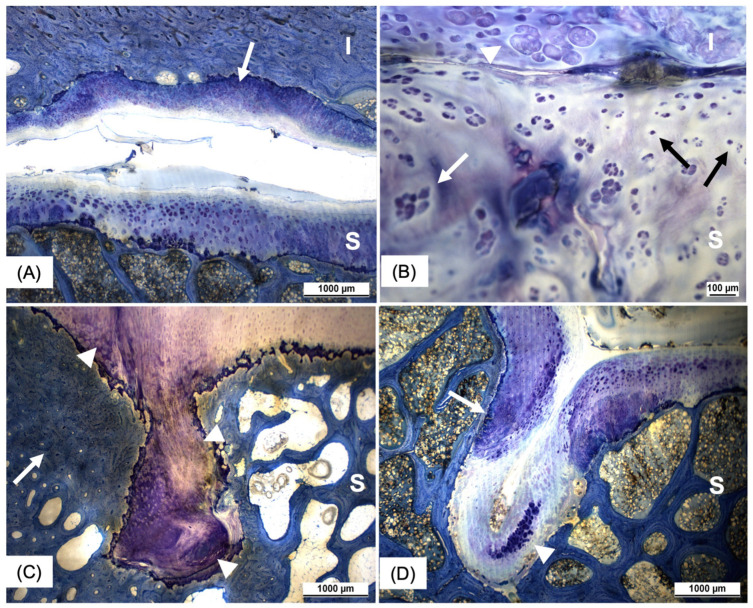 Figure 3
Figure 3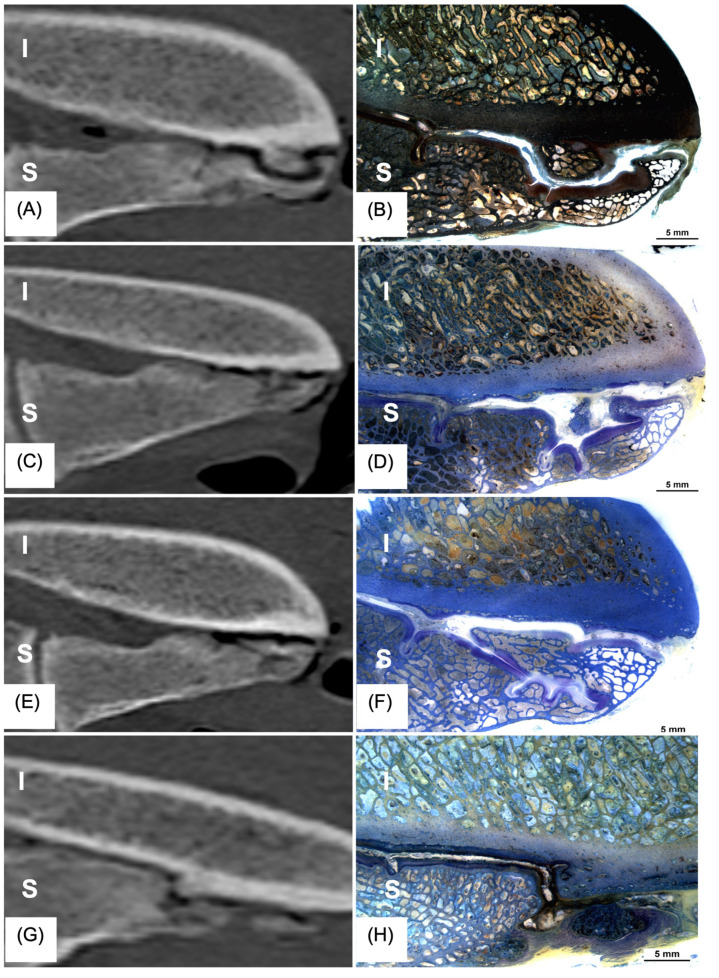 Figure 4
Figure 4- —Loriot Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVeterinary Equine Medical Research · Spine and Intervertebral Disc Pathology · Shoulder Injury and Treatment
1. Introduction
Sacroiliac joint (SIJ) disease is a common cause of poor performance in sport horses [1,2,3]. Dressage and show jumping horses in particular are at a higher risk of developing SIJ disease than horses in other disciplines [1]. Diagnosing SIJ pain can be challenging [4]. A thorough orthopedic examination including SIJ anesthesia is key to rule out other conditions resulting in similar clinical presentations, such as thoracolumbar pain, lumbosacral pain, and mild hind limb lameness of other origins, such as proximal suspensory desmopathy or mild ataxia [1,2,3].
Diagnostic imaging of the SIJ and surrounding structures includes nuclear scintigraphy or transrectal ultrasonography [5,6,7,8,9,10]. The sensitivity and specificity of nuclear scintigraphy for diagnosing SIJ pain were found to be 51% and 77%, respectively [11]. The ultrasonographic evaluation protocol of the normal SIJ, staging of disease severity, and its imaging features have previously been reported [10,12,13,14,15,16]. Albeit being fast and cheap, evaluation of the SIJ via transrectal ultrasonography is limited to the caudoventral aspect of the joint, raising the question of whether pathologic changes in the dorsolateral aspect of the joint remain underdiagnosed [15]. So far, there is only limited information available on the correlation of ultrasonographic changes of the SIJ with other diagnostic imaging modalities.
In human medicine, computed tomography (CT) is a frequently used imaging modality for patients experiencing pain in the lumbosacroiliac region [17]. Recent studies in dogs have established CT as a sensitive modality to detect degenerative SIJ [18,19,20]. Good anatomical detail was shown when the equine lumbosacral region was examined with CT in living patients and cadavers [13,21,22]. With the development of newer, large-bore CT units, examination of the SIJ in horses under general anesthesia is becoming a feasible diagnostic option.
The equine SIJ is a tight joint (amphiarthrosis) and lies at an approximately 30° angle from the horizontal plane between the first sacral transverse process and the wing of the ilium [23]. The main functions of the SIJ are the fixation of the sacrum between the wing of the ilium and the transmission of propulsive forces from the hind limbs to the trunk [24]. The SIJ has been described as an atypical synovial joint because the sacral joint surface appears to be covered with hyaline cartilage, whereas the iliac joint surface is covered with fibrocartilage [4,23,25,26]. The joint is enclosed by a joint capsule closely adjacent to the articular surface and is supported by three sacroiliac ligaments [4,27]. When horses show chronic poor performance and pain that has been localized to the lumbosacroiliac region using infiltration with local anesthetic solution, distinct histological abnormalities in nerve sections and macroscopic osseous variations in the sacral and lumbar regions can be observed [28]. These findings highlight the importance of correlating clinical signs with the underlying histopathological changes associated with SIJ disease in horses.
Currently, there are no comparative reports between the CT changes of the equine SIJ with other diagnostic modalities, such as transrectal ultrasonography and histology. The objectives of this study were to describe, grade, and correlate transrectal ultrasonographic, CT, and histological findings of the SIJs in Warmblood horse cadavers. We hypothesized that SIJ changes are common in Warmblood horses without reported clinical signs of SIJ disease before euthanasia, and that sacroiliac joint changes detected by computed tomography (CT) would exhibit a strong correlation with findings obtained through transrectal ultrasonography. Additionally, we postulated that horses exhibiting SIJ alterations detectable through imaging modalities (CT and/or ultrasonography) would also present corresponding histopathological changes.
2. Materials and Methods
Warmblood horses aged 5–18 years (mean age: 12.3 ± 3.81 years) that were euthanized or slaughtered for reasons unrelated to the study were included in the investigation following owners’ consent at the Equine Hospital, University of Zurich between September 2021 and May 2023. All horses had been regularly used as riding horses in their respective disciplines and, according to the owner or trainers, exhibited no clinical signs indicative of SIJ disease.
2.1. Diagnostic Imaging
Immediately after euthanasia or slaughter, a transrectal ultrasonographic examination was performed using a curvilinear probe (Hitachi-Aloka ProSound Alpha 7, Hitachi Healthcare, Tokyo, Japan) with the horse positioned in left lateral recumbency. The ultrasonographic examination was conducted by an ECVS diplomate in training as a large animal diagnostic imaging resident (3rd year) or an ECVDI-certified radiologist and adhered to a previously published protocol [12]. The images were graded according to Tallaj et al. [10]. Briefly, the following criteria were evaluated in all joints (n = 25): articular margins (osteophyte formation), modeling (shape change) of the sacrum and ilium, ventral sacroiliac ligament changes, enthesophyte formation, and joint effusion (see Table 1). Findings were graded on a scale from 0 to 3, whereby 0 represented no abnormal findings, 1 represented mild, 2 represented moderate, and 3 represented severe findings (Figure 1A–C). In the end, an overall mean score was given for each joint. Grade 0 was given for normal joints, and Grade 1 was assigned if one or more criteria were mild. If at least one criterion was moderate, Grade 2 was given. Grade 3 was assigned if one or more criteria were graded as severe.
Within one to four hours following death, the abdominal and pelvic organs were removed. The pelvis was isolated cranially by disarticulation between the 3rd and 4th lumbar vertebrae, caudally by osteotomy at the first caudal vertebra, and distally in the mid-femur region. To facilitate specimen handling and reduce CT-artifacts, such as streaking and image noise, the pelvis was bisected through the symphysis, the midline of the sacrum, and the vertebral canal using a bone saw. This approach further enabled the precise positioning of each sacroiliac joint within the isocenter of the CT gantry. The specimens were subsequently frozen at −28 °C until diagnostic imaging was performed. Before CT imaging, they were slowly thawed in warm water for 24–48 h.
All CT images were obtained using a multidetector 160-slice (dual) 80-slice scanner (Canon Aquilion Exceed LB, Canon Medical Systems AG Corporation, Wallisellen, Switzerland.) in a helical acquisition mode, with a pitch of 35.9 (pitch factor 0.898), 135 kV, 530 mAs, a field of view of 700 mm, and a matrix of 256 × 256. Images were reconstructed in a bone and soft tissue algorithm with a slice thickness of 1 mm.
An ECVDI-certified radiologist (S.O.) and an ECVS diplomate training as a large animal diagnostic imaging resident (3rd year) (A.B.) reviewed all CT images. The SIJ length was measured once in the frontal plane at its maximal extent. This measurement was divided into three thirds. The caudal third of the SIJ as well as the complete SIJ were then evaluated and graded separately. The grading was adapted from Wise et al. [20]. Briefly, the CT criteria included osteophyte formation, periarticular modeling (enthesophyte formation), subchondral bone sclerosis, subchondral bone lesions, and sacrum/ilium modeling (shape change). Each criterion was assigned a severity grade: 0 = none, 1 = mild, 2 = moderate, and 3 = severe (Table 2). An overall mean score was calculated for the caudal third and the complete SIJ. Additionally, the most severe findings in each joint were localized to either the caudal, middle, or cranial third of the joint.
2.2. Histological Examination
Before the main study, sampling and histological processing were tested on a pilot cadaver. SIJ histology was performed on 11 randomly chosen SIJs following the CT examination. All muscles were removed from the pelvic halves. The SIJ, together with the lumbosacral and intertransverse joints, was sectioned into three blocks, each measuring 10 cm in length, 4 cm in width, and 6 cm in height, using a bone saw. The blocks were fixed in a buffered solution containing 2.5% glutaraldehyde and 1.3% formaldehyde (Fluka Chemie GmbH, Buchs, Switzerland). The fixation process lasted one week, during which a shaker was used to enhance the infiltration of the fixative. The fixed blocks were dehydrated in ethanol (Fluka Chemie GmbH, Buchs, Switzerland) and subsequently infiltrated and embedded in methyl methacrylate (MMA) (Brunschwig AG, Supplies for Laboratory and Production, Basel, Switzerland). The entire infiltration and embedding process required 12 weeks to complete. The MMA blocks were sectioned sagittally every 2 mm using a diamond-coated band saw (Haslab GmbH, Labor und Medizintechnik, Ostermundigen, Switzerland). The resulting cuts typically measured 1.2 mm in thickness and were subsequently bonded to a polyacrylic plate. The sections were ground to a thickness of 300–500 μm using a Leica SP 2600 milling machine (Leica Microsystems Schweiz AG, Glattbrugg, Switzerland). Staining was performed using either Giemsa or van Kossa/McNeal techniques. The van Kossa/McNeal staining technique was utilized to examine the subchondral bone and to detect calcifications in the articular cartilage associated with degenerative changes. Four authors (H.G., N.B., M.H., and R.M.) examined the stained slides with a Leica stereomicroscope, a Leica DMR microscope, and a Leica IM 1000 image manager (Leica Microsystems Schweiz AG, Glattbrugg, Switzerland). The sections were examined for the presence and distribution of hyaline cartilage and fibrous cartilage in the sacroiliac joint. The thickness of the cartilage and subchondral bone was measured using an image manager (Leica Microsystems Schweiz AG, Glattbrugg, Switzerland). The maximum thickness, minimum thickness, and corresponding mean thickness values were determined. In addition, the presence of degenerative changes within the articular cartilage, subchondral bone plate, and joint capsule of the SIJ were thoroughly assessed. These changes were graded according to a grading system modified by Mcllwraith et al. [29] (Table 3). Each histological section of the respective joint was graded individually, with the sacral and iliac joint surfaces assessed separately. A mean score for each joint was then calculated by averaging the scores of all its histological sections. The histological changes were then categorized as mild (score 1–9/26), moderate (score 10–18/26), or severe (score 19–26/26).
2.3. Statistical Analysis
Data were stored in Microsoft Excel program (Microsoft Excel for Mac 2024, version 16.87, Redmond, WA, USA). All statistical analyses were performed with SPSS 29 statistical software (IBM SPSS Statistics, Chicago, IL, USA). Data distribution was tested with a Kolmogorov–Smirnov test. A p-value of <0.05 was considered statistically significant. The Spearman’s rank correlation coefficient was calculated to evaluate the correlation between the overall scores of the ultrasonographic and CT findings, and between imaging modalities and histology. A paired t-test was used to compare the subchondral bone thickness and the cartilage thickness between the ilium and sacrum.
3. Results
A total of 15 Warmblood horses were included for imaging examination. In total, 25 sacroiliac joints (SIJ) provided images of sufficient quality for evaluation. Reasons for euthanasia or slaughter included blindness (n = 1), acute severe neurological signs (n = 2), severe acute laminitis (n = 3), behavioral issues (n = 2), colic (n = 4), headshaking (n = 2), and acute superficial flexor tendon rupture (n = 1). The horses had been used for show jumping (n = 7), dressage (n = 2), or pleasure riding (n = 6). Histological examination was performed on 11 randomly chosen SIJs.
3.1. Ultrasonography
The ultrasonographic examination revealed abnormal findings in 92% of the sacroiliac joints. Among these, 40% exhibited mild findings, 44% displayed moderate findings, and 8% were classified as severe findings (Figure 1A–C). The most common ultrasonographic findings were osteophytes (92%), effusion (76%), and sacral/iliac bone modeling (76%). Enthesophytes were observed in 68% of the cases, while alterations in the ventral sacroiliac ligament were detected in 52%.
3.2. CT
All (100%) SIJs exhibited abnormal findings on CT examination. Consistent with ultrasonographic results, 44% of the joints showed mild changes, 48% demonstrated moderate changes, and 8% were classified as having severe changes. The most prevalent CT findings in the SIJ included osteophytes (92% in the caudal third and 100% in the entire SIJ), sclerosis (72% and 88%, respectively), subchondral bone lesions (60% and 88%, respectively), and enthesophytes (60% and 68%, respectively). Among the CT scans, the most severe changes were located in the caudal third of the joint in 44% of cases (11/25), in the middle third in 16% (4/25) and the cranial third in 24% (6/25). In the remaining SIJs (4/25, 16%), the most severe lesions could not be assigned to a specific area within the SIJ. While reviewing the CT images, we largely found two different types of changes: either primary subchondral bone changes, such as subchondral cyst-like lesions with associated subchondral bone thickening, and sclerosis or periarticular new bone formation bridging the cranial and caudal aspects of the SIJ (referred to as ventral buttressing).
3.3. Histology
The sagittal thick sections obtained in this study provided an excellent depiction of the anatomy of the equine SIJ. In the sections involving the SIJ, the joint with the sacral and iliac joint surfaces and the corresponding subchondral bone plates, the joint capsule (especially at the caudal joint margin), and often parts of the ventral and interosseous sacroiliac ligaments were histologically assessable.
In terms of cartilage distribution, the iliac articular surface was peripherally composed of fibrocartilage, while a combination of hyaline and fibrocartilage was evident in the center of the joint surface (Figure 2 and Figure 3A). The sacral articular surface was covered by fibrocartilage at the cranial, lateral, and medial joint margins, whereas the caudal margin and the center were covered by hyaline cartilage. The mean cartilage thickness on the sacrum (1.19 ± 0.29 mm) was significantly thicker than on the ilium (0.86 ± 0.19 mm), (p < 0.001). In contrast to that, the subchondral bone of the ilium (2.74 ± 0.85 mm) was significantly thicker compared to the subchondral bone of the sacrum (0.51 ± 0.22 mm), (p < 0.001) (Figure 3A). The most frequently observed histological findings are summarized in Table 4. The occurrence of chondrocyte group formation, both with and without hypertrophy (Figure 3B,D), hypertrophy in the absence of group formation, tidemark perforation, pyknotic chondrocytes (Figure 3B), and subchondral bone sclerosis (Figure 3C) was significantly more prevalent in the sacral joint surface compared to in the iliac joint surface. When all histological criteria applied were summarized in a total score, the majority of SIJ (90.9%) had mild changes, 9.1% of SIJ had moderate changes, and none of the SIJ showed severe changes.
3.4. Correlation Between Imaging Modalities (CT, US) and Histology
A non-significant correlation was found when comparing the mean overall ultrasonographic grade with the CT grade of the entire SIJ (p = 0.087, correlation coefficient r_s_: 0.35, n = 25) or the caudal part of the SIJ (p = 0.15, correlation coefficient r_s_: 0.29, n = 25). The CT changes in the caudal third of the SIJ strongly and significantly correlated with the changes of the entire SIJ (p < 0.001, correlation coefficient = 0.918, n = 25). When enthesophytes were evaluated separately, a high correlation between the ultrasonography and CT was detected (p < 0.001; correlation coefficient r_s_: 0.728, n = 25).
The histological grades of the SIJ strongly and significantly correlated with the overall CT grade (p = 0.011, correlation coefficient r_s_: 0.731, n = 11) (Figure 4A–F) and with the ultrasonographic grade (p = 0.024, correlation coefficient r_s_: 0.670, n = 11). This indicates that if horses exhibit alterations in the SIJ on CT and/or ultrasonography, they are likely to exhibit corresponding degenerative changes histologically (Figure 4A–F).
4. Discussion
This study aimed at describing, grading, and associating transrectal imaging and histological findings of SIJs of Warmblood horse cadavers with the hypothesis that SIJ changes are common in Warmblood horses. This assumption was correct because, although the degree ranged from mild to moderate, all equine SIJs showed abnormal CT findings, and 92% showed abnormal ultrasonographic findings. The CT characteristics of degenerative joint disease previously reported in humans [30] and dogs [18] were also detectable in our study population. This high prevalence of abnormal CT findings is consistent with the human literature, where degenerative changes of the SIJ in CT of asymptomatic humans are as frequent as the changes seen in patients with lower back pain [17]. In our study, the prevalence of the ultrasonographic findings was also high (92%). This is in line with the high prevalence of CT findings. A study evaluating 296 horses with a positive response to local infiltration of anesthetic solution in the SIJ region and abnormal radiopharmaceutical uptake on scintigraphy reported a substantially lower prevalence of ultrasonographic abnormalities within the SIJ (32%) [2]. A possible explanation for this discrepancy is that the ultrasonographic evaluation criteria were different. In Barstow et al., only SIJ modeling was assessed as a single abnormal joint-related criterion. In our study, multiple SIJ criteria were included, which may have resulted in stricter analysis and a larger number of joints being classified as having findings.
In horses, a high prevalence of macroscopic SIJ changes was observed in both healthy individuals and clinically affected horses based on pain localized to the SIJ using diagnostic anesthesia [3,23,28,31]. This indicates that adaptative modeling of the SIJ is likely depending on a horse’s conformation, posture, and use. Differentiating between normal adaptative changes and clinically relevant changes remains difficult. In human medicine, age-dependent clinically relevant imaging findings were only determined through a comparison of changes observed in clinically affected patients with sacroiliitis and those in asymptomatic individuals [30,32,33]. One study did not show any differences in gross-pathological changes in clinically symptomatic horses localized to the SIJ and control horses [28]. However, future studies comparing the diagnostic imaging findings in asymptomatic and symptomatic horses are essential to elucidate the clinical relevance of these findings. A close correlation of the diagnostic imaging findings with the results of the orthopedic examination as well as local anesthesia of the SIJ is imperative.
The alterations identified through ultrasonography and CT demonstrated a moderate, albeit non-significant, correlation. Thus, SIJ ultrasonographic findings are not directly representative of CT changes, and vice versa. Therefore, the second hypothesis, suggesting a strong correlation between ultrasound and CT findings, could not be accepted. A possible reason for this discrepancy is that the evaluation criteria of the modalities were not identical. A recent CT study of clinical cases also found that suspected lesions in the lumbosacroiliac region identified by ultrasound could not be confirmed by CT [34]. However, the observed weak positive correlation between CT and ultrasonographic findings could suggest a possible trend that might become significant with a larger sample size.
No significant differences were observed in the overall degree of CT changes between the caudal third of the SIJ and the overall degree of changes in the entire joint. However, consistent with previous reports [23,31], the most severe CT changes were localized in the caudal third of the SIJ. Therefore, the sole examination of the caudal third of the joint by transrectal ultrasonography should depict the most severe joint pathology in nearly half of the horses (44%). In cases refractory to treatment or exhibiting unusual clinical signs, both modalities should be used in a complementary fashion. Furthermore, pain from structures adjacent to the sacroiliac joint should be considered as a differential diagnosis. As local anesthetic solution may diffuse beyond the joint, sacroiliac analgesia is not necessarily specific, and surrounding regions should be carefully evaluated [35].
The buttressing changes observed in our study have previously been reported in the literature [3,31,34]. In 1999, Haussler et al. described periarticular new bone formation in racehorse specimens in which no clinical signs of SIJ pathology had been recognized, consistent with the buttress-type lesions observed in the present study [31]. In contrast, in horses with suspected SIJ disease, the joint surface is enlarged due to bony outgrowths along the margins, which may resemble the same lesion type [3,31]. Consequently, it remains unclear whether this type of finding has any clinical relevance.
Former studies describe that the equine articular surface of the sacrum is covered by hyaline cartilage and the auricular surface of the ilium by fibrocartilage [4,23,36]. This study shows contradictory results: hyaline cartilage was not only present in the articular surface of the sacrum but also in the central aspect of the articular surface of the ilium. Thus, this work confirms the presence of fibrocartilage and hyaline cartilage on both articular surfaces of the SIJ. Chondrocyte group formation with and without hypertrophy, the presence of pyknotic chondrocytes as well as a vascular perforation of the tide mark were histologically the most prevalent findings within the articular cartilage. Histological signs of joint degeneration within the SIJ were previously reported to occur with high prevalence in the articular cartilage of horses older than four years [36].
In human medicine, the presence of hypertrophic chondrocytes in cartilage without endochondral ossification is considered a definitive sign of osteoarthritis, as the shift of chondrocytes to a hypertrophic phenotype induces a series of events leading to articular cartilage degeneration [37,38]. In horses, endochondral ossification in the SIJ is complete by the age of four years [36]. All horses included in this study were older than four years. Consequently, the presence of hypertrophic chondrocytes in these horses can be considered a sign indicative of articular cartilage degeneration in the context of osteoarthritis. Whether these degenerative changes have current or future clinical relevance remains unclear. Currently, no imaging modality enables the direct evaluation of articular cartilage at the SIJ. However, this study demonstrated that when CT and/or ultrasonography reveal alterations in the SIJ, the articular cartilage also exhibits histological signs of joint degeneration. Thus, the third hypothesis of the study, proposing that horses with findings in the imaging procedures also show histological signs of joint degeneration, can be confirmed. Nevertheless, when the histological changes in the joints were considered collectively in the form of a total score, they were mostly categorized as mild. This may suggest that the frequently observed histological findings are not necessarily degenerative changes associated with osteoarthritis, but rather adaptative changes of the bone and cartilage to facilitate the intensive transmission of forces from the hindlimbs to the spine. In this context, cartilage cell hypertrophy could represent a response to increased cellular abrasion on the joint surface, which, during loading, must withstand high pressure on the small, closely opposing cartilage surfaces.
Most of the histological changes in the articular cartilage and subchondral bone were significantly more prevalent on the sacral articular surface compared to the iliac articular surface.
Previous post-mortem studies in the horse revealed a high prevalence of macroscopic visible degenerative changes on both joint surfaces (100% in the sacrum and 72% in the ilium) [31,39,40]. These changes were not only more frequent but also exhibited greater severity on the sacral joint surface [31]. In contrast, osteophytes identified within the SIJ on post-mortem CT images appeared to be symmetrically distributed across both joint surfaces [21]. The observed differences in the extent of degenerative changes between the iliac and sacral joint surfaces may be explained by variations in the mechanical forces acting on each bone. Haussler et al. reported subtle, independent motion patterns of the ilium and sacrum, suggesting that these structures may not experience identical mechanical loading [41]. It has been postulated that shear forces predominantly influence the SIJ, as opposed to compressive forces, resulting in diminished synovial turnover and, consequently, impaired nourishment of the articular cartilage [23]. This impaired cartilage nutrition could also contribute to the high prevalence of degenerative changes observed within the equine sacroiliac joint.
The most significant limitation of the study was the absence of a thorough lameness examination by an experienced clinician familiar with the clinical signs indicative of SIJ disease conducted before the horse’s death. Theoretically, horses with early stages of SIJ disease with only mild clinical signs which may have been missed by the owners could have been included in the study. All horses were used at their original riding level before being presented to the clinic for euthanasia/slaughter, and they did not show any reported evidence of clinical signs typical of SIJ disease. Nevertheless, it should be noted that a previous study demonstrated that approximately 50% of horses considered riding sound by the owner exhibited lameness when evaluated at the trot [42]. However, no clinical signs attributable to early SIJ disease have been described to date, which is why these cases could also have been missed during an orthopedic examination.
Due to the absence of horses without CT-detectable lesions, test characteristics such as specificity and negative predictive value of ultrasonography relative to CT could not be calculated. This represents a limitation of the study.
For ethical reasons, the imaging modalities were only carried out postmortem. This inevitably led to minor gas artifacts within the vasculature overlying the SIJ on ultrasonography. This was most pronounced when horses were slaughtered due to gas entering the common carotid artery when it was severed. The CT quality was not affected by the gas artifacts. Furthermore, CT scans of living horses under general anesthesia may demonstrate reduced spatial resolution compared to cadaveric studies due to the increased anatomical mass [22] and motion artifacts. Similarly, ultrasound examination in live horses can be more challenging than post-mortem imaging because of muscle contractions, large blood vessels, etc. Therefore, the results of this study should not be directly extrapolated to clinical cases.
5. Conclusions
SIJ findings in CT, ultrasonography, and histology are very common in adult Warmblood horses without owner-perceived clinical signs indicating SIJ disease. These may represent adaptative to early maladaptive joint modeling. Future studies investigating the clinical relevance of these findings and/or the pattern of changes in horses presenting with clinical symptoms represent the next step in advancing this research. The findings of the ultrasonographic and CT examinations showed non-significant correlations, which is likely due to the criteria evaluated. The overall CT findings in the caudal third of the SIJ did not significantly differ from those present in the entire joint. Additionally, the most severe CT lesions were most frequently located in the caudal third, further supporting the diagnostic relevance of this region, assessable by ultrasonography. In horses exhibiting alterations in the SIJ detected by CT and/or ultrasonography, corresponding degenerative changes of the articular cartilage by histology can be expected.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dyson S. Murray R. Pain associated with the sacroiliac joint region: A clinical study of 74 horses Equine Vet. J.20033524024510.2746/04251640377614825512755425 · doi ↗ · pubmed ↗
- 2Barstow A. Dyson S. Clinical features and diagnosis of sacroiliac joint region pain in 296 horses: 2004-2014 Equine Vet. Educ.20152763764710.1111/eve.12377 · doi ↗
- 3Jeffcott L.B. Dalin G. Ekman S. Olsson S.E. Sacroiliac lesions as a cause of chronic poor performance in competitive horses Equine Vet. J.19851711111810.1111/j.2042-3306.1985.tb 02063.x 3987658 · doi ↗ · pubmed ↗
- 4Haussler K.K. Functional Anatomy and Pathophysiology of Sacroiliac Joint Disease Proc. Annu. Conv. Am. Assoc. Equine Pract.200450361366
- 5Gorgas D. Kircher P. Doherr M.G. Ueltschi G. Lang J. Radiographic technique and anatomy of the equine sacroiliac region Vet. Radiol. Ultrasound 20074850150610.1111/j.1740-8261.2007.00287.x 18018720 · doi ↗ · pubmed ↗
- 6Gorgas D. Luder P. Lang J. Doherr M.G. Ueltschi G. Kircher P. Scintigraphic and radiographic appearance of the sacroiliac region in horses with gait abnormalities or poor performance Vet. Radiol. Ultrasound 20095020821410.1111/j.1740-8261.2009.01519.x 19400471 · doi ↗ · pubmed ↗
- 7Erichsen C. Berger M. Eksell P. The scintigraphic anatomy of the equine sacroiliac joint Vet. Radiol. Ultrasound 20024328729210.1111/j.1740-8261.2002.tb 01005.x 12088326 · doi ↗ · pubmed ↗
- 8Erichsen C. Eksell P. Widstrom C. Berger M. Holm K.R. Johnston C. Scintigraphy of the sacroiliac joint region in asymptomatic riding horses: Scintigraphic appearance and evaluation of method Vet. Radiol. Ultrasound 20034469970610.1111/j.1740-8261.2003.tb 00534.x 14703254 · doi ↗ · pubmed ↗