Treatment Outcomes of Squamous Cell Carcinoma of the Soft Palate and the Prognostic Significance of HPV/p16 Status
Meng‐hua Li, Xing Zhang, Feng‐jiao Li, Xian‐lu Gao, Shi‐da Yan, Qiao‐hong Lin, Xi‐yuan Li, Jian Meng, Ying Zhang, Shi‐ting Zhang, Shu‐wei Chen, Ming Song

TL;DR
This study finds that surgery improves survival for early-stage soft palate cancer, and HPV status does not affect prognosis.
Contribution
Identifies primary surgery as a better treatment for early-stage SCCSP and shows HPV/p16 status is not a prognostic marker.
Findings
Primary surgery improves progression-free, overall, and disease-specific survival in early-stage SCCSP.
HPV/p16 status does not significantly affect survival outcomes in SCCSP patients.
Multivariate analysis confirms surgery's independent benefit for early-stage SCCSP.
Abstract
Squamous cell carcinoma of the soft palate (SCCSP) represents a rare subtype of oropharyngeal cancer. This study aims to evaluate the treatment outcomes of SCCSP and to assess the prognostic significance of HPV status. Patients diagnosed with SCCSP between January 1981 and December 2021 were collected. Survival outcomes were compared. In univariate analysis, primary surgery resulted in superior progression‐free survival (PFS), overall survival (OS), and disease‐specific survival (DSS) compared with definitive radiotherapy (p < 0.05). Furthermore, multivariate analysis revealed that primary surgery independently correlated with superior PFS (HR = 0.37, p = 0.002), OS (HR = 0.55, p = 0.012), and DSS (HR = 0.45, p = 0.020) in early‐stage SCCSPs. Additionally, no significant prognostic differences were observed between HPV/p16 positive and HPV/p16 negative SCCSPs (p > 0.05). Surgery…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
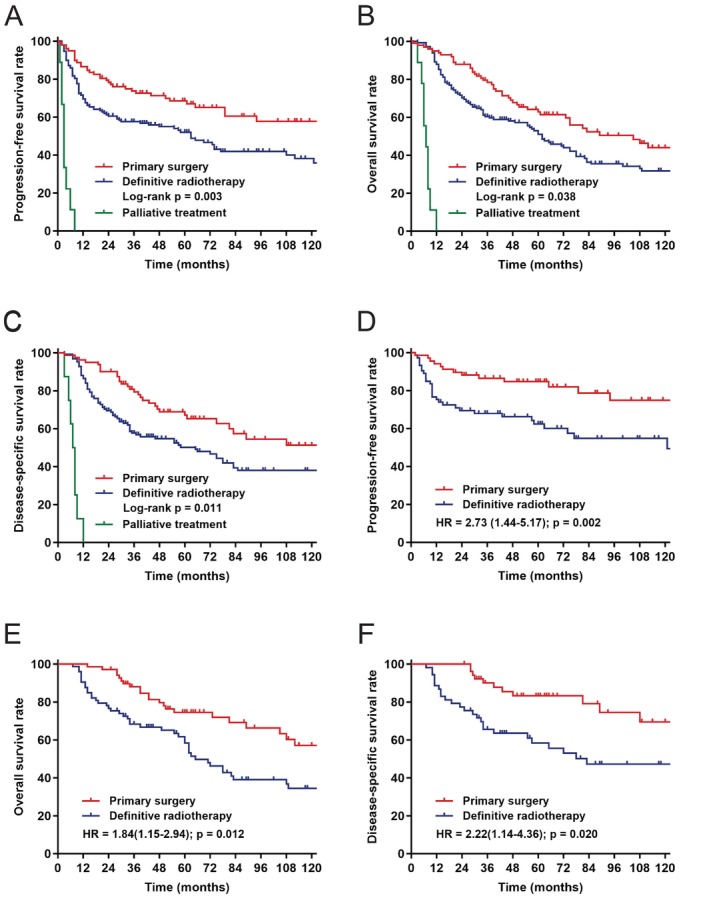 FIGURE 1
FIGURE 1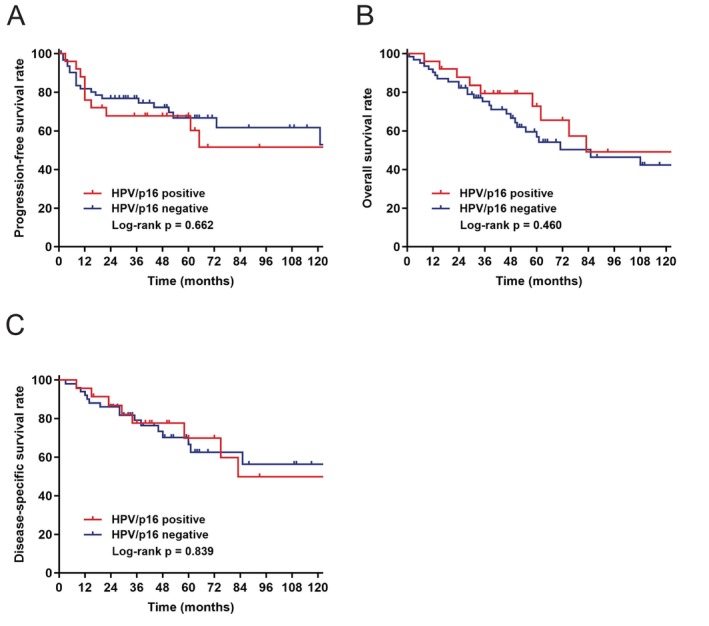 FIGURE 2
FIGURE 2| Variable | Number (%) | Primary surgery, | Definitive RT, |
| HPV/p16+, | HPV/p16−, |
|
|---|---|---|---|---|---|---|---|
| Age, y | 57.63 (9.44) | 57.32 (8.67) | 57.57 (9.87) | 0.156 | 55.20 (9.03) | 56.87 (9.03) | 0.439 |
| Gender | 0.218 | 0.348 | |||||
| Male | 234 (91.4) | 87 (87.9) | 138 (93.2) | 22 (88.0) | 59 (95.2) | ||
| Female | 22 (8.6) | 12 (12.1) | 10 (6.8) | 3 (12.0) | 3 (4.8) | ||
| Smoker | 0.075 | 1 | |||||
| Negative | 80 (31.2) | 39 (39.4) | 38 (25.7) | 7 (28.0) | 16 (25.8) | ||
| Positive | 176 (68.8) | 60 (60.6) | 110 (74.3) | 18 (72.0) | 46 (74.2) | ||
| Drinker | 0.296 | 0.058 | |||||
| Negative | 130 (50.8) | 56 (56.6) | 69 (46.6) | 7 (28.0) | 30 (48.4) | ||
| Positive | 126 (49.2) | 43 (43.4) | 79 (53.4) | 18 (72.0) | 32 (51.6) | ||
| Previous cancer | 0.034 | 1 | |||||
| No | 234 (91.4) | 85 (85.9) | 141 (95.3) | 23 (92.0) | 57 (91.9) | ||
| Yes | 22 (8.6) | 14 (14.1) | 7 (4.7) | 2 (8.0) | 5 (8.1) | ||
| HPV/p16 status | 0.004 | ||||||
| Negative | 62 (71.3) | 44 (84.6) | 17 (51.5) | ||||
| Positive | 25 (28.7) | 8 (15.4) | 16 (48.5) | ||||
| Unknown | 169 | 47 | 115 | ||||
| RN involved | 24 (9.4) | 0 | 20 (13.5) | < 0.001 | 4 (16.0) | 5 (8.1) | 0.272 |
| cT stage | < 0.001 | 0.796 | |||||
| T1 | 81 (31.6) | 35 (35.4) | 45 (30.4) | 8 (32.0) | 19 (30.6) | ||
| T2 | 113 (44.1) | 56 (56.6) | 56 (37.8) | 11 (44.0) | 29 (46.8) | ||
| T3 | 29 (11.3) | 4 (4.0) | 22 (14.9) | 2 (8.0) | 8 (12.9) | ||
| T4 | 33 (12.9) | 4 (4.0) | 25 (16.9) | 4 (16.0) | 6 (9.7) | ||
| cN stage | 0.652 | 0.108 | |||||
| N0 | 140 (54.7) | 60 (60.6) | 79 (53.4) | 15 (60.0) | 34 (54.8) | ||
| N1 | 31 (13.3) | 11 (11.1) | 23 (15.5) | 3 (12.0) | 8 (12.9) | ||
| N2 | 74 (28.9) | 25 (25.3) | 42 (28.4) | 5 (20.0) | 20 (32.3) | ||
| N3 | 8 (3.1) | 3 (3.0) | 4 (2.7) | 2 (8.0) | 0 | ||
| Overall c‐stage | 0.381 | 0.111 | |||||
| I | 60 (23.4) | 27 (27.3) | 33 (22.3) | 7 (28.0) | 15 (24.2) | ||
| II | 62 (24.2) | 29 (29.3) | 32 (21.6) | 6 (24.0) | 14 (22.6) | ||
| III | 42 (16.4) | 14 (14.1) | 28 (18.9) | 6 (24.0) | 12 (19.4) | ||
| IVa | 79 (30.9) | 24 (24.2) | 48 (32.4) | 4 (16.0) | 21 (33.9) | ||
| IVb | 13 (5.1) | 5 (5.1) | 7 (4.7) | 2 (8.0) | 0 | ||
| Treatment | 0.004 | ||||||
| Primary surgery | 99 (38.7) | 8 (32.0) | 44 (71.0) | ||||
| Definitive RT | 148 (57.8) | 16 (64.0) | 17 (27.4) | ||||
| RT/CRT | 118 | 12 | 10 | ||||
| ICT + RT/CRT | 30 | 4 | 7 | ||||
| Palliative | 9 (3.5) | 1 (4.0) | 1 (1.6) |
| Variable | Univariate analysis | Multivariate analysis (PFS) | Univariate analysis | Multivariate analysis (OS) | Univariate analysis | Multivariate analysis (DSS) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5 years PFS (%) |
| HR (95% CI) |
| 5 year OS (%) |
| HR (95% CI) |
| 5 year DSS (%) |
| HR (95% CI) |
| |
| whole cohort | 56.8 | 53.8 | 61.4 | |||||||||
| Age, y | 0.030 | 1.03 (1.01–1.05) | 0.004 | < 0.001 | 1.04 (1.02–1.06) | < 0.001 | < 0.001 | 1.04 (1.02–1.06) | < 0.001 | |||
| Gender | 0.495 | 0.484 | 0.255 | |||||||||
| Male | 55.7 | 53.2 | 60.0 | |||||||||
| Female | 67.9 | 62.9 | 76.5 | |||||||||
| Smoker | 0.258 | 0.135 | 0.231 | |||||||||
| Negative | 61.0 | 57.5 | 61.9 | |||||||||
| Positive | 54.7 | 52.6 | 61.2 | |||||||||
| Drinker | 0.768 | 0.160 | 0.415 | |||||||||
| Negative | 57.5 | 56.3 | 61.4 | |||||||||
| Positive | 56.0 | 52.0 | 61.4 | |||||||||
| Previous cancer | 0.570 | 0.911 | 0.561 | |||||||||
| No | 62.9 | 54.3 | 61.4 | |||||||||
| Yes | 56.2 | 52.4 | 62.9 | |||||||||
| RN involved | 0.339 | 0.812 | 0.714 | |||||||||
| No | 56.5 | 54.1 | 61.9 | |||||||||
| Yes | 57.8 | 50.8 | 55.9 | |||||||||
| HPV/p16 status | 0.662 | 0.460 | 0.839 | |||||||||
| Negative | 66.8 | 58.4 | 72.5 | |||||||||
| Positive | 67.8 | 72.8 | 72.8 | |||||||||
| Unknown | ||||||||||||
| cT stage | < 0.001 | 0.006 | < 0.001 | 0.073 | < 0.001 | 0.025 | ||||||
| T1‐2 | 63.5 | 1.00 | 59.2 | 1.00 | 67.8 | 1.00 | ||||||
| T3‐4 | 35.4 | 1.76 (1.18–2.64) | 37.5 | 1.43 (0.97–2.10) | 40.6 | 1.65 (1.07–2.54) | ||||||
| cN stage | < 0.001 | 0.001 | 0.002 | 0.009 | < 0.001 | < 0.001 | ||||||
| N0‐1 | 65.2 | 1.00 | 60.9 | 1.00 | 69.9 | 1.00 | ||||||
| N2‐3 | 37.9 | 1.93 (1.31–2.85) | 38.9 | 1.62 (1.13–2.31) | 42.2 | 2.09 (1.39–3.13) | ||||||
| Overall c‐stage | ||||||||||||
| I‐III | 68.5 | Ref | 64.1 | Ref | 74.4 | Ref | ||||||
| IV | 35.2 | < 0.001 | 35.4 | < 0.001 | 38.3 | < 0.001 | ||||||
| Treatment | ||||||||||||
| Definitive RT | 52.0 | Ref | 1 | Ref | 52.8 | Ref | 1 | Ref | 57.4 | Ref | 1 | Ref |
| Primary surgery | 68.6 | 0.003 | 0.68 (0.45–1.04) | 0.080 | 62.8 | 0.038 | 0.78 (0.54–1.12) | 0.172 | 72.5 | 0.011 | 0.71 (0.46–1.11) | 0.130 |
| Palliative | 0 | < 0.001 | 10.29 (4.16–25.45) | < 0.001 | 0 | < 0.001 | 27.80 (10.65–72.59) | < 0.001 | 0 | < 0.001 | 28.66 (10.13–81.06) | < 0.001 |
| Variable | PFS | OS | DSS | |||
|---|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| |
| Age, y | 1.01 (0.98–1.05) | 0.457 | 1.04 (1.01–1.07) | 0.008 | 1.03 (0.99–1.07) | 0.141 |
| cT stage | ||||||
| T1 | 1 | 1 | 1 | |||
| T2 | 3.06 (1.53–6.11) | 0.002 | 1.31 (0.80–2.15) | 0.286 | 2.57 (1.25–5.31) | 0.011 |
| cN stage | ||||||
| N0 | 1 | 1 | 1 | |||
| N1 | 1.56 (0.78–3.13) | 0.210 | 1.55 (0.84–2.84) | 0.159 | 1.64 (0.77–3.49) | 0.200 |
| Treatment | ||||||
| Definitive RT | 1 | 1 | 1 | |||
| Primary surgery | 0.37 (0.19–0.69) | 0.002 | 0.55 (0.34–0.87) | 0.012 | 0.45 (0.23–0.88) | 0.020 |
| Author, year | Country | HPV/p16+ tumors | Total number | HPV prevalence | HPV detection |
|---|---|---|---|---|---|
| Haeggblom et al., 2017 [ | Review | 59 | 488 | 12.1% | unknown |
| Rietbergen et al., 2013 [ | Netherlands | 9 | 124 | 7.3% | p16 IHC and PCR |
| Tham et al., 2019 [ | SEER | 28 | 115 | 24.3% | unknown |
| Schache et al., 2016 [ | UK | 8 | 88 | 9.1% | p16 IHC and PCR or ISH |
| The present study | China | 25 | 87 | 28.7% | p16 IHC and PCR |
| Wang et al., 2016 [ | China | 3 | 50 | 6% | PCR |
| Iyer et al., 2015 [ | USA | 8 | 46 | 17.4% | p16 IHC |
| Lamet al., 2015 [ | China | 3 | 32 | 9.4% | PCR |
| Rietbergen et al., 2012 [ | Netherlands | 0 | 31 | 0 | p16 IHC and PCR |
| Nasman et al., 2013 [ | Sweden | 7 | 22 | 31.8% | PCR |
| Lybak et al., 2016 [ | Norway | 5 | 21 | 23.8% | PCR |
| Gillison et al., 2012 [ | USA | 8 | 20 | 40% | p16 IHC |
| Saito et al., 2013 [ | Japan | 3 | 16 | 18.7% | p16 IHC |
| Cerezo et al., 2014 [ | Spain | 5 | 13 | 38.5% | p16 IHC |
| Schache et al., 2013 [ | UK | 4 | 13 | 30.8% | PCR |
| Limbergen et al., 2014 [ | Belgium | 0 | 11 | 0 | p16 IHC and PCR |
| Morbini et al., 2014 [ | Italy | 1 | 10 | 10% | ISH |
| Kim et al., 2014 [ | Korea | 4 | 10 | 40% | p16 IHC and PCR |
| Jiang et al., 2015 [ | USA | 0 | 10 | 0 | ISH |
| Kim et al., 2015 [ | South Korea | 1 | 9 | 11.1% | p16 IHC |
| Ukpo et al., 2009 [ | USA | 3 | 8 | 37.5% | PCR |
| Park et al., 2012 [ | Korea | 1 | 8 | 12.5% | p16 IHC and PCR |
| McIlwain et al., 2014 [ | USA | 4 | 6 | 66.7% | p16 IHC |
| Davis et al., 2014 [ | USA | 0 | 6 | 0 | p16 IHC |
| Grisar et al., 2016 [ | Belgium | 1 | 5 | 20% | p16 IHC |
| Bahl et al., 2014 [ | India | 0 | 5 | 0 | PCR |
| Bhosale et al., 2016 [ | India | 0 | 5 | 0 | p16 IHC |
| Hoffmann et al., 2012 [ | Germany | 1 | 4 | 25% | p16 IHC and PCR or ISH |
| Total | 167 | 1162 | 14.4% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Head and Neck Surgical Oncology · Salivary Gland Tumors Diagnosis and Treatment
Introduction
1
The incidence of oropharyngeal squamous cell carcinoma (OPSCC) has risen dramatically on a global scale, largely attributed to the increasing prevalence of human papillomavirus (HPV) within the population [1]. The oropharynx is comprised of four primary subsites: the tonsils, the base of tongue, the soft palate, and the posterior pharyngeal walls. Squamous cell carcinoma of the soft palate (SCCSP) is a relatively rare entity, accounting for approximately 10% of all OPSCCs [2]. In comparison to tonsillar‐related OPSCCs (squamous cell carcinomas of the tonsils and the base of tongue), SCCSP is linked to a poorer prognosis, with a reported 5‐year survival rate of only about 40% [3, 4].
The soft palate is composed of a stratified squamous epithelium that lacks a keratinized layer, similar to the epithelium found in the oral cavity. In contrast to the tonsillar‐related areas in the oropharynx, lymphoid tissue is not abundantly present in the soft palate [5]. Previous research has indicated that HPV‐positive OPSCC demonstrates a high responsiveness to treatment and is associated with a favorable prognosis. However, the occurrence of HPV‐positive disease in the soft palate is relatively infrequent [6]. Furthermore, the prognostic implications of HPV status in SCCSP remain ambiguous due to its rarity. Given that SCCSPs are typically located superficially and can be readily visualized during examination, they can often be diagnosed at an early stage. The management of SCCSP is still a subject of controversy, with ongoing debates regarding treatment modalities, including surgery and radiotherapy [7]. Additionally, literature specifically addressing SCCSP is limited, and there is a scarcity of studies featuring large sample sizes and long‐term outcome data.
In this study, we aim to evaluate the treatment outcomes of patients with SCCSP and to assess the influence of HPV status on prognosis within a large tertiary cancer center located in South China.
Patients and Methods
2
Patient Identification and Data Collection
2.1
We retrospectively included consecutive patients diagnosed with SCCSP between January 1981 and December 2021 at the Sun Yat‐sen University Cancer Center, a tertiary referral center located in South China. Clinical, pathological, and demographic information was extracted from the medical records of eligible patients. The inclusion criteria were as follows: (i) histologically confirmed squamous cell carcinoma located in the soft palate or uvula; (ii) a minimum of 2 years of clinical follow‐up for patients who did not experience tumor progression or who were alive at the last follow‐up. Patients with distant metastatic disease or other uncontrolled malignancies at the time of initial presentation were excluded from the study. This study was approved by our hospital's Institutional Review Board, and the ethics committee review specifically waived the need for informed consent.
HPV/p16 positivity was determined through the detection of high‐risk HPV types utilizing the real‐time polymerase chain reaction (RT‐PCR) method or by positive immunohistochemistry for p16, characterized by diffuse and strong cytoplasmic and nuclear staining in more than 70% of tumor cells [8]. In this study, tumor staging was conducted in accordance with the seventh edition of the American Joint Committee on Cancer (AJCC) staging guidelines for oropharyngeal cancers. The eighth edition of the AJCC staging guidelines was not applied due to the unknown HPV/p16 status in a significant proportion of the patient cohort.
Treatment Groups
2.2
Patients were evaluated by our multidisciplinary head and neck cancer board before the commencement of treatment. The initial treatment approach was categorized into two groups: the primary surgery group and the definitive radiotherapy group.
The primary surgery cohort comprised patients who underwent surgery with curative intent. Unilateral or bilateral therapeutic neck dissection was conducted for patients with clinically suspected lymph node metastasis, while prophylactic lymph node dissection was not actively performed for patients with cN0 tumors.
The definitive radiotherapy cohort comprised patients who underwent radiotherapy, either alone or in conjunction with concurrent therapy, which may or may not have included induction chemotherapy. The concurrent therapy regimen encompassed platinum‐based therapies and Nimotuzumab, or was combined with oral fluorouracil (capecitabine). Induction chemotherapy involved platinum‐based therapies in combination with paclitaxel‐based therapies, or was administered alongside either 5‐fluorouracil or oral fluorouracil (capecitabine).
Outcomes and Statistical Analysis
2.3
Differences in patient characteristics concerning treatment regimens and HPV/p16 status were analyzed using the Student's t‐test, Fisher's exact test, Mann–Whitney U test, and chi‐squared test. The survival endpoints included progression‐free survival (PFS), overall survival (OS), and disease‐specific survival (DSS). PFS was defined as the interval from the date of initial treatment to the date of tumor progression, which encompassed local recurrence, lymph node metastasis, distant metastasis, or death, with surviving patients without evidence of disease being censored at the last follow‐up. OS was calculated from the date of diagnosis to the date of death from any cause, with surviving patients censored at the last follow‐up. DSS was calculated from the date of diagnosis to the date of death specifically from SCCSP, with patients who did not experience SCCSP‐related death being censored at the date of the last follow‐up or at the time of non‐SCCSP‐related death. Survival time was estimated using the Kaplan–Meier method and compared using the log‐rank test for significance. The Cox proportional regression model was used for multivariate analysis. All tests were two‐sided. A p‐value of less than 0.05 was considered statistically significant. All data were analyzed using SPSS 26 software (SPSS, Chicago, IL).
Results
3
Characteristics of Patients
3.1
A total of 256 consecutive patients were enrolled in this study. All patients were ethnic Chinese. The mean age at diagnosis was 57.63 years, with a notable male predominance observed (91.4%). A majority of the patients (68.8%) were smokers, and approximately half of these individuals (49.2%) were drinkers. Twenty‐two patients had a prior history of cancer, with 14 cases located in the head and neck region and 8 cases in other anatomical sites. The baseline characteristics of the study population are summarized in Table 1.
The majority of patients initially presented with early T‐stage (T1‐2; n = 194, 75.7%) and early N‐stage diseases (N0‐1; n = 171, 68.0%). Additionally, 141 patients (55.1%) were classified as having overall early‐stage diseases (T1‐2 N0‐1 M0). Among the cohort, 87 patients underwent HPV/p16 testing, of which 25 patients (28.7%) were identified as HPV/p16 positive. When compared to HPV/p16 negative patients, those who were HPV/p16 positive were significantly more likely to receive definitive radiotherapy (64.0% vs. 27.4%, p = 0.004).
Treatment Characteristics
3.2
Among the total patient cohort, 99 individuals (38.7%) underwent primary surgery, of which 36 subsequently received postoperative radiotherapy (PORT). Additionally, 148 patients (57.8%) were treated with definitive radiotherapy, with 30 of these patients having received induction chemotherapy prior to the radiotherapy. Induction chemotherapy was administered to patients presenting with clinical T2‐4 stage tumors. Nine patients received palliative treatment due to advanced disease; the palliative treatment regimens included platinum‐based therapies, paclitaxel‐based therapies, or combinations thereof with either 5‐fluorouracil or oral fluorouracil (capecitabine) chemotherapy.
In comparison to patients who underwent primary surgery, those in the definitive radiotherapy group exhibited a lower likelihood of having a prior history of cancer (p = 0.034). Conversely, they demonstrated a higher likelihood of presenting with HPV/p16 positive disease (p = 0.004), retropharyngeal lymph node involvement (p < 0.001), and advanced clinical T‐stage disease (p < 0.001).
Survival Analysis
4
Oncological Outcomes Concerning Various Treatment Groups
4.1
The median follow‐up duration for all patients was 52 months (range: 4–504 months), while for surviving patients, it was 68 months (range: 25–504 months). As of the last follow‐up date, tumor progression was observed in 124 patients (48.4%), and 156 patients (60.9%) had died, including 112 patients (43.8%) who succumbed to disease‐specific causes. The 5‐year PFS, OS, and DSS for the entire cohort were 56.8%, 53.8%, and 61.4%, respectively. When analyzed by treatment modality, the 5‐year PFS, OS, and DSS rates for patients who underwent primary surgery compared to those who received definitive radiotherapy were 68.6% versus 52.0% (p = 0.003), 62.8% versus 52.8% (p = 0.038), and 72.5% versus 57.4% (p = 0.011), respectively. The Kaplan–Meier survival curves are presented in Figure 1.
Kaplan–Meier survival curves stratified by treatment group. (A) Kaplan–Meier curve for PFS in the whole cohort stratified by treatment group. (B) Kaplan–Meier curve for OS in the whole cohort stratified by treatment group. (C) Kaplan–Meier curve for DSS in the whole cohort stratified by treatment group. (D) Kaplan–Meier curve for PFS in early‐stage SCCSPs stratified by treatment group. (E) Kaplan–Meier curve for OS in early‐stage SCCSPs stratified by treatment group. (F) Kaplan–Meier curve for DSS in early‐stage SCCSPs stratified by treatment group. [Color figure can be viewed at wileyonlinelibrary.com]
In the primary surgery cohort, univariate analysis indicated that patients who underwent PORT experienced significantly poorer PFS (5‐year PFS: 50.9% vs. 79.5%, p = 0.001), OS (5‐year OS: 51.3% vs. 69.5%, p = 0.048), and DSS (5‐year DSS: 57.0% vs. 82.0%, p = 0.002) in comparison to those who did not receive PORT (see Table 2).
In the definitive radiotherapy cohort, patients who underwent induction therapy did not demonstrate a statistically significant enhancement in PFS (p = 0.296), OS (p = 0.362), or DSS (p = 0.224). Additionally, we evaluated the prognostic implications of salvage surgery within this cohort. A total of 25 patients underwent salvage surgery due to residual locoregional disease or progression of locoregional disease. The results indicated that salvage surgery was associated with a statistically significant improvement in 5‐year OS (74.3%, p = 0.023) and a near statistically significant enhancement in 5‐year DSS (79.2%, p = 0.068).
In the multivariable analysis, no statistically significant differences were observed in PFS (p = 0.080), OS (p = 0.172), or DSS (p = 0.130) between patients who underwent primary surgery and those who received definitive radiotherapy (see Table 2).
Treatment Outcomes for Early‐Stage SCCSPs
4.2
We conducted a comparative analysis of treatment outcomes for a cohort of 141 patients (55.1%) with clinical early‐stage tumors (cT1‐2 N0‐1 M0). The results indicated that primary surgical intervention yielded favorable 5‐year PFS rates of 84.7%, OS rates of 74.5%, and DSS rates of 86.8% in this cohort. Multivariable survival analysis demonstrated that primary surgery, in contrast to definitive radiotherapy, was significantly associated with improved PFS (HR = 0.37, p = 0.002), OS (HR = 0.55, p = 0.012), and DSS (HR = 0.45, p = 0.020). A summary of the survival outcomes is presented in Table 3 and Figure 2.
Kaplan–Meier survival curves stratified by HPV/p16 status. (A) Kaplan–Meier curve for PFS stratified by HPV/p16 status. (B) Kaplan–Meier curve for OS stratified by HPV/p16 status. (C) Kaplan–Meier curve for DSS stratified by HPV/p16 status. [Color figure can be viewed at wileyonlinelibrary.com]
Oncological Outcomes Concerning HPV/p16 Status
4.3
Survival analyses were conducted on patients with known HPV/p16 status. In the univariate analysis, patients who were HPV/p16 positive exhibited survival rates comparable to those who were HPV/p16 negative. The 5‐year PFS, OS, and DSS for patients with HPV/p16 positive disease compared to those with HPV/p16 negative disease were 67.8% versus 66.8% (p = 0.662), 72.8% versus 58.4% (p = 0.460), and 72.8% versus 72.5% (p = 0.839), respectively. The Kaplan–Meier survival curves are presented in Figure 2.
Complications
4.4
In total, 19 out of 256 patients (7.4%) experienced severe complications. Among these, one patient developed postoperative pneumonia following surgery and subsequently succumbed to acute respiratory failure. The remaining 18 patients presented with one or more of the following severe complications: permanent feeding tube placement for nutritional support (9 patients), skin ulcer (5 patients), oral mucositis (4 patients), osteoradionecrosis (3 patients), and wound infection after a planned neck dissection that necessitated surgical debridement (1 patient).
Discussion
5
There exists a limited number of studies that independently analyze SCCSP from the other oropharyngeal subsites. The current cohort represents one of the largest single‐institution series documented in the literature to date. Our analysis demonstrated that primary is associated with enhanced oncological outcomes for patients with early‐stage SCCSP. Furthermore, our findings did not support the prognostic significance of HPV status in SCCSP.
The baseline patient characteristics observed in this study are largely consistent with those documented in prior research. A significant majority (75.7%) of SCCSPs presented with early T‐stage tumors (T1‐2), which are readily identifiable during clinical examination. The distribution of age, as well as the proportions of smokers, alcohol consumers, patients with cancer history, early T‐stage tumors, and early N‐stage tumors (N0‐1), align closely with findings reported in the existing literature [4, 9, 10, 11, 12]. However, it is noteworthy that our cohort exhibited a higher proportion of male patients, accounting for 91.0%.
It has been well established that patients with HPV‐positive OPSCC typically present with an earlier onset age, improved performance status, reduced tobacco exposure rates, and heightened sensitivity to radiotherapy, resulting in a notably favorable prognosis [2, 13, 14, 15]. However, similar characteristics were not observed in SCCSPs. The prevalence of HPV‐positive disease (28.7%) in SCCSPs in the current study was significantly lower than that found in tonsillar‐related OPSCCs. A summary of the prevalence of HPV/p16 positive disease in SCCSPs reported in the literature is presented in Table 4. In this study, HPV‐positive SCCSPs exhibited comparable onset ages and similar proportions of positive smokers and drinkers when compared to HPV‐negative SCCSPs. Furthermore, our results indicated that HPV status did not hold prognostic significance in SCCSPs. We found that the survival rates of SCCSPs, irrespective of HPV status, were analogous to those of HPV‐negative tonsillar‐related OPSCC [3, 42]. These findings support the assertion that all other OPSCCs (carcinomas arising in the oropharynx outside the tonsils and base of the tongue) should be classified as HPV‐negative OPSCC. Given the considerable research interest in de‐escalating treatment for patients with HPV‐positive OPSCC due to their excellent outcomes, it is imperative to consider the impact of oropharyngeal subsites in treatment planning to mitigate treatment‐related toxicity.
Prior research has demonstrated satisfactory locoregional control rates and cause‐specific survival in patients with SCCSPs who underwent definitive radiotherapy; however, the overall 5‐year OS was approximately 40% [9, 10]. In the current study, the 5‐year OS rate for patients receiving definitive radiotherapy was significantly improved at 52.8%. Furthermore, we observed that patients who underwent salvage surgery exhibited favorable OS and DSS rates. The implementation of salvage surgery may have contributed to the enhanced outcomes observed in our study. Additionally, our findings indicated excellent outcomes for patients treated with primary surgery, with the 5‐year DSS comparable to the results reported by Iyer et al., which included a cohort of 150 patients treated with primary surgical intervention [11]. The 5‐year PFS rate of 52.0% and OS rate of 52.8% for the entire cohort in this study are notably superior to the outcomes reported by Schernberg et al. Notably, a higher proportion (39.8%) of patients in the present cohort received surgical treatment. Given that primary surgery yielded satisfactory outcomes, we hypothesize that the favorable results observed in the primary surgery group may have contributed to the overall improved outcomes for the entire cohort in this study.
The findings of our study hold significant implications for the management of SCCSP. Patients with early‐stage disease exhibit an excellent prognosis when treated with primary surgery. As such, our results may provide a rational basis for reconsidering the management strategies for early‐stage SCCSP, advocating a transition from nonsurgical approaches to transoral robotic surgery (TORS). Existing literature indicates that TORS is associated with enhanced surgical outcomes and improved survival rates, accompanied by a minimal risk of severe complications in the treatment of early‐stage OPSCC [43, 44, 45, 46, 47]. The ORATOR trial, a randomized phase II study, compared primary radiotherapy with primary TORS and neck dissection for early‐stage OPSCC. The findings revealed that while patients receiving radiotherapy demonstrated superior scores on the MD Anderson Dysphagia Inventory (MDADI), the difference decreased with time and never reached a threshold. Importantly, post hoc subgroup analysis of patients with palatine tonsil primaries indicated no significant difference in MDADI scores between those undergoing surgical versus nonsurgical treatment [48, 49, 50]. However, comparative research examining outcomes between SCCSP patients treated with TORS and those receiving non‐TORS therapies remains limited. Given the favorable oncological outcomes associated with TORS and its suitability for early‐stage SCCSP, we propose that TORS may emerge as the preferred treatment modality for early‐stage SCCSP in the future, although further validation is warranted.
There are several limitations due to the retrospective nature of this study. First, a large number of patients lack information about tumor HPV status or p16 expression level. Our analysis of the prognostic role of HPV/p16 status was based on a relatively small sample size; further research with larger and more diverse populations is necessary to establish the reliability and validity of our findings. Second, this study primarily focused on the oncological outcomes of various treatment modalities and did not include functional assessments of swallowing and speech due to insufficient data. Lastly, as a retrospective study, it is inherently subject to the limitations typical of this type of research.
Conclusions
6
SCCSPs exhibit characteristics that are more similar to those arising in the oral cavity than to those associated with tonsillar‐related OPSCCs. HPV status does not have prognostic significance for SCCSP. In patients with early‐stage SCCSP, surgery yields a more favorable oncological outcome.
Conflicts of Interest
The authors declarenoconflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. C. Chi , T. A. Day , and B. W. Neville , “Oral Cavity and Oropharyngeal Squamous Cell Carcinoma—An Update,” CA: a Cancer Journal for Clinicians 65 (2015): 401–421.26215712 10.3322/caac.21293 · doi ↗ · pubmed ↗
- 2T. D. Ellington , S. J. Henley , V. Senkomago , et al., “Trends in Incidence of Cancers of the Oral Cavity and Pharynx ‐ United States 2007‐2016,” Mmwr‐Morbidity and Mortality Weekly Report 69 (2020): 433–438.32298244 10.15585/mmwr.mm 6915 a 1PMC 7755056 · doi ↗ · pubmed ↗
- 3T. Tham , S. Ahn , D. Frank , D. Kraus , and P. Costantino , “Anatomical Subsite Modifies Survival in Oropharyngeal Squamous Cell Carcinoma: National Cancer Database Study,” Head & Neck 42, no. 3 (2019): 434–445, 10.1002/hed.26019.31773842 · doi ↗ · pubmed ↗
- 4C. K. Chan , A. Y. Han , J. E. Alonso , et al., “Squamous Cell Carcinoma of the Soft Palate in the United States: A Population‐Based Study,” Otolaryngology–Head and Neck Surgery 159, no. 4 (2018): 662–668, 10.1177/0194599818771931.29734872 · doi ↗ · pubmed ↗
- 5E. Gelwan , I.‐J. Malm , A. Khararjian , C. Fakhry , J. A. Bishop , and W. H. Westra , “Nonuniform Distribution of High‐Risk Human Papillomavirus in Squamous Cell Carcinomas of the Oropharynx: Rethinking the Anatomic Boundaries of Oral and Oropharyngeal Carcinoma From an Oncologic HPV Perspective,” American Journal of Surgical Pathology 41 (2017): 1722–1728.28877058 10.1097/PAS.0000000000000929 · doi ↗ · pubmed ↗
- 6L. Haeggblom , T. Ramqvist , M. Tommasino , T. Dalianis , and A. Näsman , “Time to Change Perspectives on HPV in Oropharyngeal Cancer. A Systematic Review of HPV Prevalence per Oropharyngeal Sub‐Site the Last 3 Years,” Papillomavirus Research 4 (2017): 1–11.29179862 10.1016/j.pvr.2017.05.002PMC 5883233 · doi ↗ · pubmed ↗
- 7Y. Monnier and C. Simon , “Surgery Versus Radiotherapy for Early Oropharyngeal Tumors: A Never‐Ending Debate,” Current Treatment Options in Oncology 16 (2015): 42.26187797 10.1007/s 11864-015-0362-4 · doi ↗ · pubmed ↗
- 8C. Ndiaye , M. Mena , L. Alemany , et al., “HPV DNA, E 6/E 7 m RNA, and p 16 INK 4a Detection in Head and Neck Cancers: A Systematic Review and Meta‐Analysis,” Lancet Oncology 15 (2014): 1319–1331.25439690 10.1016/S 1470-2045(14)70471-1 · doi ↗ · pubmed ↗