Severe Anemia Caused by a Colorectal Lipoma With Central Erosions: A Case Report
Yusuke Yoshida, Ryohei Shoji, Yuki Matsumi, Ko Watanabe, Toshiyoshi Fujiwara

TL;DR
A man in his 70s developed severe anemia due to a rare complication of a colorectal lipoma, which was diagnosed and treated with surgery.
Contribution
This case highlights that large colorectal lipomas can cause anemia and should be considered in differential diagnoses for gastrointestinal bleeding.
Findings
A cecal lipoma with central erosions was identified as the cause of severe anemia in a 70-year-old man.
Ileocecal resection confirmed the diagnosis and resolved the anemia.
The case underscores the importance of considering lipomas in the differential diagnosis of lower gastrointestinal bleeding.
Abstract
Colorectal lipomas are benign tumors that are often asymptomatic and discovered incidentally. In most cases, they can be managed conservatively with observation. We report the case of a man in his 70s with a colorectal lipoma located in the cecum. An investigation into his severe anemia led to the suspicion that the cecal lipoma was the underlying cause. An ileocecal resection was performed. Erosions were observed at the center of the lipoma. Although small colorectal lipomas are generally asymptomatic and rarely cause anemia, periodic endoscopic examinations are recommended. These lesions should be considered in the differential diagnosis of lower gastrointestinal bleeding.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
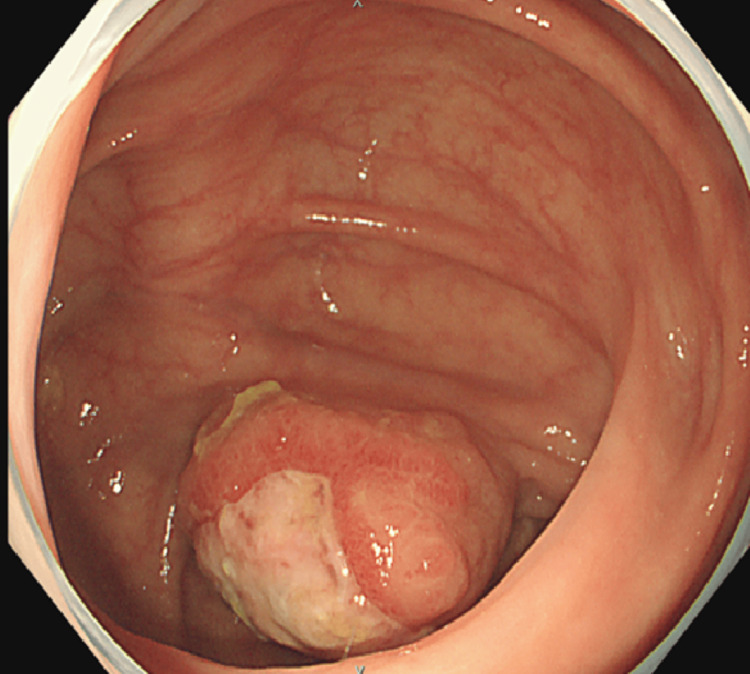 Figure 1
Figure 1 Figure 2
Figure 2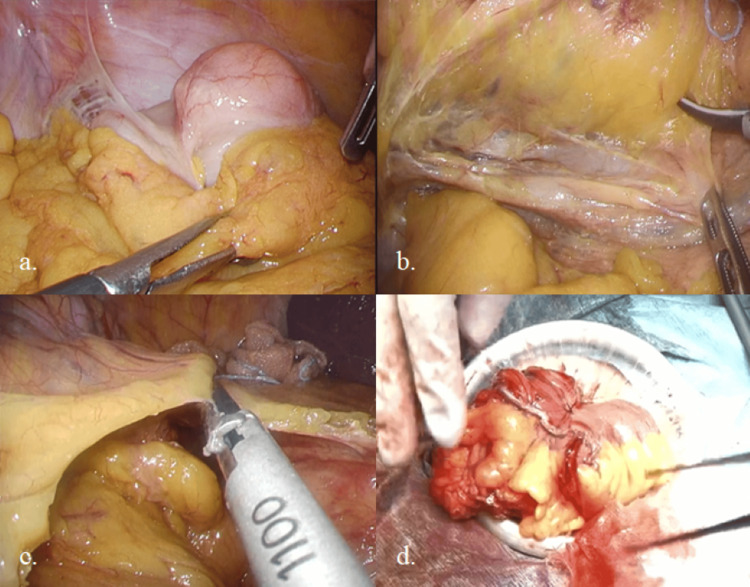 Figure 3
Figure 3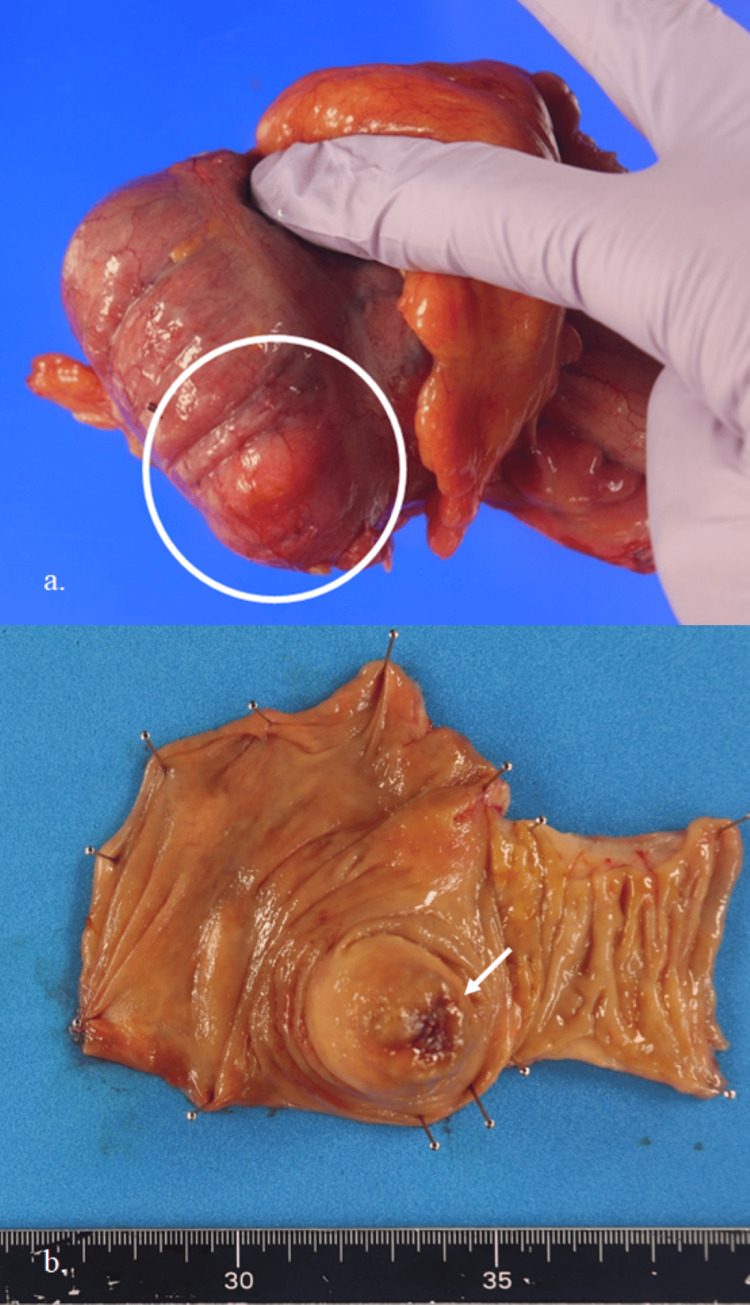 Figure 4
Figure 4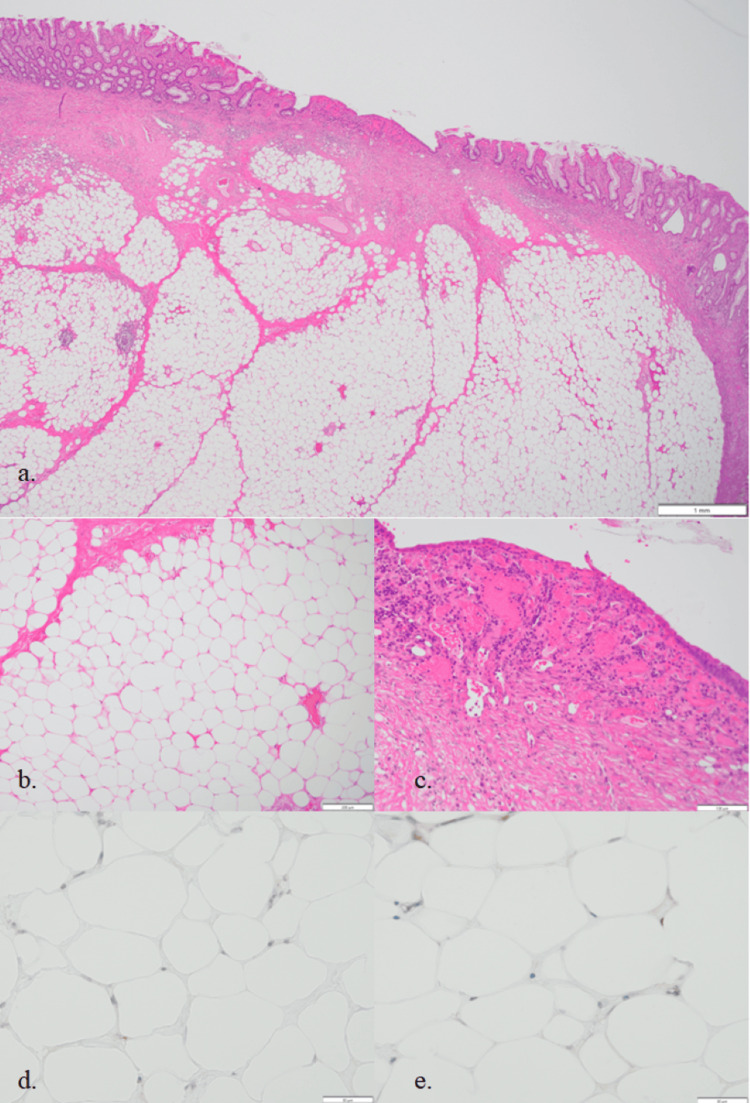 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Soft tissue tumor case studies · Tumors and Oncological Cases
Introduction
Colorectal lipomas are benign tumors that are frequently asymptomatic [1]. In many cases, they are discovered incidentally during imaging, colonoscopy, surgery, or autopsy [1]. Because they are composed predominantly of fat cells and arise from the submucosa, the overlying mucosal surface is typically smooth. When the tumor becomes large, it may compress surrounding tissues and cause bleeding [2]. However, colorectal lipomas that cause bleeding with associated mucosal erosions are extremely rare. Here, we report a case of a colorectal lipoma presenting with mucosal erosions.
Case presentation
A man in his 70s undergoing maintenance hemodialysis for chronic renal failure was found to have severe anemia (hemoglobin: 6.9 g/dL; reference range: 13.7-16.8 g/dL) during a laboratory evaluation conducted due to intradialytic hypotension. Total colonoscopy revealed a 3-cm submucosal tumor with mucosal erosions located in the cecum (Figure 1).
Lower gastrointestinal endoscopic imageA submucosal tumor-like lesion was observed in the cecum. Ulceration with a white exudate was present at the center of the lesion, which was suspected to be the source of bleeding.
Upper gastrointestinal endoscopy showed no significant findings, and the cecal lesion was suspected to be the source of gastrointestinal bleeding. Abdominal plain computed tomography (CT) revealed a low-density mass in the cecum, suggestive of a lipoma (Figure 2).
Plain abdominal computed tomography (CT)A low-density mass lesion was identified in the cecum (white arrow), suggestive of a lipoma.
Additionally, gallstones and a common bile duct stone were detected.
Based on these findings, a laparoscopic ileocecal resection was performed under the preoperative diagnosis of cecal lipoma. Given the presence of gallstones and a common bile duct stone, the common bile duct stone was endoscopically removed prior to surgery, and a cholecystectomy was performed concurrently with the ileocecal resection.
The colon surgery was initiated using the inferior approach for ileocecal mobilization, followed by mobilization of the hepatic flexure from the cephalad side (Figures 3a-3c). A cholecystectomy was then performed. Subsequently, the ileocecal resection was carried out extracorporeally using a functional end-to-end anastomosis, completing the procedure (Figure 3d).
Intraoperative images of ileocecal resection(a) The cecum was fixed to the abdominal wall and was not freely mobile.(b) Ileocecal mobilization was performed by the inferior approach.(c) The hepatic flexure was mobilized from the cephalad side.(d) A functional end-to-end anastomosis was performed.
Gross examination of the resected specimen revealed a submucosal yellow mass lesion measuring 3.1 × 1.7 cm (Figure 4a). A central mucosal erosion was noted (Figure 4b).
Macroscopic findings of the resected specimen(a) A yellowish submucosal tumor is seen in the cecum (white circle).(b) The center of the tumor shows mucosal erosion (white arrow).
Histologically, the mass was composed of mature adipocytes interspersed with thin fibrous septa, proliferating within the submucosal layer. The septal spindle-shaped cells exhibited mild atypia; however, immunohistochemical staining for MDM2 and CDK4 was negative, confirming the diagnosis of lipoma (Figure 5). The lipoma itself was not exposed at the site of erosion. Prominent intramucosal vascular hyperplasia suggested that the erosion was caused by mechanical irritation of the mucosal surface (Figure 5c).
Histological findings of the resected specimen(a) Low magnification (×20), hematoxylin and eosin (H&E) staining.(b) Medium magnification (×100), H&E staining showing adipocytes characteristic of lipoma.(c) Medium magnification (×100), H&E staining showing mucosal erosion and submucosal hypervascularization.(d,e) High magnification (×400), immunohistochemical staining for MDM2 and CDK4; both were negative.
Postoperative bleeding was observed on postoperative day 2, with anastomotic bleeding suspected. The patient was managed conservatively and discharged on postoperative day 8.
Discussion
In the present case, we found that a colorectal lipoma could be a potential cause of anemia.
Additionally, the lipoma exhibited central mucosal erosions.
While there are numerous reports of upper gastrointestinal bleeding caused by lipomas in the stomach, duodenum, and jejunum [3-7], reports of colorectal lipomas presenting with central erosions and associated bleeding are relatively rare, despite the colon being the most common site for gastrointestinal lipomas [6]. Hemorrhagic cases typically occur when the tumor is large [5,6]. In our case, however, the tumor was relatively small (3 cm in diameter), yet bleeding occurred.
Colorectal lipomas have frequently been reported as a cause of intestinal intussusception [8-11]. Although this patient had no typical abdominal symptoms such as pain or discomfort, we initially considered the possibility that ischemia due to intussusception had caused erosion and bleeding. However, intraoperative findings showed that the cecum was adherent to the abdominal wall (Figure 3a), and histological findings suggested that repeated intussusception was unlikely.
Therefore, we hypothesize that the bleeding was caused by mucosal desquamation due to mechanical irritation of the mucosal surface. A previous report suggested that gastrointestinal lipomas may cause bleeding due to the following: (1) impaired blood circulation in the overlying epithelium caused by tumor growth, (2) irritation by intestinal contents, and (3) mechanical irritation by peristalsis [3]. The patient’s comorbidities, including maintenance hemodialysis and the use of antithrombotic agents, may have also contributed to the severity of the hemorrhage.
The diagnosis of lipoma is typically straightforward with CT imaging, and small tumors are often asymptomatic and managed conservatively. While this is generally appropriate, our case highlights the importance of periodic endoscopic follow-up for anemia.
Another important differential diagnosis is hemangiolipoma [12], a benign tumor characterized by both adipose and vascular components. In our case, the erosive lesion consisted of intramucosal angiogenesis without tumor exposure, effectively ruling out hemangiolipoma. Although immunohistochemical staining was negative for liposarcoma markers, it remains crucial to differentiate such neoplasms, especially in tumors with rapid growth, where liposarcoma must be considered.
Conclusions
We encountered a rare case of a small colorectal lipoma that caused severe anemia. Although lipomas can often be suspected based on CT findings and small colorectal lipomas are typically managed conservatively, periodic endoscopic examinations are essential. Additionally, because colorectal lipomas with central erosions are extremely rare, it is important to differentiate them from liposarcomas and other neoplastic lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Endoscopic removal of large colonic lipomas Gastrointest Endosc Kim CY Bandres D Tio TL Benjamin SB Al-Kawas FH 9299315520021202415810.1067/mge.2002.124098 · doi ↗ · pubmed ↗
- 2Large lipoma of the ascending colon: a case report and review of literature J Surg Case Rep Farfour AN Abu Omar NA Alsohaibani FI 02020202010.1093/jscr/rjaa 354PMC 749706232968480 · doi ↗ · pubmed ↗
- 3A case of gastric lipoma presenting as gastrointestinal hemorrhage J Jpn Surg Assoc Tsugumasa K Yoshinari M Katsumi K Hiroyuki Y Kenji T Hiroyuki S 26822685702009 https://www.jstage.jst.go.jp/article/jjsa/70/9/70_9_2682/_article/-char/ja/
- 4Jejunal lipoma: a rare cause of small bowel bleeding Clin Case Rep Kozyk M Strubchevska K Batke M 011202310.1002/ccr 3.7228 PMC 1013041537124544 · doi ↗ · pubmed ↗
- 5Bleeding gastric lipoma resected by endoscopic submucosal dissection Cureus Mir AS Kesar V Sageer M Grider D Chitnavis V 012202010.7759/cureus.8909 PMC 738988732742875 · doi ↗ · pubmed ↗
- 6Duodenal lipoma as upper gastrointestinal bleeding presentation: case report and review of the literature Cureus Mousa MI Al Ghamdi SS Alsolmi AA Fakhri AF 015202310.7759/cureus.33996 PMC 993901336811043 · doi ↗ · pubmed ↗
- 7Giant duodenal lipoma: an unusual cause of gastrointestinal bleeding (a case report)Pan Afr Med J Baiss M Rahali A Elmajdoubi H 3423820213436742110.11604/pamj.2021.38.342.28951 PMC 8308844 · doi ↗ · pubmed ↗
- 8Colonic lipoma causing bowel intussusception: an up-to-date systematic review J Clin Med Menegon Tasselli F Urraro F Sciaudone G 51491020213476866810.3390/jcm 10215149 PMC 8584916 · doi ↗ · pubmed ↗