Surge in macrolide dispensing to Swiss children in a period of increased incidence of Mycoplasma pneumoniae detection: an interrupted time-series analysis
Manon Jaboyedoff, Catherine Plüss-Suard, Patrick M Meyer Sauteur, Stephen P Jenkinson, Alessandro Cassini, Noémie Boillat-Blanco, Pierre Alex Crisinel, François Angoulvant

TL;DR
Swiss children saw a sharp rise in macrolide antibiotic use in late 2023, likely due to increased Mycoplasma pneumoniae infections.
Contribution
This study provides empirical evidence of a surge in macrolide prescriptions in Swiss children linked to rising Mycoplasma pneumoniae cases.
Findings
Macrolide use increased by 235% in Swiss children aged 0 to 11 years from October 2023.
Amoxicillin use remained stable during the same period, suggesting a specific shift toward macrolides.
The rise in macrolide prescriptions coincided with a global increase in Mycoplasma pneumoniae infections.
Abstract
To evaluate the trend in macrolide ambulatory use among children in Switzerland following a global surge in Mycoplasma pneumoniae infections in late 2023. We conducted a population-based interrupted time-series analysis of macrolide use in Swiss children aged 0 to 11 years from 2018 to 2023 using national ambulatory antibiotic claims data. The main outcome was the evolution of macrolide use in ambulatory setting, expressed as monthly defined daily doses (DDD) per 1000 children. We defined two time periods: (i) the pre-autumn 2023 period, before M. pneumoniae detections increased in Switzerland (1 January 2018 to 30 September 2023) and (ii) the autumn 2023 period, after M. pneumoniae detections increased in Switzerland (1 October 2023 to 31 December 2023). We built a quasi-Poisson regression model to estimate the changes in macrolide monthly DDD per 1000 children from October 2023 in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
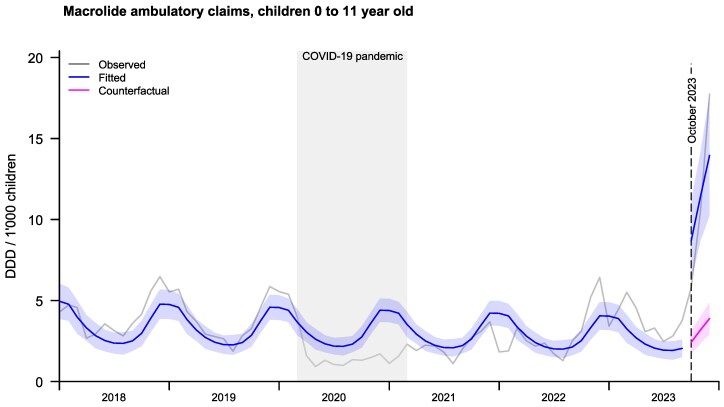 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Respiratory viral infections research · Bacterial Infections and Vaccines
Introduction
Macrolides are the first-line treatment for infections caused by Mycoplasma pneumoniae in children. M. pneumoniae infections occur worldwide but were quasi-absent during and following the COVID-19 pandemic.^1,2^ A marked increase in M. pneumoniae infections occurred globally at the end of the summer 2023, prompting the WHO to issue an alert in November 2023 informing about the upsurge of respiratory illnesses among children in Northern China.^3–5^ In children, M. pneumoniae causes respiratory tract infections, including community-acquired pneumonia (CAP), which generally manifests with milder symptoms and signs compared to other conventional bacterial causes of CAP. The main burden of disease caused by M. pneumoniae is therefore expected to be found in outpatient settings. We hypothesized that increased incidence of M. pneumoniae associated with the raised awareness of M. pneumoniae infections among paediatricians might have led to a higher rate of macrolide prescriptions.
We aimed to analyse macrolide paediatric claims data from Swiss community pharmacies invoices. The objective of the study was to evaluate trends in macrolide use in children in the context of M. pneumoniae cases increase in children by interrupted time-series analysis.
Methods
Study design
We conducted a population-based interrupted time-series analysis of macrolide antibiotic use in Swiss pharmacies over 72 months (1 January 2018 to 31 December 2023).
The main outcome was the evolution of macrolide (clarithromycin and azithromycin) use in ambulatory setting, expressed as monthly defined daily doses (DDD) per 1000 children. The interruption was set on 1 October 2023, when M. pneumoniae detections increased in Switzerland, coinciding with the first media alerts about the upsurge of respiratory illnesses among children.^3,6^ We analysed amoxicillin as a control outcome to prevent potential confounding. Given that amoxicillin is not effective to treat M. pneumoniae infections due to its natural resistance against β-lactam antibiotics, their increased incidence should not impact use of this antibiotic agent.
Data collection and source
In Switzerland, antibiotics for children are dispensed only with a physician’s prescription. In the ambulatory setting, antibiotics can be delivered by community pharmacies and by self-dispensing physicians in some areas of the country. The Swiss Pharmacists Association (https://pharmasuisse.org) provides antibiotic (ATC J01) claims data, which are dispensed in community pharmacies, to ANRESIS, the Swiss Centre for Antibiotic Resistance (https://www.anresis.ch). Pharmacies participating in this antibiotic use surveillance system are those using the billing service of the professional association of Swiss pharmacists (ofac, https://www.ofac.ch), representing ∼50% of all pharmacies in Switzerland (ranging from 50% in 2023 to 53% in 2018). These pharmacies are distributed across the entire country and include both urban and non-urban areas, providing a geographically and demographically representative sample. Claims data are provided in DDDs aggregated by month and by age groups, i.e. for children: 0 to 1 years and 2 to 11 years of age.
DDD is a technical unit allocated to drugs by the WHO Collaborating Centre in Oslo in association with the WHO International Working Group on Drug Statistics Methodology. It represents the ‘assumed average maintenance dose per day for a drug used for its main indication in adults’. The main outcome unit, DDD, has not been developed for evaluation of drug consumption in children and does not allow comparison of drug use between age groups. However, DDD can be used for overall comparison including time-trends. We expressed DDD per 1000 children per month by using population estimates of the Swiss Federal Office of Statistics, adjusted by age group and by year.
Statistical analysis
We built a quasi-Poisson regression model to estimate the changes in macrolide monthly DDD per 1000 children from October 2023 in Switzerland. We defined two time periods to analyse: (i) the pre-autumn 2023 period, before M. pneumoniae detections increased in Switzerland (1 January 2018 to 30 September 2023) and (ii) the autumn 2023 period, after M. pneumoniae detections increased in Switzerland (1 October 2023 to 31 December 2023). The model accounted for temporal trends before the WHO alert and for the seasonal pattern of macrolide prescriptions using harmonic terms (sines and cosines with 12-months periods). The time-unit was 1 month. We used data collected before October 2023 to generate counterfactual estimation of the number of DDD per 1000 children in the autumn 2023 period. We analysed data for the entire population of children and by age groups (i.e. 0 to 1 years and 2 to 11 years). We performed three sensitivity analyses to assess the robustness of the study findings: (i) clarithromycin use only, (ii) azithromycin use only and (iii) amoxicillin use as a control outcome. Analyses were performed using R Statistical Software (v.4.4.2; R Core Team 2021).
Ethics
This study was based on aggregated data submitted to ANRESIS. Because of the anonymous nature of the data, neither ethical approval nor written informed consent from patients was required.
Results
We found a statistically significant increase in macrolides use expressed in monthly DDD per 1000 children aged 0 to 11 years from October 2023 in Switzerland [+235% (95%CI +139%–+368%), P value < 0.001], Figure 1. The increase was more pronounced in the age group 2 to 11 years [+246% (95%CI +146%–+386%), P value < 0.001] than in the age group 0 to 1 year old [+123% (95%CI +58%–+215%), P value < 0.001] [Supplementary material, Figures S1 and S2 (available as Supplementary data at JAC-AMR Online)].
Monthly ambulatory DDDs of macrolides (clarithromycin and azithromycin) per 1000 children aged 0 to 11 years. The grey lines show the observed data. The blue line shows the fitted model based on observed data, with a blue shaded area showing the 95% CI. The pink line shows the expected DDD based on data before October 2023, with the pink shaded area showing the 95% CI.
The increase was higher for clarithromycin [+289% (95%CI +169%–+462%), P value < 0.001] than for azithromycin [+145% (95%CI +83%–+228%), P value < 0.001] when considering the entire population of children 0 to 11 years. In the age group 0 to 1 year old, there was an increase in clarithromycin use [+170% (95%CI +86%–+291%), P value < 0.001] but not in azithromycin use [+20% (95%CI −19%–+77%), P value 0.357) (Figures S3–S8).
The use of amoxicillin remained stable in both age groups after October 2023 (Figures S9–S11).
Discussion
We found that macrolide antibiotic monthly DDD per 1000 children increased by ∼3-fold in Swiss children in autumn 2023. This surge followed the increase of cases of M. pneumoniae following the lifting of restrictions to reduce the impact of COVID-19 pandemic, which was observed globally and prospectively surveyed also for Switzerland by the European Society of Clinical Microbiology and Infectious Diseases Study Group for Mycoplasma and Chlamydia Infections (ESGMAC) MAPS study.^2,3^ Other factors than treatment of M. pneumoniae pneumonia may have contributed to the increase in macrolide consumption. First, M. pneumoniae carriage may be common in children, and awareness of the increased incidence of M. pneumoniae infections among paediatricians could have led to increased diagnostic testing.^7^ Consequently, this could have resulted in the treatment of M. pneumoniae infections beyond pneumonia. Second, there are other indications for prescribing macrolides to children such as infections with Bordetella pertussis or Chlamydia pneumoniae, cat scratch disease, bacterial diarrhoea or beta-lactam allergies. The increased incidence of pertussis in Europe in 2023/24 and C. pneumoniae compared to the pandemic years could therefore also partly explain the rise in macrolide consumption, especially in the younger age group.^8,9^ In addition, the transient increase in macrolide claims during winter 2022 could partly be related to the group A Streptococcus surge reported during that period. Third, amoxicillin shortage observed globally could have led to increased macrolide use in replacement.^10^ This is, however, unlikely in our population as amoxicillin use remained stable.
The increase in azithromycin consumption was less pronounced compared to the increase in clarithromycin consumption. This trend may reflect adherence to expert recommendations favouring clarithromycin over azithromycin for the treatment of M. pneumoniae CAP, because of the notably long half-life of azithromycin.^11^ Clarithromycin and azithromycin are both in the ‘Watch’ group of ‘AWaRe’, the WHO classification of antibiotics, defined as broader-spectrum antibiotics with a higher potential of developing resistance. Macrolide consumption is an important driver for macrolide resistance and is associated with increased macrolide resistance in several pathogen including streptococci.^12^ It could also be associated with macrolide-resistant M. pneumoniae (MRMP).^13^ MRMP are highly prevalent in some countries, and infections are associated with longer illness, more severe disease and/or the presence of extrapulmonary manifestations than infections with macrolide-sensitive M. pneumoniae.^14,15^ Prudent use of macrolides is therefore essential to mitigate the potential risk of increasing antibiotic resistance and to ensure the continued effectiveness of these treatments.
Limitations
Our analysis is based on claims data of ∼50% of community pharmacies in Switzerland and does not consider all antibiotic sales channels such as self-dispensing physicians. There was, however, no change over time in data collection methods. The short period of data available after M. pneumoniae re-emergence limits our ability to assess whether macrolide use returned to baseline levels. In addition, we did not have access to information on treatment indication, which limits the interpretation of age-specific trends.
Conclusions
Macrolides DDD for children surged significantly in Switzerland in autumn 2023. The more pronounced increase in clarithromycin, despite the greater convenience of azithromycin, suggests that national guidelines may have supported appropriate antibiotic selection. The overall rise in macrolide use underscores the need for continuous monitoring of macrolide resistance and promotion of appropriate prescription practices.
Supplementary Material
dlaf123_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meyer Sauteur PM, Beeton ML, Uldum SA et al Mycoplasma pneumoniae detections before and during the COVID-19 pandemic: results of a global survey, 2017 to 2021. Euro Surveill 2022; 27: 2100746. 10.2807/1560-7917.ES.2022.27.19.210074635551702 PMC 9101966 · doi ↗ · pubmed ↗
- 2ESGMAC MAPS study group . Global spatiotemporal dynamics of Mycoplasma pneumoniae re-emergence after COVID-19 pandemic restrictions: an epidemiological and transmission modelling study. Lancet Microbe 2025; 6: 101019. 10.1016/j.lanmic.2024.10101940024259 · doi ↗ · pubmed ↗
- 3Meyer Sauteur PM, Beeton ML; European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Mycoplasma and Chlamydia Infections (ESGMAC), and the ESGMAC Mycoplasma pneumoniae Surveillance (MAPS) study group. Mycoplasma pneumoniae: delayed re-emergence after COVID-19 pandemic restrictions. Lancet Microbe 2024; 5: e 100–1. 10.1016/S 2666-5247(23)00344-038008103 · doi ↗ · pubmed ↗
- 4WHO . Upsurge of respiratory illnesses among children—Northern China. https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON 494.
- 5Dungu KHS, Holm M, Hartling U et al Mycoplasma pneumoniae incidence, phenotype, and severity in children and adolescents in Denmark before, during, and after the COVID-19 pandemic: a nationwide multicentre population-based cohort study. Lancet Reg Health Eur 2024; 47: 101103. 10.1016/j.lanepe.2024.10110339469091 PMC 11513821 · doi ↗ · pubmed ↗
- 6Global Times . Pediatricians warn of Mycoplasma pneumonia outbreak, with infections surging among children. https://www.globaltimes.cn/page/202310/1299756.shtml.
- 7Meyer Sauteur PM, Trück J, van Rossum AMC et al Circulating antibody-secreting cell response during Mycoplasma pneumoniae childhood pneumonia. J Infect Dis 2020; 222: 136–47. 10.1093/infdis/jiaa 06232034406 · doi ↗ · pubmed ↗
- 8European Centre for Disease Prevention and Control . Increase of pertussis cases in the EU/EEA: 8 May 2024. https://data.europa.eu/doi/10.2900/831122.