A case of acute coronary syndrome secondary to cocaine-induced coronary thrombosis
Mahmoud Morsy, Saad Fyyaz, Magda-Madalina Olaru, Maciej Marciniak

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
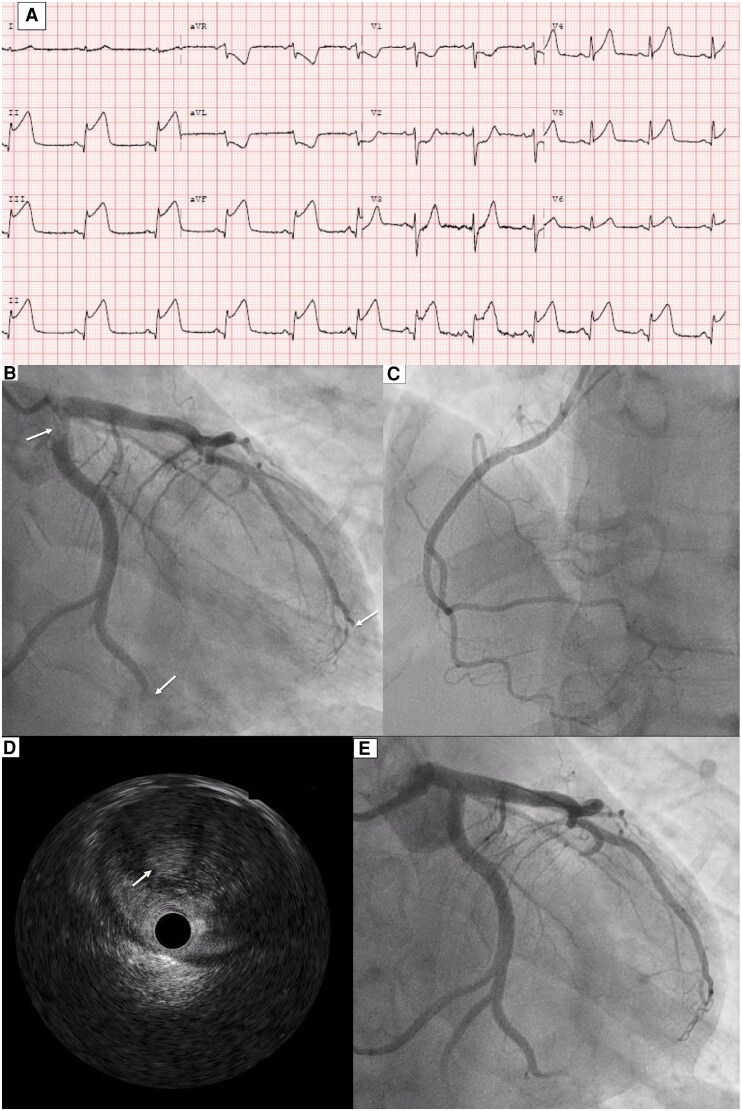 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Toxicology and Drug Analysis · Venous Thromboembolism Diagnosis and Management · Alcohol Consumption and Health Effects
Case description
A 39-year-old gentleman with no significant past medical history apart from smoking and cocaine abuse presented to our hospital with central chest pain and diaphoresis, which started 12 h before admission. An electrocardiogram showed inferior ST elevation (Figure 1A). He was transferred immediately to the Cath lab, where he underwent a coronary angiogram that showed thrombus in the ostial to proximal segment of the left circumflex (LCX) artery, with thrombus in the distal LCX, and thrombus in the distal segment of the left anterior descending artery (Figure 1B; Supplementary material online, Video S1) and a normal right coronary artery (Figure 1C). Intravascular ultrasound showed heavy thrombosis with otherwise healthy underlying vessels (Figure 1D). Thrombus aspiration was not successful due to late presentation. Given the heavy thrombosis in the ostial LCX and potential compromise to the left main artery, a multidisciplinary team discussion was held, and a decision was made to proceed with thrombolysis using Tenecteplase 40 mg, followed by anticoagulation with low molecular weight heparin and a follow-up coronary angiogram in 48–72 h. Vasculitis and prothrombotic screens were negative. A bedside transthoracic echocardiogram showed mildly impaired left ventricular systolic function, with an ejection fraction of 45%, with hypokinetic mid to apical inferior and inferoseptal segments (see Supplementary material online, Videos S3 and S4). A bubble contrast study showed no evidence of right-to-left shunt (see Supplementary material online, Video S5). Follow-up coronary angiogram showed resolution of coronary thrombosis with improvement of coronary flow (Figure 1E; Supplementary material online, Video S2). The patient was discharged on apixaban and clopidogrel for 3 months, followed by aspirin for life.
Electrocardiogram at presentation showing evidence of inferior ST elevation myocardial infarction (A). Coronary angiogram (dominant left system) showing evidence of thrombosis in the ostial, proximal, and the distal segments of the left circumflex artery and in distal segment of the left anterior descending artery (arrows) (B). No evidence of thrombosis in the non-dominant right coronary artery (C). Intravascular ultrasound showed heavy thrombosis with otherwise healthy underlying vessels (D). Follow-up coronary angiogram after 3 days showing resolution of coronary thrombosis with improved flow in the coronaries (E).
Cocaine use has been reported in the literature to cause coronary thrombosis by inducing platelet aggregation, even in normal coronaries.^1^ Myocardial infarction was reported in 6% of patients presenting with chest pain after cocaine use in two different studies.^2^ In a study performed on 71 cocaine abusers, there was a significant increase in the risk of stent thrombosis in cocaine abusers compared with the control group; thus, effort should be made to avoid stents where possible.^3^ Fibrinolysis was reported to be safe in patients with myocardial infarction secondary to cocaine abuse.^4^ For secondary prevention, cessation of cocaine use, modification of atherosclerotic risk factors, and the use of aspirin, clopidogrel, and direct thrombin inhibitors have been reported in the literature.^2^
Supplementary Material
ytaf303_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hollander JE, Hoffman RS. Cocaine induced myocardial infarction: an analysis and review of the literature. J Emerg Med 1992;10:169–177.1607624 10.1016/0736-4679(92)90212-c · doi ↗ · pubmed ↗
- 2Mc Cord J, Jneid H, Hollander JE, de Lemos JA, Cercek B, Hsue P, et al Management of cocaine-associated chest pain and myocardial infarction. Circulation 2008;117:1897–1907.18347214 10.1161/CIRCULATIONAHA.107.188950 · doi ↗ · pubmed ↗
- 3Mc Kee SA, Applegate RJ, Hoyle JR, Sacrinty MT, Kutcher MA, Sane DC. Cocaine use is associated with an increased risk of stent thrombosis after percutaneous coronary intervention. Am Heart J 2007;154:159–164.17584570 10.1016/j.ahj.2007.04.004 · doi ↗ · pubmed ↗
- 4Hollander JE, Burstein JL, Hoffman RS, Shih RD, Wilson LD. Cocaine-associated myocardial infarction. Clinical safety of thrombolytic therapy. Cocaine associated myocardial infarction (CAMI) study group. Chest 1995;107:1237–1241.7750312 10.1378/chest.107.5.1237 · doi ↗ · pubmed ↗