Knowledge, Attitudes, and Practices of Nurses Regarding Needle Stick Injuries, HIV, and Hepatitis B Prevention in a Tertiary Care Center in Nagpur, India: A Cross-Sectional Study
Sanjay Sain, Nishaant Ramasamy, Ishan Verma, Jaya Prasad Tripathy, Udit Narang, Sunita Kumbhalkar, Amol H Dube, Keshao B Nagpure

TL;DR
This study examines nurses' knowledge, attitudes, and practices regarding needlestick injuries and bloodborne disease prevention in a hospital in India, finding good awareness but gaps in safe practices.
Contribution
The study provides new insights into nurses' KAP regarding NSIs and PEP adherence in a specific Indian hospital setting.
Findings
40.5% of nurses reported experiencing needlestick injuries.
Only 31% of injured nurses received post-exposure prophylaxis.
24% of nurses still engaged in unsafe practices like recapping needles.
Abstract
Introduction Needlestick injuries (NSIs) pose serious health risks to healthcare workers, especially nurses, due to the potential transmission of HIV and Hepatitis B. Despite available guidelines for vaccination and post-exposure prophylaxis (PEP), awareness and adherence remain low, particularly in developing countries like India. Nurses face high NSI risk due to their frontline role in patient care, yet limited Indian studies assess their knowledge, attitudes, and practices (KAP) on this issue. This cross-sectional study was conducted among nurses at a tertiary care hospital in Nagpur using a validated questionnaire to evaluate KAP regarding NSI prevention and management. The findings aim to highlight existing gaps and support targeted interventions to reduce NSI-related infections and improve occupational safety among nurses. Methods A cross-sectional analytical study was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
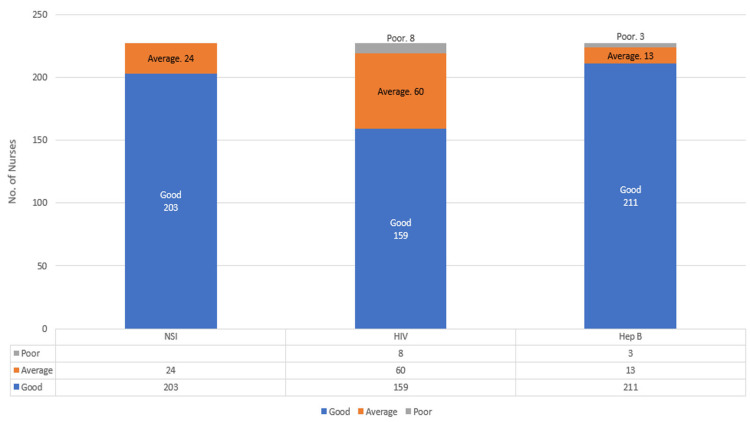 Figure 1
Figure 1| Characteristics | Value | |
| Age in years (Mean±SD) | 27±2.7 | |
| Gender (n (%)) | Male | 60 (26.4) |
| Female | 167 (73.6) | |
| Total years of experience (Median (IQR)) | 2 (1.4 – 3) | |
| Work experience (n (%)) | <3 years | 138 (61) |
| ≥3 years | 89 (39) | |
| Marital status (n (%)) | Unmarried | 157 (69.2) |
| Married | 70 (30.8) | |
| Characteristics | NSI | Test statistic | p-value^ | ||
| Present (n=92) | Absent (n=135) | ||||
| Age in years (Mean±SD) | 27.29±2.5 | 26.82±2.9 | -1.242 | 0.215* | |
| Gender (n (%)) | Male | 19 (32%) | 41 (68%) | 2.657 | 0.103 |
| Female | 73 (43.7%) | 94 (56.3%) | |||
| Total years of experience (Median (IQR)) | 2 (1.5 – 3.35) | 2 (1.3 – 3) | -0.432 | 0.665# | |
| Work experience (n (%)) | <3 years | 56 (40.6%) | 82(59.4%) | 0.0004 | 0.984 |
| ≥3 years | 36 (40.4%) | 53 (59.6%) | |||
| Marital status (n (%)) | Unmarried | 62 (39.5%) | 95 (60.5%) | 0.227 | 0.633 |
| Married | 30 (42.9%) | 40 (57.1%) | |||
| Knowledge categories | NSI | HIV | Hepatitis B | |||||||||
| NSI Category (n (%)) | ||||||||||||
| Present (n=92) | Absent (n=135) | Test Statistics | p-value^ | Present (n=92) | Absent (n=135) | Test Statistics | p-value^ | Present (n=92) | Absent (n=135) | Test Statistics | p-value^ | |
| Good | 84 (91.3%) | 119 (88.2%) | 0.576 | 0.448 | 66 (71.7%) | 93 (68.9%) | 2.703 | 0.259 | 86 (93.5%) | 125 (92.6%) | 0.092 | 1.000 |
| Average | 8 (8.7%) | 16 (11.8%) | 25 (27.2%) | 35 (25.9%) | 5 (5.4%) | 8 (5.9%) | ||||||
| Poor | - | - | 1 (1.1%) | 7 (5.2%) | 1 (1.1%) | 2 (1.5%) | ||||||
| Characteristics | NSI knowledge | HIV knowledge | Hepatitis B knowledge | ||||||||||||
| Good (n=203) | Average (n=24) | Test Statistics | p-value^ | Good (n=159) | Average (n=60) | Poor (n=8) | Test Statistics | p-value^ | Good (n=211) | Average (n=13) | Poor (n=3) | Test Statistics | p-value^ | ||
| Age in years (Mean±SD) | 27.05±2.8 | 26.71±2.6 | -0.578 | 0.563* | 26.83±2.53 | 27.61±3.11 | 26.12±3.94 | 2.19 | 0.114* | 27±2.7 | 27.61±2.56 | 3±2.88 | 0.66 | 0.516* | |
| Gender (n (%)) | Male | 51 (85%) | 9 (15%) | 1.691 | 0.193 | 41 (68.3%) | 17 (28.3%) | 2 (3.4%) | 0.154 | 0.926 | 57 (95%) | 3 (5%) | - | 1.189 | 0.552 |
| Female | 152 (91.1%) | 15 (8.9%) | 118 (70.6%) | 43 (25.7 %) | 6 (3.7%) | 154 (92.2%) | 10 (5.9%) | 3 (1.8%) | |||||||
| Total years of experience (Median (IQR)) | 2 (1.4 – 3) | 2 (1.1 – 3.5) | 0.091 | 0.927# | 2 (1.5 – 3) | 2 (1.25 – 4) | 2 (0.7 – 2.5) | 1.598 | 0.449# | 2 (1.5 – 3) | 2 (1.2 – 5) | 2 (1 – 6) | 0.075 | 0.963# | |
| Work experience (n (%)) | <3 years | 124 (89.9%) | 14 (10.1%) | 0.068 | 0.794 | 97 (70.3) | 35 (25.4%) | 6 (4.3%) | 0.833 | 0.659 | 127 (92.1%) | 9 (6.5%) | 2 (1.4%) | 0.464 | 0.793 |
| ≥3 years | 79 (88.2%) | 10 (11.8%) | 62 (69.7%) | 25 (28.1%) | 2 (2.2%) | 84 (94.4%) | 4 (4.5%) | 1 (1.1%) | |||||||
| Marital status (n (%)) | Unmarried | 137 (87.3%) | 20 (12.7%) | 2.527 | 0.112 | 116 (73.9%) | 35 (22.3%) | 6 (3.8%) | 4.499 | 0.105 | 145 (92.4%) | 10 (6.4%) | 2 (1.2%) | 0.395 | 0.821 |
| Married | 66 (94.3%) | 4 (5.7%) | 43 (61.4%) | 25 (35.7%) | 2 (2.9%) | 66 (94.3%) | 3 (4.4%) | 1 (1.3%) | |||||||
| Attitude Question | Response | Frequency (%) |
| 1. I worry that since I am in the medical profession, I am at high risk of contracting a needle stick injury at any time in my career as compared to the general population. (n=219) | Yes | 203 (92.6) |
| No | 16 (7.4) | |
| 2. Patient care is more important than the safety of nurses. (n=219) | Yes | 32 (14.6) |
| No | 187 (85.4) | |
| 3. All sharp injuries at work should be reported immediately. (n=218) | Yes | 211 (96.8) |
| No | 7 (3.2) | |
| 4. I think needle stick injury is preventable. (n=219) | Yes | 214 (97.7) |
| No | 5 (2.3) | |
| 5. Sharp object waste should be disposed of by a professional company, not in domestic waste. (n=218) | Yes | 208 (95.4) |
| No | 10 (4.6) | |
| 6. What do you think are the factors that can lead to a needlestick injury? (Multiple responses) (n=219) | Recapping | 208 (95) |
| Manipulating the needle inpatient | 116 (53) | |
| Disposal related | 169 (77) | |
| IV line related | 92 (42) | |
| Clean up | 61 (27.8) | |
| Collision with a fellow health worker | 126 (57.5) | |
| Passing the needle after use | 181 (82.6) | |
| Stress-related | 69 (31) | |
| High patient load per nurse | 164 (75) | |
| 7. What do you think are the reasons for the non-reporting of the needlestick injuries? (Multiple responses) (n=212) | I never knew that such incidents needed to be reported | 77 (36) |
| Being too busy managing patient time pressure | 166 (78.3) | |
| Needlestick injury by a fresh needle rather than contaminated ones | 166 (78.3) | |
| Not knowing how to report | 98 (46) | |
| No need to worry if fully vaccinated | 72 (34) | |
| Fear of stigma and embarrassment | 79 (37.3) | |
| 8. I am concerned that since I am in the medical profession, I am at high risk of getting infected with a Hep B/HIV infection at work. (n=217) | Yes | 202 (93) |
| No | 15 (7) | |
| 9. Hepatitis B vaccine is safe and effective. (n=218) | Yes | 213 (97.7) |
| No | 5 (2.3) | |
| 10. Changing gloves during blood collection and tests is a waste of time. (n=218) | Yes | 10 (4.6) |
| No | 208 (95.4) | |
| 11. I do not feel comfortable taking care of people with Hepatitis B. (n=216) | Yes | 24 (11.1) |
| No | 192 (88.9) | |
| 12. I do not feel comfortable taking care of people with HIV. (n=216) | Yes | 22 (10.2) |
| No | 194 (89.8) | |
| 13. All nurses should undergo mandatory HIV testing before joining the nursing profession. (n=213) | Yes | 179 (84) |
| No | 34 (16) | |
| 14. All nurses should undergo mandatory Hepatitis B testing before joining nursing. (n=211) | Yes | 188 (89) |
| No | 23 (11) | |
| 15. Post-exposure prophylaxis medications for HIV are available in our institution. (n=214) | Yes | 196 (91.6) |
| No | 2 (0.9) | |
| Don’t know | 16 (7.5) | |
| 16. Post-exposure prophylaxis medications for Hepatitis B are available at our institution. (n=214) | Yes | 186 (86.9) |
| No | 9 (4.2) | |
| Don’t know | 19 (8.9) | |
| 17. Do you recommend post-exposure prophylaxis for those who have been exposed to Hepatitis B? (n=216) | Yes | 201 (93) |
| No | 15 (7) | |
| 18. Do you recommend post-exposure prophylaxis for those who have been exposed to HIV? (n=216) | Yes | 204 (94.4) |
| No | 12 (5.6) |
| Practice Question | Response | N (%) |
| 1. Number of needlestick injuries you have had in your career so far. | Once | 57 (61.8) |
| 2-4 times | 27 (29.4) | |
| 5 or more times | 4 (4.4) | |
| Yes, but I don’t remember the count | 4 (4.4) | |
| 1.1 What was the injury type? (n=87) | Superficial (little or no bleeding) | 52 (59.8) |
| Moderate (skin punctured, some bleeding) | 31 (35.6) | |
| Severe (deep stick/cut or profuse bleeding) | 4 (4.6) | |
| 1.2 Did you report the needlestick injury? | Yes | 60 (65.2) |
| No | 32 (34.8) | |
| 1.3 Did you receive medical attention within 2 h after injury | Yes | 60 (65.2) |
| No | 32 (34.8) | |
| 1.4 What action was taken after injury - (Multiple-response question) (n=87) | Washed with soap and water | 79 (91) |
| Got tested for HIV, hepatitis B, and hepatitis C | 55 (59.7) | |
| Identified the source patient | 62 (71.2) | |
| Got post-exposure prophylaxis (PEP) when the source patient was unknown or tested positive for HIV & Hepatitis B | 27 (31) | |
| Checked Anti-HBs titre | 39 (42.3) | |
| 1.5 Device involved in the last incident. (n=87) | Intravenous (IV) cannula | 16 (18.3) |
| Butterfly needle | 2 (2.3) | |
| Hypodermic needle | 21 (24.1) | |
| Phlebotomy needle | 14 (16.1) | |
| Lancets | 18 (20.7) | |
| Razors | 2 (2.3) | |
| Scissors | 0 | |
| Suture needle | 7 (8.6) | |
| Others | 7 (8.6) | |
| 1.6 At what point in time did the NSI occur? (n=85) | Before procedure | 25 (29.4) |
| During procedure | 25 (29.4) | |
| While recapping the needle/ during disposal | 35 (41.2) | |
| 1.7 Work area where the recent injury occurred? (n=85) | Outdoor patient room | 4 (4.7) |
| Hospital wards | 56 (65.9) | |
| Emergency wards | 7 (8.7) | |
| Intensive/Critical care unit | 8 (9.4) | |
| Operating room/Recovery | 7 (8.7) | |
| Others | 3 (3.5) | |
| 1.8 When did the NSI occur? (n=85) | During graduation from nursing | 32 (37.6) |
| During post-graduation | 2 (2.4) | |
| After joining a job | 51 (60) | |
| 1.9 Did you ever get infected with any blood-borne infection after NSI? (n=88) | Yes | 8 (9.1) |
| No | 80 (90.9) | |
| 1.10 If yes, which infection? (n=8) | HIV | 3 (37.5) |
| Hepatitis B | 4 (50) | |
| Hepatitis C | 1 (12.5) | |
| 1.11 Were you offered post-exposure prophylaxis? (n=28) | Yes | 13 (46.5) |
| No | 15 (53.5) | |
| 1.12 Did you complete the post-exposure prophylaxis? (n=28) | Yes | 11 (39.3) |
| No | 17 (60.7) | |
| 1.13 If No, what was the reason for discontinuation? (n=20) | Fear of adverse effects. | 3 (15) |
| Assuming that it was enough. | 2 (10) | |
| Assuming that the drug was not effective. | 1 (5) | |
| I had to purchase the Immunoglobulin/Vaccine/ART, which was costly. | 0 | |
| Other reasons | 14 (70) |
| Practice Question | Response | NSI Present N=92 | NSI Absent N=135 | X2 | p-value |
| n (%) | n (%) | ||||
| 2. Do you recap needles with 2 hands before disposal? (n=219) | Always | 13 (59.1) | 9 (40.9) | 6.209 | 0.045 |
| Sometimes | 17 (54.8) | 14 (45.2) | |||
| No | 62 (37.3) | 104 (62.7) | |||
| 3. Do you bend needles before disposal? (n=216) | Always | 19 (52.8) | 17 (47.2) | 2.393 | 0.302 |
| Sometimes | 8 (47.1) | 9 (52.9) | |||
| No | 64 (39.3) | 99 (60.7) | |||
| 4. Is the safety box/disposal container available at your workplace? (n=219) | Yes | 87 (40.9) | 126 (59.1) | 1.602 | 0.236 |
| No | 4 (66.7) | 2 (33.3) | |||
| 5. Do you put sharp items into their assigned disposal container? (n=219) | Always | 89 (41.4) | 126 (58.6) | 2.162 | 0.394 |
| Sometimes | 1 (100) | 0 | |||
| No | 2 (66.7) | 1 (33.3) | |||
| 6. Do you change gloves for each patient during blood taking? (n=219) | Always | 79 (41.4) | 112 (58.6) | 3.788 | 0.150 |
| Sometimes | 5 (31.3) | 11 (68.7) | |||
| No | 8 (66.7) | 4 (33.3) | |||
| 7. Have you been vaccinated against HBV? (n=220) | Yes | 82 (40.6) | 120 (59.4) | 1.521 | 0.218 |
| No | 10 (55.6) | 8 (44.4) | |||
| 7.1 How many doses of HBV vaccine did you receive? (n=202) | 1 | 4 (36.4) | 7 (63.6) | 0.458 | 0.827 |
| 2 | 12 (36.4) | 21 (63.6) | |||
| 3 | 66 (41.8) | 92 (58.2) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control in Healthcare · Rabies epidemiology and control · Workplace Violence and Bullying
Introduction
Needlestick injuries (NSI) are a major occupational hazard among healthcare workers (HCWs), particularly nurses, due to the risk of transmission of bloodborne infections such as Hepatitis B virus (HBV), Hepatitis C virus (HCV), and Human Immunodeficiency Virus (HIV). According to the Centers for Disease Control and Prevention (CDC), a needlestick injury occurs when a needle or other sharp object punctures the skin after contact with blood, tissue, or body fluids of another person [1]. These injuries commonly result from blood collection needles, suture needles, intravenous (IV) delivery systems, and hypodermic needles [2].
Standardized protocols exist for the prevention and post-exposure management of HBV and HIV [3-6]. The World Health Organization (WHO) estimates that needlestick injuries account for approximately 66,000 HBV, 16,000 HCV, and 200-5,000 HIV infections annually among HCWs, with percutaneous occupational exposure contributing to 4.4% of HIV, 37% of HBV, and 39% of HCV cases [7]. Despite the availability of HBV vaccination, coverage among HCWs in developing countries remains significantly lower than in developed nations [8]. Similarly, post-exposure prophylaxis (PEP) with antiretroviral therapy (ART) for 28 days has been shown to reduce HIV transmission [9]. The recommended PEP regimen includes two nucleoside reverse transcriptase inhibitors (NRTIs) combined with a third drug, typically a protease inhibitor (e.g., Tenofovir, Emtricitabine, plus either Dolutegravir or Raltegravir), and should be initiated as early as possible, ideally within 72 hours [10].
The risk of infection transmission following an NSI varies, with HBV having the highest rate (6-30%), followed by HCV (1.8%) and HIV (0.3%) [10]. Indian data on NSI remains largely underreported, and available statistics suggest that approximately 3-6 billion injections are administered annually in India, of which nearly two-thirds are unsafe [11]. The Exposure Prevention Information Network (EPINet) has reported 27 NSIs per 100 hospital beds, while Indian studies indicate a rate of 8.9 to 10.4 NSIs per 100 beds [12]. Additionally, a recent meta-analysis estimated the global prevalence of NSIs to be 44.5% [13]. Considering these factors, a low reported incidence of NSI should not be mistaken for an actual low occurrence, as underreporting remains a significant concern across healthcare settings [12]. Developing countries, including India, face higher NSI risks due to factors such as hospital overcrowding, high patient-to-HCW ratios, inadequate awareness, limited adherence to infection control protocols, and restricted access to PEP. The incidence of HBV among HCWs is reported to be four times higher than in the general population [8]. Furthermore, around 0.5% of healthcare workers worldwide contract HIV each year, highlighting the ongoing occupational risk in clinical settings [14].
As per 2022 data from the Indian Nursing Council (INC), the country has approximately 33.41 lakh registered nurses [15]. Among HCWs, nurses are particularly vulnerable due to their direct involvement in procedures such as administering injections, phlebotomy, inserting IV lines, and assisting in surgical interventions [16]. Studies indicate that nurses experience higher rates of percutaneous and mucosal exposures to blood and body fluids compared to other HCWs [17].
Efforts to mitigate NSIs have been implemented in developed nations, such as the Needlestick Safety and Prevention Act enacted in the United States (1999-2000), which established guidelines for safer needle devices and enhanced infection control practices [18]. However, such legislative measures are yet to be fully realized in India and many other developing countries, where NSIs remain a significant public health concern.
There is a dearth of comprehensive studies from India that assess the knowledge, attitudes, and practices (KAP) related to NSI, Hepatitis B, and HIV collectively. This study aims to assess the KAP of nurses regarding NSI prevention and associated bloodborne infections in a tertiary care hospital in Nagpur, India. By identifying existing gaps in awareness and adherence to safety protocols, this study seeks to contribute to the development of targeted interventions aimed at reducing NSI incidence and enhancing occupational safety among nurses.
Materials and methods
Study design and setting
This was a cross-sectional analytical study conducted at a tertiary care hospital in Nagpur, situated in the central part of India, from December 2023 to February 2024.
Sample size calculation
The sample size was determined using the single proportion formula:
\begin{document}n = z_{1 - \alpha/2}^2 \left( \frac{p(1 - p)}{d^2} \right)\end{document} ; at a 95% confidence interval, where \begin{document}z_{1 - \alpha/2}\end{document} = 1.96 (standard normal value for 95% CI); p = 50% (prevalence of good knowledge regarding NSI among nurses [19]); d = 7% (margin of error). A minimum sample size of 196 was calculated, and with a 10% dropout rate, the final required sample was 216 participants.
Subject selection
Inclusion criteria included nurses aged ≥18 years working in the hospital. Exclusion criteria included nurses who declined consent or were on medical leave due to illness.
Ethical considerations
The study was approved by the Institutional Ethics Committee (IEC/Pharmac/2023/694). Informed consent was obtained from all participants before study participation, and confidentiality was maintained.
Data collection
A self-administered online questionnaire was developed using validated questions from prior studies (Appendices) [7-14,16]. The self-developed questionnaire underwent face validation by experts to ensure relevance and appropriateness. This process involved experts reviewing the questionnaire's items and overall structure to assess clarity, readability, and how well the questions aligned with the study's objectives. The questionnaire, hosted on Google Forms (Google, Mountain View, California, US), was distributed to all 500 nursing officers via WhatsApp, with reminders sent every 10 days. The data collection period lasted two months, and 227 responses were obtained.
The questionnaire comprised 66 questions across four sections: Socio-demographic characteristics (6 questions), knowledge of NSI, HBV, and HIV prevention (21 questions), attitudes toward NSI and infection prevention (18 questions), and practices related to NSI prevention (7 questions).
The knowledge section was categorized separately for NSI, HIV, and HBV. Each correct response was awarded one point, while incorrect responses received zero points. For multiple-response questions, scores ranged from 1 to 3 points based on the number of correct answers. The total knowledge score for NSI, HIV, and HBV was categorized as follows, based on a validated classification system [9]: good knowledge: >75% (score >6), average knowledge: 50-75% (score 4-5) and poor knowledge: <50% (score <3).
Statistical analysis
All the data obtained from the questionnaire were entered into a Microsoft Excel sheet (Microsoft Corporation, Redmond, WA, US), and statistical analysis was done using Stata version 18 (StataCorp LLC, College Station, TX, US) [20]. The prevalence of NSI was expressed in percentage with a 95% confidence interval. The knowledge categories were summarized as frequencies and percentages. The knowledge categories were compared across socio-demographic characteristics of the participants by the t-test/Wilcoxon rank sum test and the analysis of variance (ANOVA)/Kruskal-Wallis test for continuous variables based on the number of groups and normality, whereas for categorical variables, the chi-squared/Fisher exact test was used. The knowledge category was compared between the NSI categories using the chi-squared test. The responses for the attitude domain were summarized as frequencies and percentages. The practice domain responses were summarized as frequencies and percentages and were compared between the NSI groups, and the chi-squared test was used to assess statistical significance.
Results
The study included 227 nurses with a mean age of 27 ± 2.7 years. The majority were female (73.6%), had less than three years of experience (61%), and were unmarried (69.2%) (Table 1). The overall prevalence of NSI among participants was 40.5% (95% CI: 34.1% - 47.2%). NSI occurrence was not significantly influenced by age (p = 0.215), experience (p > 0.65), or marital status (p = 0.633). While males had higher NSI rates, the difference was not significant (p = 0.103), suggesting minimal impact of demographic factors (Table 2). The study revealed high overall knowledge levels, with 89.4% demonstrating a good understanding of NSI, 70% of HIV, and 93% of Hepatitis B. However, notable gaps persisted in HIV awareness, where 26.4% had average knowledge and 3.6% showed poor understanding (Figure 1). These findings highlight the need for targeted educational interventions to bridge knowledge deficits and strengthen prevention strategies.
Knowledge levels for NSI, HIV, and Hepatitis BNSI: needlestick injury
NSI incidence did not significantly differ based on knowledge levels of NSI, HIV, or Hepatitis B (p > 0.05). While minor variations were observed, they were not statistically significant, suggesting that knowledge alone may not directly influence NSI occurrence (Table 3). Demographic factors, such as age (p = 0.563), gender (p = 0.193), work experience (p = 0.794), and marital status (p = 0.112), did not significantly influence knowledge levels for NSI, HIV, or Hepatitis B (Table 4). These findings suggest that demographic characteristics did not have a meaningful impact on knowledge levels regarding NSI, HIV, or Hepatitis B, reinforcing the need for targeted education and intervention programs.
A majority of participants (92.6%) expressed concern about the risk of NSI in their profession, and 97.7% believed NSI incidents were preventable. Most participants (96.8%) supported immediate reporting of sharp injuries, but common barriers to reporting included a lack of awareness and time constraints. Concern about acquiring HIV (93%) and Hepatitis B (93%) was widespread, yet only 10.2% and 11.1% felt uncomfortable managing patients with these infections, respectively. Support for mandatory testing before entering nursing was high (HIV: 84%, Hepatitis B: 89%), and most participants endorsed PEP for HIV (94.4%) and Hepatitis B (93%) (Table 5).
Among healthcare workers with NSI history, 61.8% had at least one incident, primarily superficial injuries (59.8%), with 65.2% reporting the event. However, 34.8% did not seek medical attention within two hours. Common responses included washing with soap and water (91%) and identifying the source patient (71.2%), yet only 31% received PEP. Hypodermic needles (24.1%) and lancets (20.7%) were the most frequently involved devices, with 41.2% of NSIs occurring during disposal or recapping, mainly in hospital wards (65.9%) and after joining the job (60%). While 90.9% did not acquire infections, 50% of those infected had Hepatitis B. Despite PEP being recommended, only 46.5% were offered it, and just 39.3% completed the regimen, often due to fear of side effects or assuming it was unnecessary. These findings highlight both strengths and critical gaps in NSI management, emphasizing the need for timely medical attention, improved PEP adherence, and stricter prevention strategies (Table 6).
Unsafe practices such as recapping needles with two hands were significantly associated with NSI (p = 0.045). However, other practices, including bending needles before disposal, availability of safety containers, and proper disposal of sharp items, did not show significant associations with NSI occurrence. HBV vaccination status and the number of vaccine doses received were also not significantly correlated with NSI incidence (p = 0.827) (Table 7).
To summarize, NSI prevalence was high (40.5%), but demographic factors did not significantly influence occurrence. Knowledge levels were high, but no significant relationship with NSI rates was observed. A strong attitude towards NSI prevention and reporting existed, but barriers to reporting persisted. Unsafe practices, particularly recapping needles, were a significant contributor to NSI. Despite available PEP, adherence remained low, highlighting a need for better post-exposure management strategies. These findings emphasize the importance of reinforcing safe needle practices, improving PEP adherence, and addressing barriers to reporting NSI incidents to reduce occupational risks among healthcare workers.
Discussion
NSIs remain a major occupational hazard for healthcare workers (HCWs), posing risks of bloodborne infections, including Hepatitis B (HBV) and HIV. This study evaluated the knowledge, attitudes, and practices (KAP) related to NSI, HBV, and HIV among nurses in a tertiary care hospital in Nagpur, India.
The prevalence of NSI in this study was 40.5% (95% CI: 34.1% - 47.2%), comparable to global prevalence rates of 44.5% [13] and findings from Sudan (40%) [11]. However, it was higher than in Kerala, India (24.4%) [21] and Saudi Arabia (11.57%) [19] but lower than in Egypt (67.9%) [22]. The higher NSI prevalence observed in this study could be due to multiple factors, including nurses' workload, exposure to high-risk procedures, and adherence to preventive measures.
The mean age of participants was 27 years, which was lower than in other comparable studies [11,12,19,21] but higher than the study by Balegha et al. [23], which focused on nursing students. While Naidu et al. reported a higher NSI incidence among younger HCWs, in this study, age was not significantly associated with NSI prevalence (p = 0.215) [12]. The majority of participants were female (73.6%), which is consistent with the Sudanese study [11]. NSI was more prevalent among female nurses than male nurses, aligning with findings from Naidu et al. [12]. However, Goel et al. and Muralidhar et al. reported higher NSI prevalence in male HCWs [24,25]. Studies suggest that NSI risk decreases with experience [12]. In our study, most nurses had an average of two years of experience (range: 1.4-3 years), lower than in other studies [11,19], likely due to our hospital’s younger workforce. Consequently, NSI incidence did not significantly vary with experience. Balegha AN et al. observed that married nurses exhibited better practices than unmarried ones, attributing this to increased responsibility and guideline adherence post-marriage [23]. While 90% of nurses in their study were unmarried, our study had 69% unmarried nurses, yet NSI was more frequently reported among married nurses. Further research is needed to explore socio-demographic influences on NSI. The knowledge levels of participants were high, with 89.4% demonstrating good knowledge of NSI, 70% for HIV, and 93% for Hepatitis B. These results are comparable to studies from Sudan, Afghanistan, and Saudi Arabia [8,11,19]. However, despite high knowledge levels, NSI prevalence remained substantial, suggesting that knowledge alone may not directly reduce NSI risk. Unsafe behaviors persisted, with 24% of participants admitting to recapping needles, despite 64% of them experiencing NSI. This risk was lower than in Saudi Arabia, where 38.8% of HCWs engaged in recapping. In this study, 88% of participants recognized Hepatitis B as the most transmissible infection following NSI, a finding consistent with the Saudi Arabian study [19]. Additionally, 97% of nurses were aware of local guidelines for NSI management, aligning with findings from Sudan. However, only 52% knew that the correct immediate response to an NSI was washing the injury site with soap and water, which is lower than the Sudanese study, where 77.8% of participants identified the ideal method [11]. This discrepancy could be attributed to variations in training, years of experience, and exposure to standardized protocols across different healthcare systems. Regarding Hepatitis B transmission, 93% identified NSI as a risk, 77% acknowledged sexual transmission, and 87% recognized mother-to-child transmission, findings consistent with the Afghan study [8]. Knowledge of the vaccine schedule (86%) and post-exposure prophylaxis (93%) was higher than in Afghan [8] and Saudi studies [19]. However, only 69% knew Hepatitis B could lead to liver cancer, highlighting a gap in awareness that needs to be addressed.
Eighty percent (80%) of nurses correctly understood PEP for HIV, better than that shown in the study by Tshering et al. [9]. However, 8.4% falsely believed that HIV could be prevented by a vaccine, possibly due to misinformation prevalent in developing countries. Awareness of HIV PEP was high, with 96% knowing it exists, 86% learning about it during graduation, 64.7% identifying the correct initiation window, and 63.4% recognizing the 28-day regimen. These figures exceeded those reported in Bhutan [9], possibly due to differences in training curricula, exposure to standardized guidelines, or institutional emphasis on HIV PEP awareness.
Most nurses prioritized their own safety over patient care, with 92.6% expressing concern about an NSI risk. A majority supported immediate reporting of NSI, considered it preventable, and endorsed professional disposal of sharps, findings consistent with studies from Saudi Arabia and India [19,21]. Similarly, 93% perceived a high occupational risk of Hepatitis B and HIV, aligning with the Afghan study [8]. Despite this awareness, many nurses felt uncomfortable managing Hepatitis B or HIV-infected patients and advocated for PEP availability for NSI cases. The four main factors contributing to NSI included recapping needles (91.6%), passing used needles (79.6%), improper disposal (74.4%), and high patient load per nurse (72.2%). These differed from Alsabaani et al., where handling/passing needles was the leading cause, likely due to variations in training and workplace practices [19].
Barriers to NSI reporting included time constraints, fresh needle injuries, lack of reporting knowledge, and fear of stigma, consistent with Sudanese data and Alsabaani et al. [11,19]. However, in Madhavan et al., minor injuries were the most cited reason for non-reporting [21]. Additionally, many nurses supported mandatory HIV and Hepatitis B testing before entering the profession, mirroring findings from Afghanistan [8].
In our study, 61.8% of nurses experienced NSI once, while 33.8% had multiple NSIs, contrasting with the Saudi Arabian study, where 39.6% had a single NSI and 58.3% had multiple [19]. However, injury severity patterns were similar, with superficial injuries being the most common (59.8%) and severe injuries accounting for 4.6%. NSI reporting and medical attention rates were higher in our study, with 65.2% reporting to authorities and all receiving immediate care, whereas in Saudi Arabia, only 47.3% reported NSI, and 46.2% sought medical attention [19]. Post-injury practices varied, with 91% washing the injury site, 31% receiving PEP, 42.3% checking Anti-HBs titers, 71.2% identifying the source patient, and 59.7% getting tested for blood-borne infections, findings comparable to Saudi Arabian data. Hypodermic needles (24.1%) were the most common cause of NSI, followed by lancets (20.7%) and IV cannulas (18.3%), differing from Saudi Arabian data, where IV cannulas were predominant [19]. This may be due to frequent bedside glucose monitoring in our hospital. Most NSIs occurred during recapping or disposal (41.2%), primarily in hospital wards (65.9%), with 60% of cases reported post-employment. Among affected nurses, 9.1% developed blood-borne infections, mainly Hepatitis B (50%). Despite PEP availability, only 46.5% of affected nurses were offered it, and just 39.3% completed the full regimen, often due to fear of side effects. Recapping needles was significantly linked to NSI (p = 0.045), and unsafe practices like bending needles and not changing gloves were common, consistent with Afghan and Sudanese studies [8,11].
Hepatitis B vaccination coverage was 89%, higher than in Afghanistan (56.97%) but similar to Saudi Arabia [8,19]. Notably, nurses without NSI were more likely to have completed the full three-dose Hepatitis B vaccine, reinforcing its potential protective role.
Strengths
The strengths of this study are that it integrated findings from three distinct studies for a comprehensive analysis; focused exclusively on nurses, ensuring homogeneity in the study population; high response rates were achieved through a reminder system, minimizing bias; and categorization by NSI status allowed targeted knowledge analysis.
Limitations
The limitations of this study include: nurse rotations across departments could have influenced results; findings from a single tertiary care center may not have represented all nurses in the region; and a potential volunteer bias in data collection and non-participation due to shift schedules/workload constraints or declined consent may have impacted findings.
The study underscores the urgent need for infection control training, emphasizing safe handling and disposal of needles. High-risk behaviours, such as recapping needles, were significantly associated with NSI incidence. While knowledge levels were high, gaps in compliance and safe practices persist. Future research should focus on longitudinal studies assessing intervention effectiveness in reducing NSI rates and improving safety protocol compliance.
Conclusions
The findings of this study provide a comprehensive assessment of the knowledge, attitudes, and practices (KAP) of nurses regarding needlestick injuries (NSI), HIV, and Hepatitis B in a tertiary care hospital. While the majority of nurses demonstrated high knowledge levels and positive attitudes, significant gaps were observed in safe practices, particularly needle recapping and adherence to post-exposure prophylaxis (PEP). Despite high awareness, unsafe practices persist, emphasizing the need for structured training programs, reinforcement of infection control policies, and continuous monitoring of compliance. The study highlights the urgent need for targeted interventions, including enhanced training on safe needle disposal, mandatory Hepatitis B vaccination policies, and routine PEP training and availability. Addressing these gaps can significantly enhance healthcare worker safety, reduce the occupational risks associated with NSI, and strengthen infection control measures. Future research should focus on longitudinal assessments of intervention effectiveness and policy-driven initiatives to further reduce the NSI incidence and improve compliance with safety protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reducing work-related needlestick and other sharps injuries among law enforcement officers. National Institute for Occupational Safety and Health National Institute for Occupational Safety and Health 2022 https://www.cdc.gov/niosh/docs/wp-solutions/2022-154/
- 2What every worker should know: how to protect yourself from needlestick injuries. National Institute for Occupational Safety and Health National Institute for Occupational Safety and Health 2014 https://www.cdc.gov/niosh/docs/2000-135/
- 3NIOSH alert: preventing needlestick injuries in health care settings. National Institute for Occupational Safety and Health National Institute for Occupational Safety and Health 2014 https://www.cdc.gov/niosh/docs/2000-108/
- 4Occupational exposure to Hepatitis B virus, disease burden and pathways for postexposure prophylaxis management: recommendations for healthcare workers in highly endemic settings Infect Prev Pract Senoo-Dogbey VE Ohene LA Wuaku DA 100354620243855936910.1016/j.infpip.2024.100354 PMC 10979087 · doi ↗ · pubmed ↗
- 5Universal hepatitis B vaccination in adults aged 19-59 years: updated recommendations of the Advisory Committee on Immunization Practices - United States, 2022 MMWR Morb Mortal Wkly Rep Weng MK Doshani M Khan MA 4774837120223535816210.15585/mmwr.mm 7113 a 1PMC 8979596 · doi ↗ · pubmed ↗
- 6Guidelines for HIV Post-exposure Prophylaxis World Health Organization Geneva World Health Organization 2024 https://iris.who.int/bitstream/handle/10665/378221/9789240095137-eng.pdf 39259822 · pubmed ↗
- 7Sharps injuries: assessing the burden of disease from sharps injuries to health-care workers at national and local levels. Environmental burden of disease series No. 11 6 2025 52025112005 https://www.who.int/publications/i/item/sharps-injuries-assessing-the-burden-of-disease-from-sharps-injuries-to-health-care-workers-at-national-and-local-levels
- 8Assessment of knowledge, attitude, and practice of health-care workers towards hepatitis B virus prevention in Kabul, Afghanistan J Multidiscip Healthc Roien R Mousavi SH Ozaki A Baqeri SA Hosseini SM Ahmad S Shrestha S 317731861420213481567210.2147/JMDH.S 334438 PMC 8605488 · doi ↗ · pubmed ↗