Thyrotoxicosis: Unraveling the Mystery of Fever
Zeinab K Majed, Miril Janji, Hadil Basma, Paola Atallah

TL;DR
This paper presents a case of subacute thyroiditis causing prolonged fever and highlights the importance of considering thyroid disorders in diagnosing fevers of unknown origin.
Contribution
The paper emphasizes the need to include thyroid function tests in the routine evaluation of fever of unknown origin.
Findings
A 65-year-old male with prolonged fever was diagnosed with subacute thyroiditis after negative infectious workups.
Thyroid function tests showed suppressed TSH and elevated T4 and T3 levels, confirming thyrotoxicosis.
Corticosteroid treatment led to rapid resolution of symptoms, underscoring the importance of timely diagnosis.
Abstract
Subacute thyroiditis (SAT) is a transient inflammatory thyroid disorder, typically following an upper respiratory tract viral infection, and can rarely present as fever of unknown origin (FUO). Considering endocrine diseases in the differential diagnosis of fever is essential to prevent delayed diagnosis and unnecessary investigations. We report a case of a 65-year-old male who presented with a prolonged fever of two to three weeks, unresponsive to antibiotics, starting with mild upper respiratory symptoms. Extensive infectious and other workups were negative. Thyroid function tests revealed suppressed thyroid-stimulating hormone (TSH) and elevated free thyroxine (T4) and triiodothyronine (T3) levels. Thyroid ultrasound findings were consistent with thyroiditis. The patient was diagnosed with SAT and treated with corticosteroids, leading to rapid symptom resolution. SAT can be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
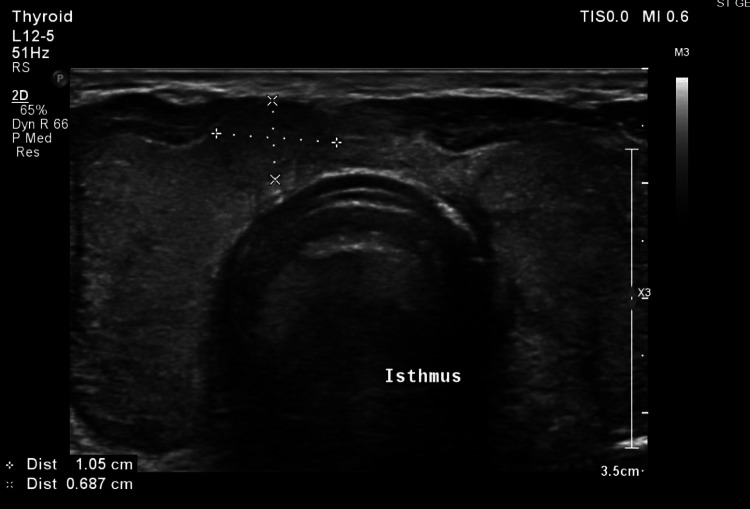 Figure 1
Figure 1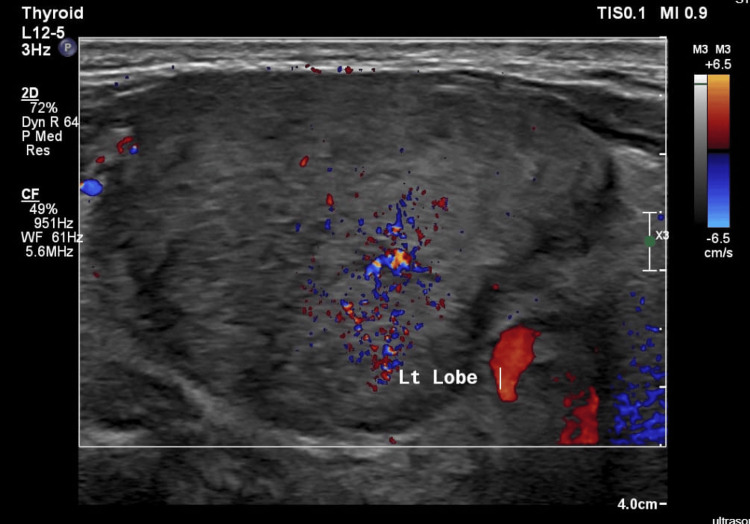 Figure 2
Figure 2 Figure 3
Figure 3| Laboratory test | Value | Units | Reference range |
| White blood cells | 11.64 | 10^9/L | 4-10 |
| Hemoglobin | 12.4 | g/dl | 13-17 |
| Hematocrit | 37 | % | 40-50 |
| Platelets | 264 | 10^9/L | 150-450 |
| Laboratory test | Reference range | October 22, 2024 | November 22, 2024 | November 24, 2024 | November 26, 2024 | November 28, 2024 | November 31, 2024 |
| Erythrocyte sedimentation rate | 0-15 mm/hour | - | 90 | 92 | - | - | - |
| C-reactive protein | <0.6 mg/dl | 17.38 | 23.78 | 17.79 | 24.89 | 23.72 | 22.91 |
| Laboratory test | November 24, 2024 | December 2, 2024 | January 17, 2025 | Units | Reference range |
| Thyroid-stimulating hormone (TSH) | 0.06 | 4.66 | 5.95 | microU/ml | 0.27-4.2 |
| Free T4 | 3.99 | 8.6 | - | ng/dl | 0.92-1.68 |
| Free T3 | 5.97 | 2.71 | - | pg/ml | 2.5-4.3 |
| TSH receptor antibodies (TRAb) | - | 0.63 | - | IU/L | <0.8 |
| Anti-thyroperoxidase (anti-TPO) | - | 1.02 | - | IU/ml | <34 |
| Anti-thyroglobulin | - | 0.61 | - | IU/ml | <116 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Hematological disorders and diagnostics · Neonatal Health and Biochemistry
Introduction
All conditions with elevated levels of thyroid hormones are called thyrotoxicosis, regardless of the underlying mechanism [1]. It amplifies catecholamine signaling, leading mainly to adrenergic symptoms (e.g., palpitations, heat intolerance, tremor, and increased bowel movements) [2]. Other manifestations can include hypermetabolism and neuromuscular symptoms (e.g., proximal muscle weakness) [3]. If left untreated, it can cause cardiac arrhythmias, congestive heart failure (CHF), osteoporosis, infertility, oligomenorrhea, uncontrolled diabetes mellitus (DM), and reduced exercise tolerance [1].
Graves’ disease is the most common cause of hyperthyroidism (70%), followed by thyroid multinodular goiter (16%). It can be caused by other uncommon conditions, such as subacute thyroiditis (SAT) (3%) and drug-induced cases (9%) [4].
Thyroiditis can be caused by painful conditions, such as SAT and suppurative thyroiditis, as well as by painless conditions, such as drug-induced thyroiditis, postpartum thyroiditis, and Riedel thyroiditis [5].
SAT generally follows a viral upper respiratory infection and causes the further release of preformed thyroid hormone due to inflammatory destruction of thyroid follicles [6,7]. It is considered the most common cause of painful thyroiditis, with females more likely to be affected, and the age at presentation ranging from three to 78 years old (average ± SD: 35.2 ± 11.2 years) [6,8]. Painless SAT is rare and can come as a fever of unknown origin (FUO) [9].
In 1961, FUO was originally defined by Petersdorf and Beeson as a body temperature above 38.3°C (101°F) on three or more occasions for at least three weeks’ duration, if undiagnosed after preliminary investigations [10]. The causes can vary. Overall, infections have been the most common (37.8%), followed by non-infectious inflammatory diseases (20.9%) such as vasculitis, granulomatous disorders, and malignancies. Other diseases (6.5%) are categorized as miscellaneous causes, which comprise SAT. The diagnosis remained irresolute in 23.2% of cases [11,12].
Endocrine disorders are a very infrequent cause of FUO [13]. Since 1961, FUO has remained a challenging diagnosis, with the most wide-ranging differential diagnosis.
Case presentation
We report a case of a 65-year-old male, a non-smoker, with a medical history of benign prostatic hyperplasia managed with tamsulosin, and dyslipidemia treated with rosuvastatin 10 mg. On November 22, 2024, he was admitted to our hospital for an unresolved fever lasting 18 days, which did not respond to a course of amoxicillin/clavulanic acid prescribed by his primary care physician for a suspected upper respiratory tract infection. The fever was accompanied by a mild headache and a five-day history of a new-onset dry cough. Additionally, he reported increased palpitations and eye dryness and redness, for which he had been using artificial tears.
He denied experiencing gastrointestinal, genitourinary, neurological, or musculoskeletal symptoms, as well as periorbital pain, jaw claudication, neck rigidity or pain, night sweats, or skin rashes. There was no history of consuming unpasteurized milk, contact with animals, recent surgical or dental procedures, new medications, or weight loss. As a result, he was hospitalized for evaluation and management of fever.
Upon admission, his vital signs were all within normal ranges except for his temperature of 39°C and heart rate of 110/min. A physical examination was unremarkable. Blood laboratory tests were significant for mild leukocytosis (Table 1) and increased inflammatory markers (Table 2).
Other laboratory tests, including kidney function, liver function, electrolytes, uric acid, antinuclear antibody (ANA), and procalcitonin, were all within normal range. An extensive workup for FUO was performed, including microbiology studies such as panculture, Cytomegalovirus (CMV) IgM, Epstein-Barr virus (EBV), purified protein derivative (PPD), Brucella antibodies, and Salmonella, all of which were negative.
Additionally, a cardiac ultrasound and a chest-abdomen-pelvis CT scan revealed no evidence of endocarditis or infections, respectively.
Due to the persistence of fever without a clear source of infection and without improvement on continuous intravenous ketoprofen, a PET scan was ordered, and as part of the evaluation for tachycardia, thyroid function tests were conducted on November 24, 2024. The results revealed low thyroid-stimulating hormone (TSH) levels and elevated free thyroxine (T4) and triiodothyronine (T3) levels (Table 3). A thyroid ultrasound done on November 28, 2024, showed an enlarged heterogeneous echotexture of the thyroid gland isthmus indicating post-thyroiditis, with minimal increase in vascularity on echo Doppler, and a 1 cm nodule in the right lobo-isthmic area classified as TIRADS (Thyroid Imaging Reporting and Data System) III, and no cervical lymph nodes (Figures 1, 2). A PET scan done on November 28, 2024, after doing the thyroid ultrasound, showed diffuse increased fluorodeoxyglucose (FDG) uptake within the enlarged thyroid gland, which could be related to thyroiditis (Figure 3).
Ultrasound showing the enlarged heterogeneous thyroid with right lobo-isthmic nodule.
Ultrasound showing the enlarged heterogeneous thyroid with minimal increased vascularity.
PET scan showing diffuse increased fluorodeoxyglucose uptake within the enlarged thyroid gland.
TRAb, anti-TPO, and anti-thyroglobulin antibodies were negative (Table 3), making the diagnosis of autoimmune thyroid diseases unlikely, so he was diagnosed with subacute thyrotoxicosis and started on propranolol 20 mg twice per day and slow tapering oral steroids (prednisolone). The patient’s fever and palpitations resolved soon after starting treatment, with follow-up thyroid function tests revealing normalization, then increased TSH, and he was clinically euthyroid (Table 3). He showed a good clinical evolution, assuring the diagnosis of SAT.
Discussion
The diagnosis of SAT is mainly clinical, where neck/jaw pain - easily dismissed as dental pain - may be a clue to SAT [11]. Symptoms vary, with palpitations and neck pain (unilateral or bilateral) being the most common presentations (62.5%), followed by weight loss (50%), goiter, anxiety, fatigue, and heat intolerance (37.5%). Diaphoresis and hoarseness occur in 25%, and only 12.5% of SAT subjects may present with tremors, fever, mood swings, insomnia, hair loss, and ear or face pain [8].
Inflammatory markers such as erythrocyte sedimentation rate (ESR) are high, and radioactive iodine (RAI) uptake is low [7,8,14]. Ultrasonography shows heterogeneous hypoechoic parenchyma and decreased vascularity [7].
It follows a triphasic pattern with a self-limiting course [6]. Around 50% of patients present in their first symptomatic phase of thyrotoxicosis, which lasts for three to six weeks, followed by painless hypothyroidism (developed in one-third of patients), which can last up to six months. Most return to euthyroidism within 12 months of onset, except for 5-15% of patients who develop permanent hypothyroidism [7].
The goal in treatment is to ameliorate the symptoms. For tachycardia, beta blockers are required. For mild symptoms, treatment is not needed. In the painful phase, patients can be treated with nonsteroidal anti-inflammatory drugs (NSAIDs; e.g., ibuprofen 1200-3200 mg per day in divided doses) or corticosteroids for severe symptoms or if NSAIDs are not effective after four days of intake (e.g., prednisone 15-40 mg per day for one to six weeks, followed by tapering of 5 mg every two weeks). If hypothyroidism occurs, levothyroxine is used if the patient is symptomatic or of reproductive age, and it is mostly transient [7].
In a systematic review of treatment protocols for SAT, steroid therapy was the most effective for moderate to severe SAT, with low initial doses (15 mg) preferred compared to higher doses (30-40 mg). The review showed that a short tapering period was associated with greater recurrence rates [15].
Stasiak et al. noted that previously painless SAT was simply undiagnosed and that cases are increasing over the years [16]. Despite changing the quantitative definition of FUO with a qualitative one requiring obligatory investigations - including a minimal diagnostic workup such as C-reactive protein, complete blood count, electrolytes, creatinine, total protein, protein electrophoresis, liver function tests, lactate dehydrogenase, rheumatoid factor, cultures, chest X-ray, abdominal ultrasound and many others - tests that should be included in the workup remain a matter of debate [11].
Given the possibility for SAT to be painless or dismissed, our case emphasizes the importance of considering SAT in the differential diagnosis of FUO and including thyroid function tests (TFTs) in routine workup to prevent the patient from being subjected to unnecessary diagnostic tests and treatments.
Conclusions
Fever is mostly due to infectious or inflammatory causes, but many endocrine disorders (thyrotoxicosis, carcinoid syndrome, pheochromocytoma, adrenal crisis) can present as fever. SAT is a rare thyroid disorder and is often overlooked, especially if it is painless. It should be considered in the differential diagnosis of FUO. A good clinical approach can aid in the early resolution of the diagnostic dilemma of fever.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis Thyroid Ross DS Burch HB Cooper DS 134314212620162752106710.1089/thy.2016.0229 · doi ↗ · pubmed ↗
- 2Thyroid-adrenergic interactions: physiological and clinical implications Thyroid Silva JE Bianco SD 157165182008 https://pubmed.ncbi.nlm.nih.gov/18279016/1827901610.1089/thy.2007.0252 · doi ↗ · pubmed ↗
- 3Neuromuscular findings in thyroid dysfunction: a prospective clinical and electrodiagnostic study J Neurol Neurosurg Psychiatry Duyff RF Van den Bosch J Laman DM van Loon BJ Linssen WH 7507556820001081169910.1136/jnnp.68.6.750PMC 1736982 · doi ↗ · pubmed ↗
- 4Hyperthyroidism: aetiology, pathogenesis, diagnosis, management, complications, and prognosis Lancet Diabetes Endocrinol Wiersinga WM Poppe KG Effraimidis G 2822981120233684891610.1016/S 2213-8587(23)00005-0 · doi ↗ · pubmed ↗
- 5Thyroiditis N Engl J Med Pearce EN Farwell AP Braverman LE 2646265534820031282664010.1056/NEJ Mra 021194 · doi ↗ · pubmed ↗
- 6Hyperthyroidism: definition, causes, pathophysiology and management Austin J Endocrinol Diabetes Bereda G 109192022 https://austinpublishinggroup.com/endocrinology-diabetes/fulltext/ajed-v 9-id 1091.pdf
- 7Thyroiditis: evaluation and treatment Am Fam Physician Martinez Quintero B Yazbeck C Sweeney LB 6096171042021 https://pubmed.ncbi.nlm.nih.gov/34913664/34913664 · pubmed ↗
- 8Subacute thyroiditis: clinical presentation and long term outcome Int J Endocrinol Alfadda AA Sallam RM Elawad GE Aldhukair H Alyahya MM 794943201420142480392910.1155/2014/794943 PMC 3996955 · doi ↗ · pubmed ↗