A Case of Curative Surgery after Effective Chemotherapy for Gastric Adenocarcinoma with Enteroblastic Differentiation Accompanied by Synchronous Multiple Liver Metastases
Shuhei Yamada, Toshiki Wakabayashi, Isao Kikuchi, Michinobu Umakoshi, Masato Sageshima, Tsutomu Sato, Junichi Arita

TL;DR
A patient with aggressive stomach cancer and liver metastases was successfully treated with chemotherapy followed by surgery, leading to long-term remission.
Contribution
This case demonstrates that aggressive surgery after effective chemotherapy can cure GAED with multiple liver metastases.
Findings
Trastuzumab-based chemotherapy effectively reduced tumor size in HER2-positive GAED with liver metastases.
Curative surgery following chemotherapy eradicated all liver metastases and achieved long-term remission.
Radical surgery may prolong survival in GAED with liver metastases if chemotherapy is effective.
Abstract
Gastric adenocarcinoma with enteroblastic differentiation (GAED) is associated with a poor prognosis because of high rates of liver and lymph node metastases. While systemic chemotherapy is the standard treatment for gastric cancer (GC) with liver metastases, several studies suggest that hepatectomy, when combined with multimodal treatment, may provide a survival benefit. However, the role of surgical resection for GAED with liver metastases remains controversial. A 71-year-old man presented with abdominal pain and nausea. Endoscopy revealed a type 2 tumor at the greater curvature of the gastric body. Contrast-enhanced computed tomography showed thickening and enhancement of the gastric wall, bulky lymph node metastases, and bilobar hepatic lesions, with the largest tumor measuring 60 mm in diameter. Histological examination of the stomach and liver tumors revealed adenocarcinoma…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
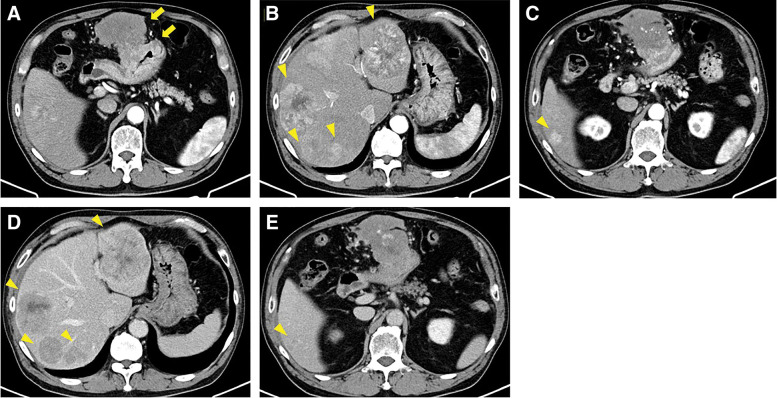 Fig. 1
Fig. 1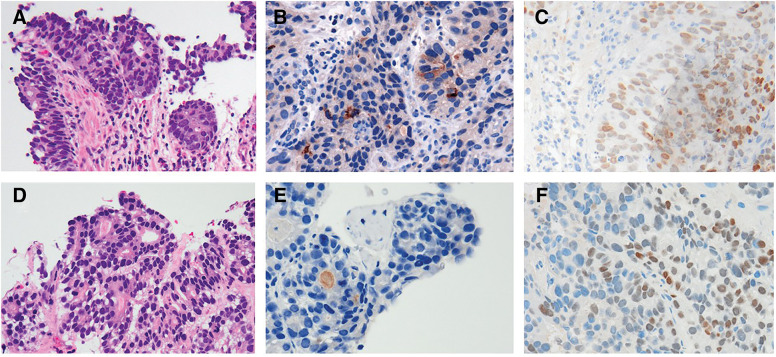 Fig. 2
Fig. 2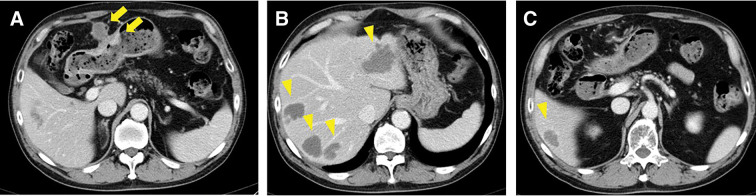 Fig. 3
Fig. 3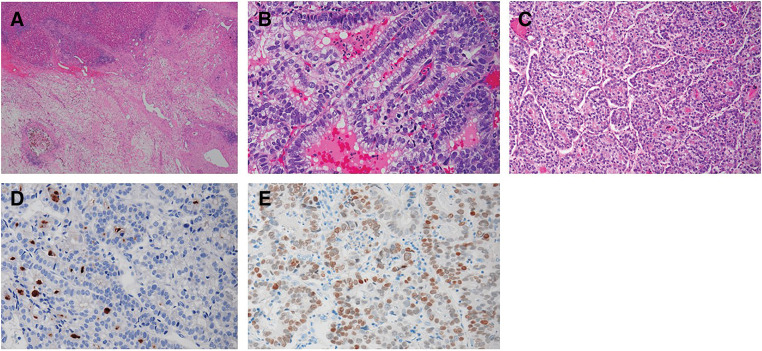 Fig. 4
Fig. 4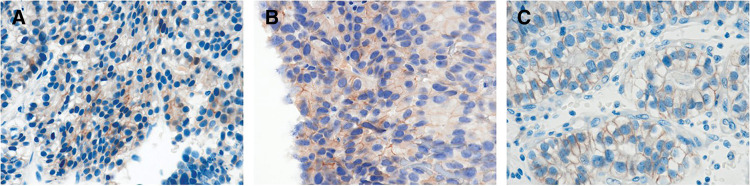 Fig. 5
Fig. 5| RBC | 4.35 106/μL | PT | 116 % |
| Hb | 13.4 g/dL | APTT | 27.2 |
| WBC | 5.5 103/μL | Glucose | 110 mg/dL |
| Plt | 21.3 104/μL | HbA1c | 5.3 % |
| T.bil | 0.54 mg/dL | ||
| D.bil | 0.12 mg/dL | HBsAg | 0 IU/mL |
| AST | 41 U/L | HBcAg | 0 IU/mL |
| ALT | 16 U/L | HCVAb | 0 C.O.I |
| ALP | 132 U/L | ||
| LDH | 543 U/L | ||
| GTP | 251 U/L | ||
| BUN | 13.8 mg/dL | ||
| CRE | 1.12 mg/dL | ||
| Na | 138 mmol/L | ||
| K | 4.6 mmol/L | ||
| CL | 106 mmol/L | ||
| TP | 6.1 g/dL | ||
| ALB | 3.7 g/dL | ||
| CRP | 0.87 mg/dL |
| Report | Histological | Sex | Age | Metastases/Invasion | Preoperative | Surgical procedure | Clinical course | Reported survival |
|---|---|---|---|---|---|---|---|---|
| Ye et al. 2013 | HAC | Male | 58 | Multiple liver metastases tumor thrombosis in the portal vein | 4 cycles of epirubicin, oxaliplatin, and fluorouracil | Distal gastrectomy with left lateral sectionectomy | No recurrence | 20 months (alive) |
| Becq et al. 2015 | HAC | Male | 69 | Infiltration into left liver and splenic hilum paraaortic lymph node metastases | 4 cycles of epirubicin, oxaliplatin, and capecitabine | Total gastrectomy with splenectomy, left hemihepatectomy, and partial phrenicotomy | No recurrence | 31 months (alive) |
| Nakao et al. 2016 | Unknown | Male | 63 | Tumor thrombosis in the portal vein | 3 cycles of S-1 and cisplatin | Total gastrectomy | No recurrence | 48 months (alive) |
| Shen et al. 2016 | HAC | Male | 70 | Infiltration into left liver | 2 cycles of capecitabine and oxaliplatin | Resection of the stomach and external lobe of left liver | No recurrence | 7 months (alive) |
| Simmet et al. 2018 | HAC | Male | 64 | Three lesions of liver metastases | 6 cycles of cisplatin and etoposide | Gastrectomy and right hemihepatectomy | No recurrence | More than 9 years (alive) |
| Jun et al. 2023 | GAED | Female | 69 | Two lesions of liver metastases | 18 cycle of nivolmab | Partial hepatectomy | No recurrence | 25 months (alive) |
| Present case | HAC + GAED | Male | 71 | Six lesions of liver metastases | 6 cycles of cisplatin, capecitabine, and trastuzumab | Distal gastrectomy with left lateral sectionectomy and partial hepatectomy | No recurrence | 28 months (alive) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Gastrointestinal Tumor Research and Treatment
Abbreviations
AFP alpha-fetoprotein AFPGC alpha-fetoprotein-producing gastric cancer GAED gastric adenocarcinoma with enteroblastic differentiation GC gastric cancer HAC hepatoid adenocarcinoma HER2 human epidermal growth factor receptor 2 PD-L1 programmed cell death ligand 1 SALL4 spalt-like protein 4
INTRODUCTION
GAED has been recognized as a variant of AFPGC. Previous studies have reported that GAED is associated with a poor prognosis because of its high incidence of liver metastases.^1,2)^ The standard treatment for GC with multiple liver metastases is chemotherapy. With chemotherapy alone, the median survival for GC with distant metastases is reportedly 10–15 months.^3–6)^ However, because of its rarity, it remains unclear whether chemotherapy for GAED is as effective as for other major histologic subtypes of GC.^7–9)^ New anticancer agents, including molecular-targeted drugs, have recently been developed. The ToGA trial demonstrated that a recombinant humanized monoclonal antibody targeting HER2 significantly prolonged overall survival in patients with HER2-positive GC.^10)^ Given that HER2 positivity tends to be higher in GAED than in conventional GC, patients with GAED may be good candidates for anti-HER2 therapy.^11–13)^ Additionally, previous studies have reported that surgical resection for GC with liver metastases can improve survival rates in select patients.^14–17)^
We herein report a case of HER2-positive GAED with synchronous multiple liver metastases, in which preoperative chemotherapy, including trastuzumab, was effective. We successfully performed surgical resection, and the patient was clinically well without any recurrence at the time of this writing.
CASE PRESENTATION
A 71-year-old man presented with abdominal pain and nausea. His medical history included systemic hypertension, angina pectoris, and gastric ulcer. Laboratory data, including liver enzyme levels, were all within the normal range (Table 1). Tumor marker levels were as follows: AFP, 552 ng/mL (normal: <10 ng/mL); protein induced by vitamin K absence-II, 23 mAU/mL (normal: <40 mAU/mL); carcinoembryonic antigen, 23 ng/mL (normal: <5.0 ng/mL); and carbohydrate antigen 19-9, 185 U/mL (normal: <37 U/mL). Contrast-enhanced computed tomography revealed thickening and enhancement of the gastric body wall, bulky lymph node swelling, and five bilobar hepatic lesions, the largest measuring 60 mm with central necrosis and heterogeneous enhancement. All liver tumors exhibited hyperattenuation in the arterial phase and washout in the venous phase. The liver surface was smooth, the liver edge was sharp, and no epigastric venous dilatation was observed (Fig. 1). Upper gastrointestinal endoscopy revealed a 50- × 40-mm type 2 tumor at the greater curvature of the gastric body.
(A) Contrast-enhanced computed tomography showing thickening and enhancement of the gastric body wall with bulky lymph node swelling (arrows). (B–E) Five bilateral hepatic lesions, with the largest measuring 60 mm, exhibiting central necrosis and heterogeneous enhancement. All liver tumors demonstrated arterial hyperattenuation and washout on dynamic computed tomography (B and C, early phase; D and E, late phase; arrowheads).
An endoscopic biopsy confirmed a histological diagnosis of poorly differentiated adenocarcinoma with HER2-positive status. Because of the hypervascularity of the liver tumors, hepatocellular carcinoma and liver metastases from GC were considered as differential diagnoses. A percutaneous needle biopsy was subsequently performed, revealing a histological diagnosis of tubular adenocarcinoma. Immunostaining of the liver specimen showed faint cytoplasmic positivity for AFP. Additionally, the tumor cells consisted of cuboidal or columnar cells resembling a primitive intestine-like structure, with periodic acid-Schiff-positive clear cells in some areas. The tumor cells also demonstrated heterogeneous positivity for SALL4 by immunostaining. Similar histopathological features were also identified in a gastric specimen. SALL4 positivity might be similar between primary and metastatic lesions but AFP of primary lesion was much more than that of metastatic lesions (Fig. 2). Based on these findings, the hepatic lesions were diagnosed as liver metastases of GAED, a variant type of AFPGC.
Histological features of the biopsied gastric and liver specimens. (A) Gastric tissue showing poorly differentiated adenocarcinoma with a tubular growth pattern and clear cells. In addition, tumor cells composed of cuboidal or columnar cells resembling a primitive intestine-like structure with clear cells (H&E, 200×). (B) Gastric tumor cells moderately stained for AFP (200×). (C) Gastric tumor cells diffusely stained for SALL4 (200×). (D) The liver biopsy specimens closely resemble the gastric specimens in morphology (H&E, 200×). (E) Liver tumor cells faintly stained for AFP (200×). (F) Liver tumor cells diffusely stained for SALL4 (200×).AFP, alpha-fetoprotein; H&E, hematoxylin and eosin; SALL4, spalt-like protein 4
We started chemotherapy with capecitabine/cisplatin plus trastuzumab. We followed the regimen used for major histologic subtypes of GC because no standardized chemotherapy protocol has been established for GAED due to its rarity.
After six cycles of chemotherapy, the liver metastases markedly decreased in size and exhibited morphological changes; the largest hepatic tumor shrank to 46 × 35 mm (59% of its original area) and became homogeneous with low attenuation, as shown in Fig. 3. No additional metastatic tumors were detected in imaging studies, and the chemotherapy response was classified as a partial response according to version 1.1 of the Response Evaluation Criteria in Solid Tumors. All tumor markers returned to normal levels, prompting the decision for curative-intent surgery as adjuvant therapy. Six weeks after chemotherapy, the patient underwent distal gastrectomy with D2 lymph node dissection, Billroth II reconstruction, left lateral sectionectomy, and two partial hepatectomies. The surgery lasted 8 hours and 21 minutes, with blood loss of 652 mL, and no blood transfusion was required. Histopathological examination revealed that nearly all liver tumors were replaced by fibrous and necrotic tissue, with no viable tumor cells remaining (Fig. 4A), and the chemotherapy efficacy for hepatic specimens was graded as Evans grade 3. By contrast, the gastric tumor, measuring 45 × 35 mm on the posterior wall, contained viable malignant cells and had infiltrated the subserosal layer without lymph node metastasis. A previously suspected metastatic lymph node showed cystic changes due to chemotherapy. Histologically, the tumor cells were tubular and poorly differentiated adenocarcinoma with clear cells, composed of cuboidal or columnar cells resembling a primitive intestine-like structure (Fig. 4B). Additionally, hepatoid areas, mimicking hepatocellular carcinoma with a nested pattern, were present in some regions (Fig. 4C). While residual tumor cells were observed in the gastric tumor, contrary to the liver tumors, both AFP and SALL4 were positive (Fig. 4D and 4E). The histological findings of the resected gastric tumor were consistent with those of the preoperatively biopsied liver tumors, leading to a final diagnosis of GAED and HAC. According to the Evans grading system, the chemotherapy efficacy for the gastric tumor was classified as grade 1b.
Tumor response after six courses of trastuzumab-containing chemotherapy. (A) Bulky lymph node swelling decreased in size, and gastric wall thickening improved (arrows). (B, C) Liver metastases shrank and demonstrated morphological changes; the largest hepatic tumor in the left lateral segment shrank to 46 × 35 mm, representing 59% of the original area (arrowheads).
Histopathological features of the resected specimens. (A) Almost all liver tumors were replaced by fibrotic scar tissue, with no viable tumor cells observed (H&E, 20×). (B) The gastric tumor displayed tubular, poorly differentiated adenocarcinoma with clear cells, composed of cuboidal or columnar cells resembling a primitive intestine-like structure (H&E, 50×). (C) The hepatoid area, resembling hepatocellular carcinoma, was arranged in a nested pattern (H&E, 100×). (D) Tumor cells stained positively for AFP (100×). (E) Tumor cells diffusely stained for SALL4 (100×).AFP, alpha-fetoprotein; H&E, hematoxylin and eosin; SALL4, spalt-like protein 4
The postoperative course was uneventful, and the patient was discharged on postoperative day 14. The same chemotherapy regimen, including trastuzumab, was continued as adjuvant therapy and completed after 1 year. At the time of this writing (>3 years after surgery), the patient remained in good health with no signs of tumor recurrence.
DISCUSSION
AFPGC is a rare subtype of GC, accounting for 1%–7% of cases,^18,19)^ with GAED recognized as a variant of AFPGC. In this case, we performed radical resection for AFPGC following chemotherapy. While the standard treatment for GC with multiple liver metastases is chemotherapy, surgical resection has been shown to improve survival rates in select patients.^14–17)^ Previous studies have identified the number and size of hepatic tumors as poor prognostic factors after hepatectomy for GC.^15,20–25)^ Kinoshita et al.^15)^ reported prognostic factors for resectable GC liver metastases, suggesting that serosal invasion of the primary tumor, the presence of ≥3 liver metastases, and a largest hepatic tumor ≥5 cm are associated with poor overall survival. They emphasized that non-surgical treatment should be considered when any of these three factors are present at diagnosis.^15)^ In this case, the patient had two of these poor prognostic factors—five liver metastases and a maximum tumor diameter exceeding 5 cm. Accordingly, we initially selected chemotherapy with an anti-HER2 drug, opting for subsequent conversion surgery only after confirming a significant reduction in liver metastases. However, the indication for conversion surgery in patients with liver metastases from GC has yet to be clearly defined.^14–17)^ Although positron emission tomography scan was not performed in the present case, a comparison of the images between before and after chemotherapy might support the validity of conversion surgery.
Previous reports have shown that AFPGC is associated with a high incidence of lymphatic and venous invasion, synchronous and metachronous liver metastases, and poor pTNM stage.^26–29)^ Adachi et al. analyzed 270 cases of AFPGC and reported that curative resection improved survival rates; however, nearly all deaths were attributed to liver metastases, with a median survival of only 15 months.^26)^ In previous studies, six cases of conversion surgery after chemotherapy for AFPGC have been reported, all leading to favorable prognoses (Table 2).^30–35)^ The histological subtype was HAC in four cases, GAED in one case, and unknown in the remaining case. Chemotherapy regimens included cisplatin or oxaliplatin in five cases, while nivolumab monotherapy was used in one case for metachronous liver metastases. In three of the six cases, curative resection was performed for liver metastases, resulting in a median survival of 25 months.^30,34,35)^ In the present case, bilobar liver metastases were observed, a condition not previously reported; however, the patient had remained alive and recurrence-free for 3 years at the time of this writing. This outcome aligns with previous reports, suggesting that long-term survival may be achievable.
The standard diagnosis of AFPGC, including GAED, is based on elevated serum AFP levels combined with specific histological findings. In GAED, solid areas consist of large cells with hyperchromatic nuclei and abundant clear cytoplasm containing intracytoplasmic periodic acid-Schiff-positive droplets, resembling a primitive intestine-like structure.^2,36)^ Additionally, the importance of immunological positivity for glypican 3 and SALL4 as enteroblastic markers has been increasingly recognized.^7,37,38)^ In the present case, SALL4 was diffusely positive. HAC, another subtype of AFPGC, is characterized by hepatoid features arranged in a tubular or solid nested growth pattern with large polygonal hepatoid-like neoplastic cells.^39,40)^ However, this area also exhibited clear hepatoid features, and both GAED and HAC are representative subtypes of GC with clear cell morphology.^7,36,41)^ Because of their rarity and histologic overlap, differentiating GAED from HAC can be challenging for pathologists. Previous reports suggest that more than half of AFPGC cases present as mixed types, incorporating HAC, GAED, and conventional adenocarcinoma.^27,42)^ In the present case, histological diagnosis was difficult because features of both GAED and HAC were observed: a primitive intestine-like structure and a nested growth pattern with large polygonal hepatoid-like neoplastic cells. However, the absence of sinusoid-like vascular channels in the solid pattern served as a distinguishing characteristic from HAC, making a diagnosis of GAED more likely than HAC.
The optimal chemotherapy regimen for GAED has not yet been established. Previous studies have reported frequent overexpression of HER2 and PD-L1 in GAED and HAC.^11,13,43–45)^ Trastuzumab, an anti-HER2 drug, has been shown to be effective in patients with advanced HER2-positive GC, as demonstrated in the large-scale phase 3 international ToGA clinical trial.^10)^ Fujimoto et al. reported HER2 positivity rates of 31% in HAC and 42% in GAED,^12)^ both higher than the 22.1% observed in conventional GC.^10)^ These findings suggest that patients with GAED and HAC may be strong candidates for anti-HER2 therapy. In the present case, chemotherapy including trastuzumab was effective, resulting in histological complete remission in the resected liver specimens. However, the primary gastric lesion remained predominantly viable. In the present case, HER2 expression of liver specimens was more clustered than that of primary lesions (Fig. 5A and 5B). In addition, HER2 expression of primary lesions before treatment was not as much as that after treatment (Fig. 5A and 5C). This discrepancy may be attributable to the reported heterogeneity in HER2 amplification rates between primary and metastatic gastric cancer lesions, which could influence differential responses to trastuzumab-based chemotherapy.^46–48)^
HER2 positivity of primary and metastatic lesions both before and after treatment. (A) Gastric tumor cells before treatment moderately stained positively for HER2 (100×). (B) Liver tumor cells before treatment strongly stained positively for HER2 (100×). (C) Gastric tumor cells after treatment moderately stained positively for HER2. HER2 expression of primary lesion before treatment was not as much as that after treatment (100×).HER2, human epidermal growth factor 2
CONCLUSIONS
We encountered a rare case of GAED with multiple liver metastases successfully treated with systemic therapy followed by curative-intent surgical resection. Although GAED is associated with a poor prognosis, preoperative anti-HER2 therapy aimed at conversion surgery may serve as a potential treatment option.
ACKNOWLEDGMENTS
We thank Angela Morben, DVM, ELS, from Edanz (https://jp.edanz.com/ac), for editing a draft of this manuscript.
DECLARATIONS
Funding
The authors declare that they have not received any funding for this report.
Authors’ contribution
SY drafted the manuscript.
TW, IK, and TS treated the patient.
MU and MS diagnosed this case based on pathological findings.
JA contributed suggestions and critiqued the manuscript.
All authors have read and approved the manuscript.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Informed consent was obtained from the patient for this publication.
Competing interests
The authors declare no conflicts of interest.
Use of artificial intelligence tools
We did not use any AI tools.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chang YC Nagasue N Kohno H Clinicopathologic features and long-term results of alpha-fetoprotein-producing gastric cancer. Am J Gastroenterol 1990; 85: 1480–5.1700600 · pubmed ↗
- 2Matsunou H Konishi F Jalal RE Alpha-fetoprotein-producing gastric carcinoma with enteroblastic differentiation. Cancer 1994; 73: 534–40.7507794 10.1002/1097-0142(19940201)73:3<534::aid-cncr 2820730307>3.0.co;2-x · doi ↗ · pubmed ↗
- 3Al-Batran SE Hartmann JT Hofheinz R Biweekly fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) for patients with metastatic adenocarcinoma of the stomach or esophagogastric junction: a phase II trial of the Arbeitsgemeinschaft Internistische Onkologie. Ann Oncol 2008; 19: 1882–7.18669868 10.1093/annonc/mdn 403 · doi ↗ · pubmed ↗
- 4Al-Batran SE Hartmann JT Probst S Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: a study of the Arbeitsgemeinschaft Internistische Onkologie. J Clin Oncol 2008; 26: 1435–42.18349393 10.1200/JCO.2007.13.9378 · doi ↗ · pubmed ↗
- 5Cunningham D Starling N Rao S Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med 2008; 358: 36–46.18172173 10.1056/NEJ Moa 073149 · doi ↗ · pubmed ↗
- 6Janjigian YY Shitara K Moehler M First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (Check Mate 649): a randomised, open-label, phase 3 trial. Lancet 2021; 398: 27–40.34102137 10.1016/S 0140-6736(21)00797-2PMC 8436782 · doi ↗ · pubmed ↗
- 7Murakami T Yao T Mitomi H Clinicopathologic and immunohistochemical characteristics of gastric adenocarcinoma with enteroblastic differentiation: a study of 29 cases. Gastric Cancer 2016; 19: 498–507.25893262 10.1007/s 10120-015-0497-9 · doi ↗ · pubmed ↗
- 8Nagtegaal ID Odze RD Klimstra D The 2019 WHO classification of tumours of the digestive system. Histopathology 2020; 76: 182–8.31433515 10.1111/his.13975 PMC 7003895 · doi ↗ · pubmed ↗