Extensive mucosal denudation and necrosis complicated by esophagothoracic fistula after submucosal tunnel endoscopic resection
Lixing Yu, Jiatao Tu, Xuan Huang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
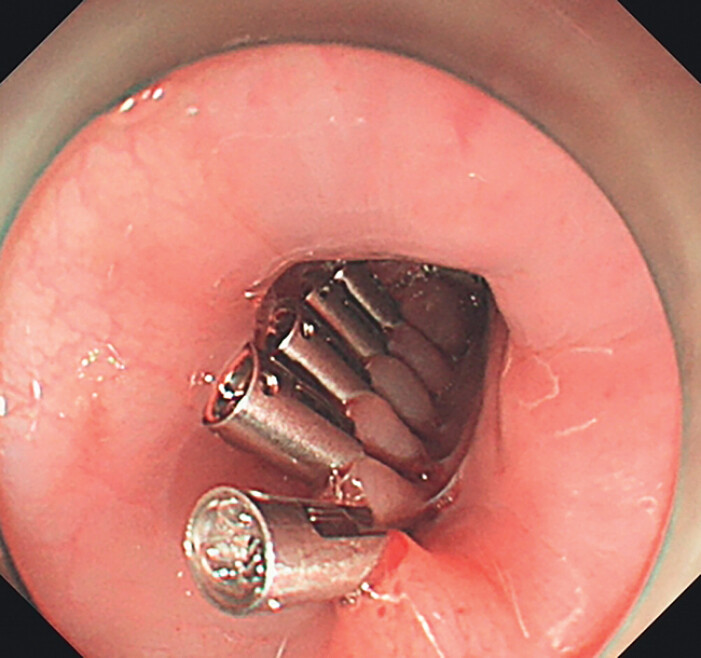 Fig. 1
Fig. 1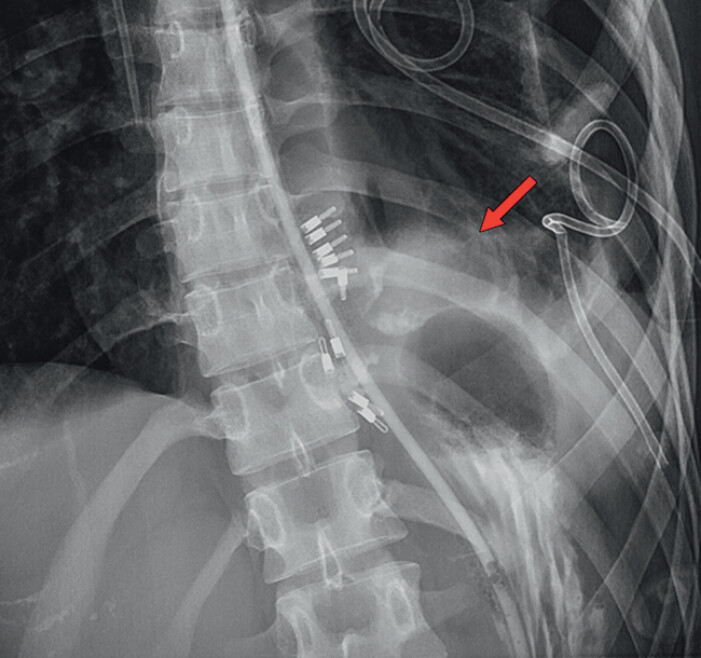 Fig. 2
Fig. 2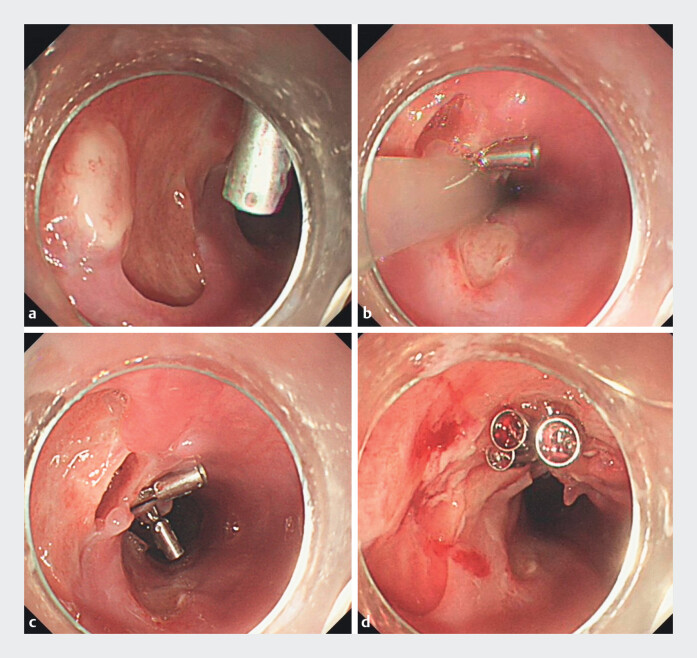 Fig. 3
Fig. 3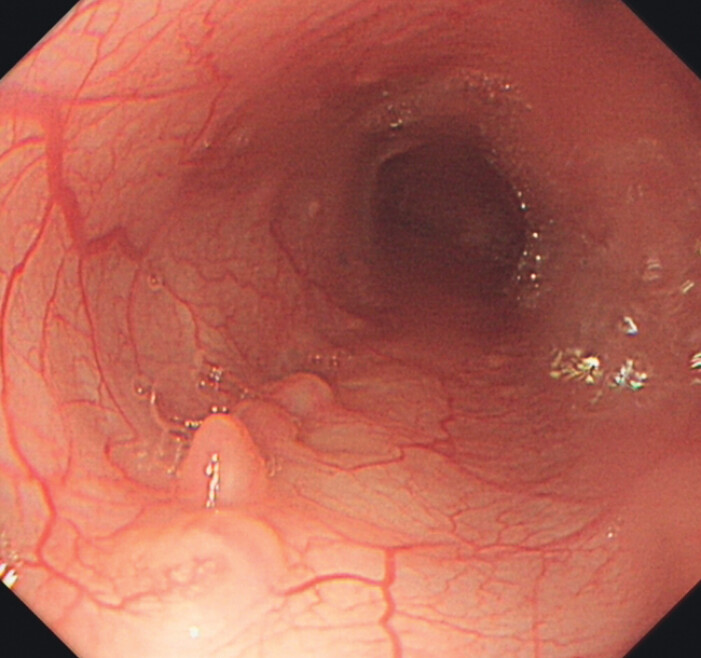 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Dysphagia Assessment and Management · Esophageal Cancer Research and Treatment
A 21-year-old woman with no underlying medical history was admitted for an esophageal mass. After excluding contraindications, submucosal tunnel endoscopic resection (STER) was performed ( Fig. 1 ).
The wound bed post-submucosal tunnel endoscopic resection was securely closed using hemostatic clips.
On postoperative day 1, the patient developed a fever, chest tightness, shortness of breath, and chest pain. Contrast esophagography demonstrated contrast extravasation, indicative of an esophagothoracic fistula ( Fig. 2 ). A left-sided tube thoracostomy was performed for closed drainage of the thoracic cavity, with two chest tubes placed in total, and a large amount of purulent fluid was drained.
Contrast esophagography demonstrated peri-procedural contrast extravasation, indicative of leakage at the surgical site.
Subsequent endoscopic evaluation revealed extensive and confluent mucosal denudation with necrosis extending from 35 to 40 cm distal to the incisors, accompanied by necrotic ulceration at the gastroesophageal junction ( Fig. 3 a–c ); the retained hemostatic clips were carefully removed under direct visualization, followed by successful closure of the suspected fistula orifice ( Fig. 3 d , Video 1 ).
a–c Endoscopy showed extensive and confluent mucosal denudation with necrosis. d Endoscopic clip closure was performed on the suspected fistula orifice.
Extensive postoperative mucosal necrosis complicated by esophagothoracic fistula successfully managed through a combination of endoscopic intervention and enhanced nutritional support therapy.Video 1
Following endoscopic intervention, antimicrobial therapy combined with enteral and parenteral nutritional support was administered, with no significant adverse events or discomfort observed during the treatment course. Contrast esophagography on postoperative day 7 confirmed the absence of contrast medium leakage into the thoracic cavity. A three-month follow-up endoscopy demonstrated satisfactory mucosal healing at the previous surgical site ( Fig. 4 ).
Endoscopic evaluation revealed satisfactory mucosal healing of the esophagus at three months postoperatively.
Extensive esophageal mucosal necrosis with esophagothoracic fistula represents a rare complication following STER 1 . Postoperative analysis suggested potential contributing factors including extensive submucosal vascular dissection during the procedure, inadequate closure of the tunnel entrance, and suboptimal postoperative nutritional support. The patient ultimately achieved complete recovery through comprehensive endoscopic management combined with adjunctive therapies. These findings indicate that extensive postoperative mucosal necrosis complicated by esophagothoracic fistula could be managed through a combination of endoscopic intervention and enhanced nutritional support therapy.
Endoscopy_UCTN_Code_CPL_1AH_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.