Isolated Central Nervous System Presentation of Early T-Cell Precursor Acute Lymphoblastic Leukemia/Lymphoma: A Rare Case of Exclusive Brain Involvement
Violet O. Swart, Behyar Zoghi

TL;DR
A rare case of a leukemia variant presented exclusively in the brain of a 73-year-old woman, highlighting the need for early detection in the central nervous system.
Contribution
Reports a rare case of isolated central nervous system presentation of ETP-ALL/LBL, expanding understanding of its clinical variability.
Findings
ETP-ALL/LBL typically involves bone marrow and blood but presented exclusively in the brain in this case.
Systemic disease was absent despite neurological symptoms, requiring surgical resection for diagnosis confirmation.
The case emphasizes the importance of CNS-directed evaluation in atypical leukemia presentations.
Abstract
Early T-cell precursor acute lymphoblastic leukemia/lymphoma (ETP-ALL/LBL) is a high-risk and biologically distinct subset of T-cell acute lymphoblastic leukemia, typically characterized by leukemic involvement of bone marrow, peripheral blood, and mediastinal structures. Central nervous system (CNS) involvement is typically a secondary manifestation [1, 2, 3]. We report a rare case of isolated CNS presentation of ETP-ALL/LBL in a 73-year-old woman who presented with progressive neurological symptoms. Imaging revealed a large right frontal extra-axial mass. Systemic evaluation, including peripheral blood flow cytometry and CT imaging of chest, abdomen, and pelvis, showed no evidence ofsystemic disease. Surgical resection and subsequent histopathology confirmed the diagnosis of ETP-ALL/LBL. A bone marrow biopsy was deffered to the patient's preference and rapid clinical deterioration.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
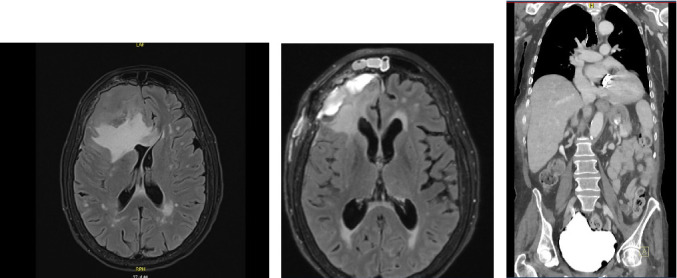 Figure 1
Figure 1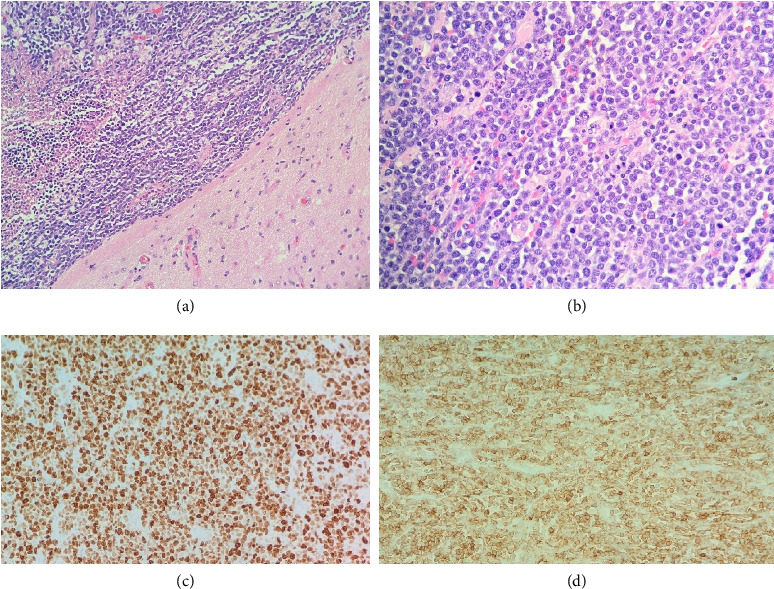 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Lymphoblastic Leukemia research · Childhood Cancer Survivors' Quality of Life · Acute Myeloid Leukemia Research
1. Introduction
Early T-cell precursor acute lymphoblastic leukemia/lymphoma (ETP-ALL/LBL), first described in 2009, accounts for 10%–15% of T-ALL cases and is characterized by an immature T-cell phenotype with stem cell and myeloid marker expression. It is associated with poor prognosis, high relapse rates, and treatment resistance. ETP-ALL/LBL typically presents with systemic findings such as leukocytosis, bone marrow infiltration, hepatosplenomegaly, and mediastinal lymphadenopathy. Central nervous system (CNS) involvement, when present, usually represents a secondary site of disease progression [4, 5, 7].
This case describes an exceedingly rare presentation of ETP-ALL/LBL confined to the CNS, in the absence of systemic disease. These atyical manifestations create significant diagnostic uncertainty and challenge conventionaltreament algorithms. They also raise important questions about disease biology, optimal therapeutic approaches, and strategies for early detection.
2. Case Presentation
A 73-year-old woman with a history of aortic valve replacement in 2008 presented with worsening headache, imbalance, weakness, and a recent fall. She denied fever, night sweat, weight loss, or other systemic symptoms. Her physical exam revealed right-sided weakness, and initial CT of the head revealed a large right frontal mass with midline shift. MRI of the brain (Figures 1(a) and 1(b)) demonstrated an 8 × 6 × 6 cm lobulated extra-axial mass in the right anterior cranial fossa, with significant surrounding edema and a 0.9 cm midline shift to the left.
Subsequent CT of the chest, abdomen, and pelvis showed no evidence of lymphadenopathy or visceral involvement (Figure 1(c)). Peripheral blood flow cytometry revealed no abnormal lymphoid population. A bone marrow biopsy was not performed, as the patient declined further invasive procedures during postoperative recovery. This decision was also influenced by the lack of systemic disease and the patient's rapid neurological deterioration aftrer surgery.
The patient underwent right frontal craniotomy with gross total resection of the tumor. Histopathology revealed diffuse infiltration of the cortical brain parenchyma by medium-to-large blastoid lymphoid cells (Figures 2(a), 2(b), 2(c), and 2(d)). Immunohistochemistry demonstrated positivity for CD3, CD4, CD7, CD34 (57%), CD43, CD45Rb, BCL-2, c-MYC, and CD117. The Ki-67 proliferation index was > 95%, consistent with a diagnosis of ETP-ALL/LBL. Flow cytometry of the brain mass confirmed these findings.
Despite initial recovery, the patient developed progressive neurological deterioration, aspiration pneumonia, and sepsis. She passed away approximately 1 month after surgery.
3. Discussion
This case illustrates an isolated CNS presentation of ETP-ALL/LBL, a rare and diagnostically challenging manifestation of an already aggressive leukemia subtype. The absence of systemic disease, normal peripheral flow cytometry, and lack of marrow involvement complicate timely diagnosis.
Three key diagnostic lessons emerge:
-
- Histopathology and immunophenotyping are essential: CNS masses of lymphoid origin require early biopsy and detailed immunophenotyping.
-
- Peripheral blood may be misleading: Negative systemic studies do not preclude the presence of hematological malignancy, particularly in cases confined to the CNS.
-
- Early CNS-directed evaluation is crucial: In patients with undifferentiated brain masses, CSF analysis, advanced imaging, and flow cytometry should be considered, especially in older patients.
The pathophysiology of CNS-restricted leukemic presentations remains poorly understood but may involve selective migration of leukemic precursors across the blood–brain barrier via adhesion molecules and chemokine interactions (e.g., CXCR4, VLA-4, and ICAM-1). Mutations in NOTCH1, FLT3, DNMT3A, and PHF6 may also play a role in CNS homing and immune evasion [6, 8, 10].
No systemic leukemia-directed therapy was administered in this case due to the delayed diagnosis and clinical deterioration. Standard ETP-ALL/LBL regimens typically involve high-dose chemotherapy and stem cell transplant, often with CNS prophylaxis. However, in isolated CNS cases, the role of CNS-penetrant agents such as intrathecal methotrexate, high-dose cytarabine, and venetoclax-based regimens remains to be defined. Emerging investigational strategies, including CAR T-cell therapy targeting CD7 and CD34, and small molecule inhibitors of JAK/STAT and FLT3 pathways, may hold promise in molecularly defined subgroups [9].
4. Conclusion
This case represents one of the very few documented instances of ETP-ALL/LBL presenting exclusively in the CNS. It highlights the importance of early diagnostic suspicion, thorough CNS-directed evaluation, and personalized therapeutic strategies. Further research is needed to define the biology of CNS-restricted leukemia and identify effective CNS-penetrant therapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rosenthal A. Younes A. High-Grade B-Cell Lymphoma With Rearrangements of MYC and BCL 2 and/or BCL 6: Double-Hit and Triple-Hit Lymphomas and Double-Expressing Lymphoma Blood Reviews 2017312374210.1016/j.blre.2016.09.0042-s 2.0-85000956373 PMC 557213727717585 · doi ↗ · pubmed ↗
- 2Jain N. Lamb A. V. O’Brien S. Early T-Cell Precursor Acute Lymphoblastic Leukemia/Lymphoma (ETP-ALL/LBL) in Adolescents and Adults: A High-Risk Subtype Blood 2016127151863186910.1182/blood-2015-08-6617022-s 2.0-8496375774226747249 PMC 4915808 · doi ↗ · pubmed ↗
- 3Coustan-Smith E. Mullighan C. G. Onciu M. Early T-Cell Precursor Leukaemia: A Subtype of Very High-Risk Acute Lymphoblastic Leukaemia The Lancet Oncology 200910214715610.1016/s 1470-2045(08)70314-02-s 2.0-5874909581619147408 PMC 2840241 · doi ↗ · pubmed ↗
- 4Patrick K. Wade R. Goulden N. Outcome for Children and Young People With Early T‐cell Precursor Acute Lymphoblastic Leukaemia Treated on a Contemporary Protocol, UKALL 2003 British Journal of Haematology 2014166342142410.1111/bjh.128822-s 2.0-8490407040424708207 · doi ↗ · pubmed ↗
- 5Inukai T. Kiyokawa N. Campana D. Clinical Significance of Early T‐Cell Precursor Acute Lymphoblastic Leukaemia: Results of the Tokyo Children’s Cancer Study Group Study L 99‐15 British Journal of Haematology 2012156335836510.1111/j.1365-2141.2011.08955.x 2-s 2.0-8485579325322128890 · doi ↗ · pubmed ↗
- 6Zhang J. Ding L. Holmfeldt L. The Genetic Basis of Early T-Cell Precursor Acute Lymphoblastic Leukaemia Nature 2012481738015716310.1038/nature 107252-s 2.0-8486290759322237106 PMC 3267575 · doi ↗ · pubmed ↗
- 7Neumann M. Heesch S. Schlee C. Whole-Exome Sequencing in Adult ETP-ALL Reveals a High Rate of DNMT 3A Mutations Blood 2013121234749475210.1182/blood-2012-11-4651382-s 2.0-8488104125023603912 · doi ↗ · pubmed ↗
- 8Bond J. Graux C. Lhermitte L. Early Response–Based Therapy Stratification Improves Survival in Adult Early Thymic Precursor Acute Lymphoblastic Leukemia: A Group for Research on Adult Acute Lymphoblastic Leukemia Study Journal of Clinical Oncology 201735232683269110.1200/jco.2016.71.85852-s 2.0-8502877476428605290 · doi ↗ · pubmed ↗