Assessment of the Impact of Anti-nuclear Antibody (ANA) Titer and Pattern on Anti-extractable Nuclear Antigen (ENA) Positivity: Experience at Cheikh Khalifa Hospital
Hamza Ouazzani, Hajar Fadili, Halima Filali, Abdelhamid Zrara, Youssef Bamou, Jalila El Bakkouri

TL;DR
This study explores how ANA titer and pattern relate to ENA positivity in patients, showing that higher ANA titers and specific patterns like S-ANA and H-ANA are linked to ENA positivity.
Contribution
The study identifies specific ANA patterns and titers that predict ENA positivity, emphasizing the importance of integrating these findings with clinical context for better diagnosis.
Findings
High ANA titers (≥1:320) and S-ANA/H-ANA patterns are strongly associated with ENA positivity.
C-ANA patterns do not predict ENA positivity, while N-ANA has limited predictive value.
Nine percent of ANA-negative patients were ENA-positive, highlighting discrepancies between detection methods.
Abstract
This retrospective study examined the relationship between anti-nuclear antibody (ANA) titers, immunofluorescence (IIF) patterns, demographic variables, and anti-extractable nuclear antigen (ENA) positivity in a cohort of 538 patients at Cheikh Khalifa Hospital. Among them, 409 of 538 patients (76%) were women, and 129 of 538 (24%) were men. ANA and 15 ENA specificities were assessed using indirect IIF on Hep-2/monkey liver substrates and immunoblot analysis with the ANA Profile 3 Plus DFS-70 kit (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany). ANA staining patterns were classified based on ICAP guidelines as speckled (S-ANA), homogeneous (H-ANA), cytoplasmic (C-ANA), and nucleolar (N-ANA). Certain patterns are known to be associated with specific antibodies or clinical conditions; for example, S-ANA may suggest anti-Sm antibodies in systemic lupus erythematosus, while…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
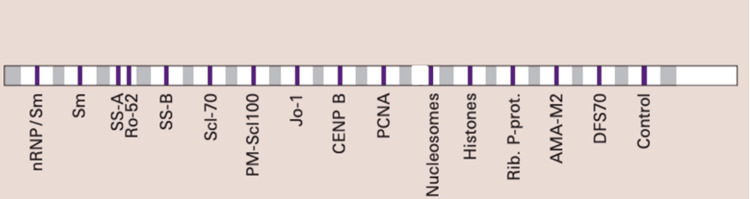 Figure 1
Figure 1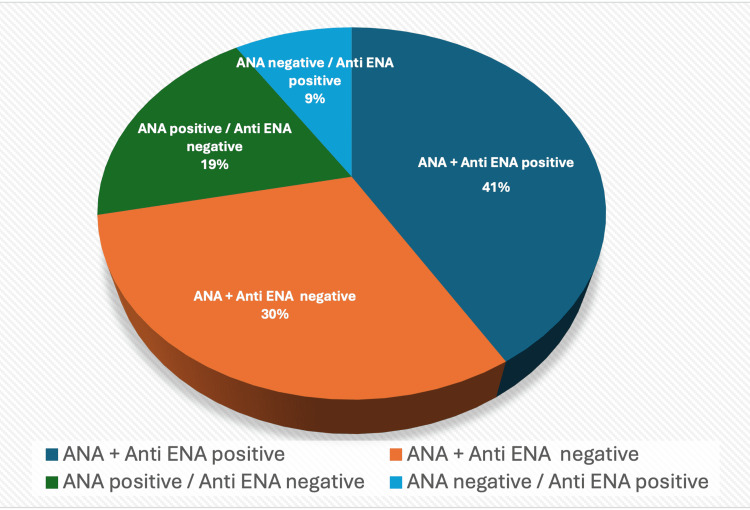 Figure 2
Figure 2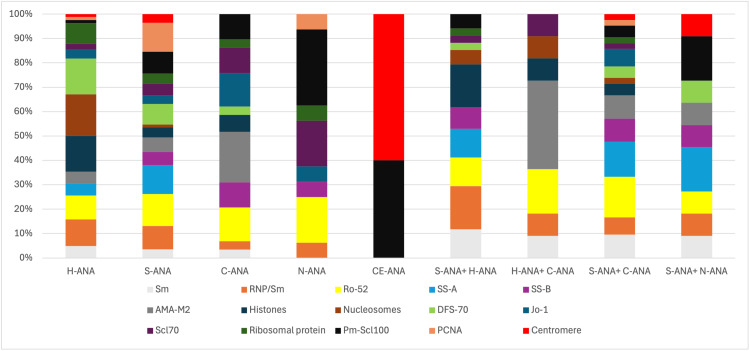 Figure 3
Figure 3| Variables | Values |
| Average age | 47.7 |
| 0-20 | 38 (7%) |
| 20-40 | 161 (30%) |
| 41-60 | 187 (35%) |
| >60 | 152 (28%) |
| Females | 409 (76%) |
| Males | 129 (24%) |
| Frequency | |
| ANA positive | 326 (61%)/538 |
| ANA patterns | |
| H-ANA | 49 (15%)/326 |
| S-ANA | 161 (49%)/326 |
| C-ANA | 39 (12%) / 326 |
| N-ANA | 17 (5%)/ 326 |
| CE-ANA | 5 (1%)/ 326 |
| H-ANA + S-ANA | 8 (2%)/326 |
| S-ANA + C-ANA | 26 (8%)/326 |
| H-ANA + C-ANA | 6 (2%)/326 |
| S-ANA + N-ANA | 7 (2%)/326 |
| H-ANA + N-ANA | 4 (1%)/326 |
| N-ANA + C-ANA | 4 (1%)/326 |
| ANA titers | |
| 1/160 | 174 (53%)/326 |
| 1/320 | 93 (29%) /326 |
| 1/640 | 46 (14%)/326 |
| 1/1280 | 13 (4%)326 |
| Antigenic targets | Frequency |
| Anti-ENA | 268 (49%)/538 |
| Sm | 22/268 |
| RNP/Sm | 41/268 |
| SS-A | 40/268 |
| SS-B | 23/268 |
| Ro-52 | 61/268 |
| Jo-1 | 22/268 |
| Scl70 | 23/268 |
| Nucleosomes | 21/268 |
| Centromere | 16/268 |
| Pm-Scl100 | 43/268 |
| PCNA | 31/268 |
| Histones | 31/268 |
| AMA-M2 | 33/268 |
| Ribosomal protein | 14/268 |
| DFS-70 | 35/268 |
| Patterns | ||||||||||||
| ENA | H-ANA (N=49) | S-ANA (N=161) | C-ANA (N=39) | N-ANA (N=17) | ||||||||
| n/N | p-value | OR | n/N | p-value | OR | n/N | p-Value | OR | n/N | p-value | OR | |
| Sm | 4 /49 | 0.234 | 2.42 (0.779-7.49) | 6/161 | 1 | 0.908 (0.246-2.39) | 1/39 | 0.97 | 0.617 (0.0806-4.72) | 0/17 | 0.824 | 0.652 (0.037-11.2) |
| Sm/RNP | 9/49 | 0.009 | 3.14 (1.4-7.05) | 16/161 | 0.290 | 1.51 (0.783-2.91) | 1/39 | 0.342 | 0.295 (0.0395-2.21) | 1/17 | 1 | 0.736 (0.095-5.69) |
| SS-A | 4/49 | 1 | 1.16 (0.395-3.43) | 20/161 | 0.004 | 2.75 (1.41-5.35) | 0/39 | 0.137 | 0.148 (0.089-2.46) | 0/17 | 0.476 | 0.351 (0.0207-5.96) |
| Ro-52 | 8/49 | 0.310 | 1.67 (0.743-3.77) | 22/161 | 0.249 | 1.46 (0.826-2.56) | 4/39 | 1 | 0.921 (0.31-2.69) | 3/17 | 0.618 | 1.76 (0.495-6.38) |
| SS-B | 0/49 | 0.247 | 0.205(0.0123-3.44) | 9/161 | 0.397 | 1.61 (0.675-3.85) | 3/39 | 0.466 | 2.06 (0.582-7.3) | 1/17 | 1 | 1.46 (0.185-11.5) |
| AMA-M2 | 4/49 | 0.643 | 1.55 (0.517-4.64) | 10/161 | 0.88 | 1.15 (0.525-2.51) | 6/39 | 0.10 | 2.73 (0.98-7.58) | 0/17 | 0.62 | 0.451 (0.0265-7.68) |
| Histones | 12/49 | <0.001 | 7.85 (3.54-17.4) | 8/161 | 0.702 | 0.782 (0.34-1.79) | 2/39 | 1 | 0.85 (0.197-3.73) | 0/17 | 0.601 | 0.436 (0.0256-7.42) |
| Nucleosomes | 14/49 | <0.001 | 31.5 (11.4-87.1) | 2/161 | 0.07 | 0.244 (0.055-1.06) | 0/39 | 0.394 | 0.290 (0.0172-4.88) | 0/17 | 0.853 | 0.685 (0.039-11.8) |
| DFS-70 | 12/49 | <0.001 | 6.43 (2.96-13.9) | 14/161 | 0.283 | 1.57 (0.777-3.17) | 1/39 | 0.468 | 0.352 (0.0469-2.64) | 0/17 | 0.534 | 0.384(0.0226-6.51) |
| Jo-1 | 3/49 | 0.67 | 1.67(0.474-5.8) | 6/161 | 1 | 0.9 (0.34-2.39) | 4/39 | 0.09 | 3.17 (1.01-9.94) | 1/17 | 1 | 1.53 (0.194-12.1) |
| Scl70 | 2/49 | 1 | 0.928 (0.211-4.08) | 8/161 | 0.82 | 1.23 (0.510-2.95) | 3/39 | 0.514 | 1.95 (0.554-6.89) | 3/17 | 0.034 | 5.26 (1.40-19.8) |
| Ribosomal protein | 7/49 | <0.001 | 11.2 (3.76-33.6) | 7/161 | 0.651 | 0.614 (0.169-2.23) | 1/39 | 1 | 0.964 (0.123-7.56) | 1/17 | 0.94 | 2.39 (0.295-19.4) |
| Pm-Scl100 | 1/49 | 0.196 | 0.229 (0.0307-1.70) | 15/161 | 0.48 | 1.35 (0.693-2.62) | 3/39 | 1 | 0.989(0.291-3.36) | 5/17 | 0.003 | 5.50 (1.84-16.5) |
| PCNA | 1/49 | 0.433 | 0.336 (0.0447-2.52) | 20/161 | <0.001 | 4.78 (2.17-10.5) | 0/39 | 0.23 | 0.198(0.0118-3.30) | 0/17 | 0.1 | 1.08 (0.138-8.42) |
| Centromere B | 1/49 | 1 | 0.692 (0.089-5.38) | 6/161 | 0.698 | 1.54 (0.539-4.40) | 0/39 | 0.543 | 0.388 (0.0228-6.60) | 0/17 | 1 | 0.91 (0.052-15.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Monoclonal and Polyclonal Antibodies Research · Chronic Lymphocytic Leukemia Research
Introduction
Anti-nuclear antibodies (ANA) are autoantibodies directed against various cellular components, including nuclear, mitotic, and cytoplasmic elements. Their detection is generally indicated in patients with signs suggestive of connective tissue disease or systemic autoimmune disease. ANA profiles are strongly associated with autoimmune conditions, such as systemic lupus and scleroderma, frequently serving as early warning signs. However, positive ANA results aren't unique to autoimmunity; we regularly detect low-titer ANA in healthy controls and patients battling infections or unrelated conditions. Typically, higher ANA titers are associated with a greater likelihood of true autoimmune pathology, whereas very low ANA titers (1:40 or 1:80) are often nonspecific. Previous surveys have shown that only a small percentage of healthy people (around 5%) have ANA titers as high as 1:160 [1,2].
They are most commonly detected by indirect immunofluorescence (IIF) on Hep-2 cells, a human cell line derived from a squamous cell carcinoma of the larynx, which is chosen due to its large nuclei and high mitotic rate, allowing for the screening of a wide range of autoantibodies. However, it does not precisely identify specific antigenic targets [3].
Therefore, following a positive ANA-IIF result, anti-extractable nuclear antigen (ENA) antibodies are often detected using solid-phase techniques such as ELISA, immunodot, or the Luminex method, allowing for a more precise identification of targeted antigens. Some patterns of ANA staining are associated with certain ENA antibodies or diseases; for instance, a speckled pattern might suggest anti-Sm in lupus, or C-ANA patterns are often associated with antibodies targeting cytoplasmic antigens, such as anti-mitochondrial or anti-Jo-1 antibodies, which are relevant in primary biliary cholangitis or antisynthetase syndrome, respectively. Whether the ANA titer level or IIF pattern can predict subsequent ENA positivity is an important question for optimizing diagnostic algorithms [4].
This study aimed to assess the association between patient demographics (age, sex), ANA titers, and IIF patterns with ENA antibody detection by immunoblot to evaluate their predictive value and support more targeted ENA testing. This study was conducted at Cheikh Khalifa Hospital, a tertiary care center in Morocco that serves a diverse patient population, providing a relevant and representative setting for evaluating ANA and ENA profiles in real-world clinical practice.
Materials and methods
Study design
We performed a retrospective, observational study in the immunology laboratory of Cheikh Khalifa Hospital, reviewing all ANA and ENA tests conducted from January 1, 2023, to January 31, 2024.
Study population and sample size
During the study period, we included 538 consecutive patients referred for ANA and ENA testing. Exclusion criteria comprised hemolyzed or insufficient serum samples, as well as patients with a confirmed diagnosis of autoimmune disease who were already receiving immunosuppressive or immunomodulatory therapy. The latter exclusion aimed to minimize the confounding effects of treatments on autoantibody titers and profiles. The final cohort consisted of 538 patients, including 409 females (76.0%) and 129 males (24.0%), with a mean age of 47.7 years (range: 0-90 years). The age distribution was stratified as follows: 38 patients (7%) were aged 0-20 years, 161 (30%) were aged 20-40 years, 187 (35%) were aged 41-60 years, and 152 (28%) were over 60 years.
Laboratory procedures
ANA screening was performed at an initial dilution of 1:160 using Hep-2/monkey liver slides and FITC-conjugated anti-IgG (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany). Fluorescence patterns were recorded and classified following the International Consensus on ANA Patterns (ICAP) guidelines, including homogeneous (H-ANA), speckled (S-ANA), cytoplasmic (C-ANA), nucleolar (N-ANA), centromeric (CE-ANA), and mixed, as well as end-point titers (1:160, 1:320, 1:640, ≥1:1 280) [5].
We considered a titer of 1:160 as the screening cutoff for positivity. Additionally, for analysis, we defined high-titer ANA as ≥1:1280, moderate titer as 1:320 or 1:640, and low titer as 1:160. All ANA IIF slides were interpreted by qualified specialists in clinical biology, with positive and negative controls included in each run to ensure result reliability.
Anti-ENA profiling (Sm, RNP/Sm, SSA/Ro52, SSB, Jo-1, Scl-70, nucleosomes, centromeres, Pm-Scl-100, PCNA, histones, AMA-M2, ribosomal P proteins, DFS-70) was carried out using the ANA Profile 3 Plus DFS-70 kit (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany; Figure 1) and quantified with EUROLineScan (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany; negative: 0-5; borderline: 6-10; positive: 11-50; strongly positive: >50). The manufacturer's protocols were strictly followed throughout the testing process.
EUROIMMUN immunoblot (ANA Profile 3 Plus DFS-70)ANA: anti-nuclear antibody
Statistical analysis
Statistical analyses were conducted using Jamovi software version 2.3 (Jamovi, Sydney, Australia) and XLSTAT software version 2023 (Addinsoft, Paris, France). Categorical variables were expressed as frequencies and percentages. Associations between ANA characteristics (pattern and titer) and ENA positivity were assessed using univariate analysis via chi-square (χ²) tests. For binary variables coded as 0 (negative) and 1 (positive), odds ratios (ORs) and 95% confidence intervals (CIs) were calculated based on contingency tables to quantify the strength and direction of the associations. All tests were two-tailed, and statistical significance was set at p<0.05.
Results
Among the 538 patients, 409 (76%) were women and 129 (24%) were men, with a mean age of 47.7 years. Out of the total number of patients, 326 (60%) tested positive for ANA, including 260 women (48%) and 66 men (12%). ENA antibodies were detected in 268 patients (n=268; 50% of the total cohort): 215 (40%) women and 53 (10%) men. The 40-60 year age group accounted for the most significant proportion of patients in the cohort, with 187 out of 538 individuals (35%). Tables 1-3 summarize the demographic and serological characteristics of the studied population.
A total of 221/538 (41%) patients had positive ANA and ENA results, while 165/538 (30%) were negative for both tests. Additionally, 105/538 (19%) ANA-positive sera tested negative for ENA, whereas 47/538 (9%) ANA-negative sera tested positive for ENA (Figure 2). The most frequently identified IIF patterns among positive patients, both women and men, were 161/326 (49%) S-ANA and 49/326 (15%) H-ANA. Some patients exhibited mixed patterns, most commonly S-ANA + C-ANA in 26/326 patients (8%). We analyzed the most common ENA among different ANA patterns. ENA could be detected at varying frequencies depending on the ANA patterns.
Distribution of patients according to ANA and ENA resultsANA: anti-nuclear antibody, ENA: extractable nuclear antigen
The most frequently identified ENAs were Ro-52, SS-A, PmScl-100, and Sm/RNP. SS-A/Ro52 (20/268 and 22/268) and PCNA (20/268) were predominant in patients with S-ANA. Nucleosomes (14/268), histones (12/268), and DFS-70 (12/268) were the most frequently found in H-ANA. The AMA-M2 antigen was most frequently seen with cytoplasmic fluorescence (6/268), while Pm-Scl100 (5/268), Scl-70 (3/268), and Ro-52 (3/268) were linked to nucleolar fluorescence. Regarding mixed patterns, the most frequent combination, S-ANA + C-ANA, mainly presented Ro-52 (7/268) and SS-A (6/268) (Figure 3).
Frequency of ENA in different ANA profilesENA: extractable nuclear antigen, ANA: anti-nuclear antibody, H-ANA: homogeneous, S-ANA: speckled, C-ANA: cytoplasmic, N-ANA: nucleolar, CE-ANA: centromeric
Association between ANA patterns and anti-ENA antibodies
We found specific associations between ANA patterns and anti-ENA antibodies. There was an increased frequency of SSA (20/161; p=0.004, OR: 2.75, 95% CI: 1.41-5.35) and PCNA (20/161; p<0.001, OR: 4.78, 95% CI: 2.17-10.5) in patients with speckled patterns. There was an increased frequency of anti-histone antibodies (12/49; p<0.001, OR: 7.85, 95% CI: 3.54-17.4), anti-nucleosome antibodies (14/49; p<0.001, OR: 31.5, 95% CI: 11.4-87.1), anti-DFS 70 antibodies (12/49; p<0.001, OR: 6.43, 95% CI: 2.96-13.9), anti-ribosomal protein antibodies (7/49; p<0.001, OR: 11.2, 95% CI: 3.76-33.6), and anti-Sm/RNP antibodies (9/49; p=0.009, OR: 3.14, 95% CI: 1.4-7.05) in patients with homogeneous fluorescence. We found an increased frequency of anti-Scl70 antibodies (3/17; p=0.034, OR: 5.26, 95% CI: 1.40-19.8) and anti-Pm-scl100 antibodies (5/17; p=0.003, OR: 5.50, 95% CI: 1.84-16.5) in sera with nucleolar fluorescence. The results can be found in Table 4.
Association between gender and anti-ENA antibodies
Our analysis revealed significant gender-based differences in anti-ENA antibody profiles. Anti-ENA positivity was substantially higher in women (215 out of 409 women, 53%) than in men (53 out of 129 men, 41%), with this difference reaching statistical significance (p=0.023). Women demonstrated a greater likelihood of anti-ENA positivity (OR: 1.59, 95% CI: 1.06-2.37). The disparity was particularly striking for anti-SSA antibodies: detected in 9% of women (37 out of 409 women) versus only 2% of men (3 out of 129 men). This gender-specific pattern remained statistically significant (p=0.01), with women showing higher odds of anti-SSA positivity (OR: 4.18, 95% CI: 1.27-13.8).
Association between age and anti-ENA antibodies
Anti-ENA antibodies were most frequently detected in the 40-60 age group, where 106 of 187 individuals (57%) tested positive. This association was statistically significant (p=0.02; OR: 1.53, 95% CI: 1.07-2.18).
Association between ANA titer and anti-ENA antibodies
The frequency of anti-ENA antibodies was higher in patients with a moderate (OR: 3.37, 2.22-5.11) and high ANA titer (p<0.001, OR: 28.6, 1.69-483) compared to those with a low titer (p<0.001, OR: 2.16, 95%, 1.49-3.13). Sixty-five of 174 patients (37%) with a low titer did not present anti-ENA antibodies, compared to 40 of 139 (28%) with moderate fluorescence intensity and none of the 13 patients with high fluorescence intensity.
Discussion
The primary objective of this study was to investigate whether specific ANA patterns and titers, as detected by IIF on HEp-2 cells, are associated with the presence of anti-ENA antibodies in a Moroccan hospital-based population. Detecting ANA is crucial when evaluating systemic autoimmune diseases, particularly when patients exhibit symptoms in multiple organs. But a positive ANA result from standard IIF testing doesn't automatically equal autoimmune disease. These antibodies are also commonly found in non-rheumatic cases [6].
ANA-IIF patterns as predictors of anti-ENA antibody profiles
In this cohort, S-ANA was the most frequently observed ANA profile, noted in 161 of the 326 ANA-positive cases (49%). H-ANA and C-ANA followed in frequency. A notable association was found between S-ANA and anti-SSA antibodies, identified in 20 of the 161 patients (p=0.004; OR: 2.75; 95% CI: 1.41-5.35). This association echoes earlier findings from studies like those of Sanchez-Guerrero et al. (40%) [7], Banhuk et al. (43%) [8], and Lora et al. [9], which all demonstrated a similar connection between S-ANA and the presence of anti-SSA or anti-Ro52 antibodies.
This alignment highlights the clinical significance of S-ANA as a reliable indicator of anti-ENA antibody presence, particularly in cases involving SSA/Ro autoantibodies. It highlights the potential utility of this pattern in directing ENA testing for patients being evaluated for systemic autoimmune conditions.
The association between H-ANA and anti-histone or anti-nucleosome antibodies in our study is consistent with previous findings [10]. Notably, we also observed H-ANA in several patients who were positive for DFS-70, although this antibody typically produces a dense, fine-speckled (DFS) pattern on IIF. Similar discrepancies were reported by Yumuk and Demir [11], who found that nearly half of DFS-70-positive individuals displayed atypical staining patterns. This variability may reflect the coexistence of other autoantibodies, as 10 of 35 DFS-70-positive cases in our study also had anti-histone or anti-nucleosome antibodies. The potential involvement of anti-DNA antibodies, not assessed here, cannot be excluded [12].
H-ANA's association with anti-ribosomal protein antibodies does not align with standard ANA profiles, such as AC-19 (diffuse cytoplasmic fluorescence) or AC-5 (coarse speckled nucleoplasmic fluorescence) for Sm/RNP [13]. Some studies suggest that IIF is not a reliable screening test for anti-RibP antibodies, with detection sensitivity below 30% in certain Hep-2 cell studies [14]. Since anti-Sm/RNP and anti-ribosomal protein antibodies are particular to lupus, their presence might indicate SLE cases with anti-DNA, histone, or nucleosome antibodies contributing to homogeneous fluorescence [15]. In some studies, 28.6% of lupus patients showed an RNP/Sm association with homogeneous fluorescence [16]. In our study, all patients (9/9) with homogeneous fluorescence and positive RNP/Sm ENA were also positive for histones/nucleosomes.
Moreover, N-ANA, although rare, was observed in 17 out of 326 ANA-positive patients (5%) and showed a strong association with anti-Scl70 and anti-Pm-Scl100 antibodies. These findings reinforce the diagnostic value of N-ANA in systemic sclerosis and overlap syndromes, where anti-Scl70 and anti-Pm-Scl100 serve as serological markers for diffuse cutaneous systemic sclerosis and scleroderma-polymyositis overlap, respectively [13].
However, it is important to note that ANA positivity is not exclusive to autoimmune diseases; it may also occur in viral infections, drug-induced autoimmune reactions, or in healthy elderly individuals, especially at low titers [2].
High ANA titers strongly correlate with ENA positivity
ANA titers of 1:320 or higher (1:640, ≥1:1280) are generally observed in patients with autoimmune diseases. In contrast, low-titer ANA (such as 1:160) may be seen in both autoimmune conditions and occasionally in healthy individuals. Our findings align with studies showing that samples with high fluorescence intensity at a fixed titer have an increased frequency of anti-ENA antibodies [17].
Gender-specific differences in anti-ENA antibody prevalence
Among the 40 SSA-positive sera, 37 were from women and only three from men. A strong association was found between anti-SSA and female sex (OR: 4.18), consistent with previous studies, especially in Sjögren's syndrome, where anti-SSA/Ro is predominant in women, reaching 94% in some studies [6]. Estrogen and other sex hormones may contribute to a higher prevalence of autoimmunity and increased ANA positivity in women, with levels rising with age [18,19]. However, the high proportion of women in our study, 409 out of 538 patients (76%), may have influenced these findings.
The study has several strengths. First, a large number of patients (n=538) were included in the study, which contributes to making the statistical analysis more robust and provides insight into ANA/ENA testing in the Moroccan population. Second, we analyzed several parameters, including age, sex, ANA titer, and IIF patterns, highlighting their associations with anti-ENA. In addition, using a 15-antigen immunoblot panel for ENA testing, more than several studies on the same subject enabled us to conduct a more precise analysis of the effect of different variables on ENA positivity. Finally, our observations were reinforced by the fact that patients with autoimmune diseases were excluded from the study, which allowed us to reduce the potential confounding effect of immunosuppressive treatments on anti-nuclear antibody levels.
Three methodological constraints deserve attention. The retrospective, single-center design may introduce referral bias and limit the ability to draw causal conclusions. Lack of comprehensive clinical data (particularly symptoms and diagnoses) also restricts serological interpretation. Future studies require covariate adjustment to establish the true predictive utility of ANA across populations. Multivariate analysis would clarify the interactions between key variables, such as titer levels and fluorescence patterns. Although EUROIMMUN kits demonstrated consistent performance, unverified cases obtained through methods such as ELISA can affect the reliability of certain findings. Crucially, since all participants were referred explicitly for ANA testing, our results may not extend to general screening contexts.
Additionally, the observed discordance between ANA-negative and ENA-positive results in 47 of 538 patients (9% of cases) may reflect differences in assay sensitivity or antigen coverage between IIF and immunoblot techniques [20]. Finally, the presence of ENA negativity in 105 out of 538 ANA-positive patients (19%) highlights the limited specificity of IIF, as ANA positivity may also be observed in non-autoimmune conditions or even in healthy individuals [17].
Conclusions
Our data clearly show that high ANA titers and specific patterns, particularly S-ANA and H-ANA, reliably indicate the presence of anti-ENA antibodies, confirming their diagnostic value in autoimmune workups. C-ANA, in contrast, proved less clinically useful. The increased ENA positivity we noted in women and those aged 40-60 years likely reflects referral patterns in our cohort rather than true biological trends. These observations highlight a critical need: refining how labs interpret ANA profiles to target ENA testing smartly. While lab results provide key pieces of the puzzle, they're just one part. We always combine ANA findings with the patient's comprehensive clinical picture, including symptoms, examination findings, and suspected diagnoses, to reach accurate conclusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The use of antinuclear antibodies in clinical practice Réanimation Lassoued K Coppo P Gouilleux-Gruart V 651656142005
- 2Range of antinuclear antibodies in "healthy" individuals Arthritis Rheum Tan EM Feltkamp TE Smolen JS 16011611401997932401410.1002/art.1780400909 · doi ↗ · pubmed ↗
- 3Added value of indirect immunofluorescence intensity of automated antinuclear antibody testing in a secondary hospital setting Clin Chem Lab Med Oyaert M Bossuyt X Ravelingien I Van Hoovels L 63665420162656203710.1515/cclm-2015-0887 · doi ↗ · pubmed ↗
- 4Assessment of antinuclear antibodies (ANA): national recommendations on behalf of the Croatian society of medical biochemistry and laboratory medicine Biochem Med (Zagreb) Tešija Kuna A Đerek L Drvar V Kozmar A Gugo K 2050231202110.11613/BM.2021.020502 PMC 804779133927550 · doi ↗ · pubmed ↗
- 5Reflecting on a decade of the international consensus on ANA patterns (ICAP): accomplishments and challenges from the perspective of the 7th ICAP workshop Autoimmun Rev Andrade LE Klotz W Herold M 1036082320243918722110.1016/j.autrev.2024.103608 · doi ↗ · pubmed ↗
- 6Risk factors for ANA positivity in healthy persons Arthritis Res Ther Li QZ Karp DR Quan J 3813201110.1186/ar 3271 PMC 313201721366908 · doi ↗ · pubmed ↗
- 7Utility of anti-Sm, anti-RNP, anti-Ro/SS-A, and anti-La/SS-B (extractable nuclear antigens) detected by enzyme-linked immunosorbent assay for the diagnosis of systemic lupus erythematosus Arthritis Rheum Sánchez-Guerrero J Lew RA Fossel AH Schur PH 10551061391996865197110.1002/art.1780390626 · doi ↗ · pubmed ↗
- 8Relationships among antibodies against extractable nuclear antigens, antinuclear antibodies, and autoimmune diseases in a Brazilian public hospital Autoimmune Dis Banhuk FW Pahim BC Jorge AS Menolli RA 9856910201820183036402110.1155/2018/9856910 PMC 6186355 · doi ↗ · pubmed ↗