Effectiveness of implementation strategies for uptake of fall prevention interventions in community care: A systematic review
Siv Linnerud, Linda Aimée Hartford Kvæl, Birgitte Graverholt, Maria Bjerk, Kristin Taraldsen, Therese Brovold, Rehana Abdus Salam, Rehana Abdus Salam, Rehana Abdus Salam, Rehana Abdus Salam

TL;DR
This paper reviews how well strategies to implement fall prevention programs work in community care for older adults.
Contribution
The study highlights the limited evidence on effective implementation strategies for fall prevention in community settings.
Findings
Training and education strategies can increase the number of fall prevention interventions in communities.
There is no clear evidence that these strategies reduce hospital or emergency department admissions.
The review identifies a significant research gap in evaluating implementation strategies for fall prevention.
Abstract
Falls among older adults are one of the leading causes of morbidity and mortality in this population and pose a significant economic burden on society. Despite substantial evidence supporting effective interventions to prevent falls, their uptake in practice remains limited. While various strategies could enhance implementation, few have been evaluated for their effectiveness in fall prevention. This study aimed to assess the effectiveness of such implementation strategies on implementation and health-related outcomes in community care for fall prevention. A systematic search was conducted in MEDLINE (Ovid), CINAHL, EMBASE, PsycINFO, Web of Science, the Cochrane Library, and Google Scholar November 27th 2024. We included studies evaluating an implementation strategy for preventing falls among older adults living in the community. Eligible study designs included randomized controlled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
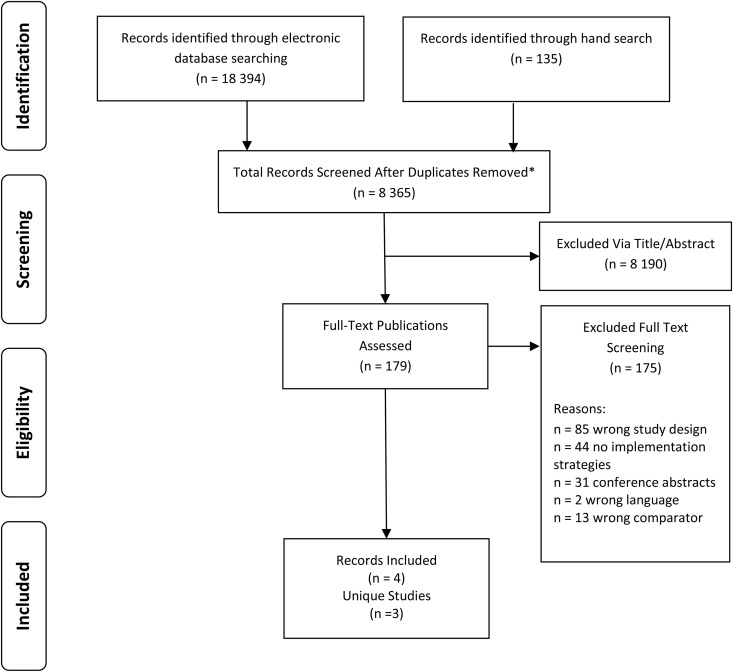 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100005416Norges Forskningsråd
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Cerebral Palsy and Movement Disorders · Stroke Rehabilitation and Recovery
Introduction
One-third of older adults’ experience one or more falls annually, and falls are one of the leading causes of morbidity and mortality among this group [1]. Falls are considered a major health hazard as they can lead to serious injuries, reduce individuals’ health, and increase the need for healthcare services [2]. Over the last decade, there has been significant interest in how to prevent falls, and in 2022, the World Falls Guidelines were published [1]. In general, these guidelines recommend an increased focus on fall identification, multifactorial fall risk assessment, and tailored exercises focusing on strength and balance to reduce falls [1]. Despite solid evidence on how to prevent falls [1,3,4], its implementation in practice has been slow and limited [5,6]. Although fall prevention is regarded as an important task in the community setting, implementation of fall prevention guidelines is considered a complex process that requires systematic work of identifying barriers and facilitators within the health care services [7]. In community settings, implementation strategies have often been used unconsciously and unintentionally, through a trial and error method, to improve practice [7]. Barriers to implementation in the community setting are related to the underreporting of falls, lack of knowledge among healthcare providers, interventions’ incompatibility with practice, and the absence of financial incentives [6,8].
The implementation of research evidence into practice is considered a complex process [9]. Accumulated insights from implementation science highlight the need for a systematic approach. Such an approach involves identifying local barriers to the use of specific research [9] and addressing them with implementation strategies or methods designed to overcome these barriers, thus tailoring the uptake of evidence [10]. In 2015, a group of implementation experts formulated the Expert Recommendations for Implementing Change (ERIC) taxonomy, which comprises 73 implementation strategies [11]. The ERIC study aimed to establish a common understanding of implementation strategy terms and definitions by gathering input from diverse stakeholders in implementation science and practice. Several implementation strategies have been assessed for their effectiveness. The use of clinical decision support, practice visits, audit and feedback, employment of local opinion leaders, tailored interventions, and employee training are examples of implementation strategies that have improved healthcare professionals’ adherence to guidelines [12–14]. However, to the best of our knowledge, no reviews have assessed the effectiveness of similar implementation strategies for fall prevention in the community setting. Given that implementation is contextual, there is a need to tailor implementation strategies to fall prevention interventions and further explore effective strategies for implementation [15].
As a result, it remains unclear what the effective implementation strategies for preventing falls in the community setting are, posing a challenge for further practice. An overview of effective implementation strategies can provide insights for future research opportunities and inform the design of fall prevention interventions. Thus, the aim of this study was to assess the effectiveness of implementation strategies on implementation and health-related outcomes in community care for fall prevention.
Method
The protocol for this systematic review was registered with PROSPERO (ID = CRD42022233395). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was followed [16] (Additional file 1), complemented by the Synthesis Without Meta-analysis (SWiM) reporting guidelines [17].
Information source and search strategy
A systematic search was conducted and updated November 27^th^ 2024, using databases MEDLINE (Ovid), CINAHL, EMBASE, PsycINFO, Web of Science, the Cochrane Library, and Google Scholar. The search strategy was developed based on a similar review from 2011 [15], using MeSH terms and keywords for four elements: 1) Older adults, 2) Falls, 3) Prevention, and 4) Implementation. Additionally, we manually screened the reference lists of the included papers. The full search strategy is included in Additional File 2.
Eligibility criteria
The inclusion criteria are presented in Table 1. We included implementation studies that aimed to test strategies for the uptake of fall prevention interventions. While we anticipated that healthcare professionals would play a crucial role in most implementation strategies aimed at reducing falls, we also included studies where individuals other than healthcare professionals, such as family members or volunteers, played a more active role. For outcomes, we included all measures used to assess the effectiveness of the implementation strategy. Implementation outcomes considered were acceptability, adoption, appropriateness, feasibility, fidelity, penetration, and sustainability. Clinical outcomes considered eligible were falls and fall related consequences such as injuries etc. Conference abstracts and protocols were excluded.
Table 1: Inclusion criteria for study selection.
Study selection
References from the literature searches were imported into EndNote (version 21) and deduplicated. Titles and abstracts were then independently screened by the first author and a research assistant using the systematic review tool, Covidence [18]. In cases of disagreement at this stage, the article was included for full-text screening. Full-text articles were screened independently by pairs of authors (SL, LAHK, BG, KT, and TB), and then compared. Any disagreements were resolved by involving a third author.
Quality assessment
Risk of bias was independently assessed by pairs of authors (SL, LAHK, BG, and TB), using Version 2 of the Cochrane Risk of Bias Tool for Randomized Trials (RoB2) and the ROBINS-I tool [19]. The overall quality and certainty of evidence (Grading of Recommendations, Assessment, Development, and Evaluations) were not assessed due to the lack of effect sizes and confidence intervals within the results.
Data extraction
A data extraction form was developed using Microsoft Excel for 365 spreadsheet (Version 2002). We extracted: author, year, country, participant demographics, descriptions of the fall prevention intervention, details of the implementation strategy, outcome measures, and study results. Data were extracted verbatim by the first author and verified by the last. The ERIC compilation of implementation strategies were used to identify and categorize the implementation strategies [11]. Strategies were further clustered as suggested by Waltz et al. [20]. The table below (Table 2) describes the most relevant implementation strategies from the ERIC compilation [11] expected to be found in the included studies.
Table 2: Most relevant implementation strategies from ERIC compilation [11].
Synthesis methods
As we found variation in the interventions, comparators, and outcomes, we synthesized the results using vote-counting based on the direction of effect, as recommended in the Cochrane handbook [21]. Our approach followed the SWiM reporting guidelines [17] and the synthesis was done regardless of statistical significance [21]. We synthesized results for both implementation and clinical outcomes. For each outcome, the effects were categorized as either in favor of the implementation strategy or the control intervention without an implementation strategy. In cases where more than one outcome could be relevant from the study, we chose the outcome that was most relevant to answering our research question. We did not take the measurement timepoint into consideration. No hypothesis test or calculation of confidence interval for the estimate was conducted due to the low numbers in each analysis [21]. Missing outcome data was evaluated in the Risk of Bias assessment, as vote-counting based on the direction of effect does not account for this.
Amendments made to the protocol
Some amendments were made to the PROSPERO protocol (ID = CRD42022233395) due to the publication by Vandervelde et al. [15] that explored strategies used to implement multifactorial fall prevention interventions in the community. The review question was refined, and implementation studies were specified as the intervention of interest. Additionally, a restriction was applied to the control groups, emphasizing that the control group had to receive a fall prevention intervention similar to that of the intervention group.
Results
Study selection
We identified 8365 unique references eligible for title and abstract screening (see Fig 1). A total of 179 studies were screened in full text, resulting in the inclusion of four articles from three unique studies [22–25].
Flowchart for the inclusion of studies.
Study design, setting and fall prevention intervention
Two of the three studies were cluster-randomized at either the community level [23,25] or the county level [22], while the third was a non-randomized controlled trial in which each participating site had both an intervention and a control group [24]. One study was designed as a three-arm randomized trial, testing two implementation strategies [23,25]. All studies were conducted in the United States of America. Study-level characteristics are described in Table 3.
Table 3: Characteristics of included studies.
In two out of the three studies [22,23,25], the fall prevention intervention was Stepping On, a multifactorial program that addresses medication review, home modification, strength and balance exercises, community mobility, and vision [22]. Detailed description on how this intervention was conducted was only available for one of the studies, as described by Guse et al. [23] and Peterson et al. [25]. In this study, Stepping On was provided in group settings through 2-hour workshops held weekly over seven weeks. This was followed by a home visit or a phone call at ten weeks and a booster session at three months. In the final study, the fall prevention intervention consisted of screening older adults over 75 years for falls by asking three questions [24]. The results of these three questions were available for both the intervention and the control sites. However, only the intervention site received education on the appropriate response to the results.
Implementation strategies
The three included studies utilized multifaceted interventions, in which four to six strategies were combined. A total of 15 implementation strategies were described across the three studies. These studies included implementation strategies aimed at training and educating stakeholders, both healthcare providers and older adults. This included making training dynamic [23–25], distributing educational material [24], and conducting educational outreach visits [22]. The implementation strategies are presented in Table 3.
In the study by Ford et al. [22] the implementation intervention involved a change team, including a change leader, formulating and carrying out Plan-Do-Study-Act change cycles over a year. This process was accompanied by coaching, introductory education, and a site visit from the coach, which included an assessment of the context for implementation. The study described by Guse et al. [23] and Peterson et al. [25], had two study arms and one control arm and tested two different implementation strategies within the same study. In the first arm the intervention was called enhanced support, and comprised funding and a training compendium, support consisting of technical assistance and coaching, access to fall data, and an assessment of readiness. n the second arm the implementation intervention, was called standard support, and only comprised funding and a training compendium, [23,25]. Ganz et al. [24] described an implementation intervention that comprised four strategies: training of healthcare providers, use of a decision support system, audit and feedback on healthcare providers’ practice, and distribution of patient education handouts.
Implementation effectiveness
Ganz et al. [24] extracted information on five types of serious injuries from patient medical records as their primary outcome. The clinical outcome in Guse et al. [23] was fall injury morbidity in adults aged 65 years and older, measured by inpatient and emergency department discharge data. This study also included specific implementation outcomes to assess effectiveness of the two implementation interventions, measured as the number of Stepping On workshops, leaders, and participants. Compared to the control arm, only the enhanced support arm was associated with a significantly higher number of workshops, leaders and participants. Additionally, Peterson et al. [25] included the RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance) as a secondary outcome, but they did not report effect estimates between groups for this outcome. Ford et al. [22] used the number of completed workshops and the number of participants enrolled in the workshops as the implementation outcome in their study. They also included the number of falls, and the number of emergency department visits as secondary outcomes but did not report the effect between groups for these outcomes [22].
The vote-counting exercise of implementation outcomes revealed that two studies reported on the number of fall prevention interventions held, with both reporting results in favor of the implementation strategy. Both studies incorporated training and education of stakeholders as part of the implementation strategy. This suggests that using training and education of stakeholders in the implementation strategy resulted in a higher number of fall prevention interventions being held in the counties and thus more older adults being offered the fall prevention intervention [22,23].
The vote-counting exercise for clinical outcomes revealed that two studies reported on fall injuries resulting in emergency department or hospital admission. The results for this vote-counting were divergent, with one study favoring the implementation strategy, where using the implementation strategy resulted in fewer fall injuries leading to admission [23]. While the other study favored the control group, where using an implementation strategy resulted in a higher number of fall injuries leading to admission [24]. Both studies used an implementation strategy incorporating training and education of stakeholders. The results of the vote-counting analysis are presented in Table 4. Additionally, Ford et al. [22] reported results that were not part of the vote-counting analysis, as only one result from each study can be included. They indicated a significant increase in the number of interventions completed compared to the control group (7.62, p = .05).
Table 4: Vote counting results direction of effects on implementation outcomes and clinical outcomes.
Risk of bias
The risk of bias assessment revealed an overall high risk of bias for three of the outcomes included in the vote-counting analysis, whereas the remaining outcomes were judged to have some concerns. The high risk of bias was related to inadequate information about the timing of identification or recruitment of the sample, or due to confounding. The outcomes judged to have some concerns were related to a lack of information on deviations from the intended intervention. The risk of bias assessment is presented in Table 5.
Table 5: Results from the risk of bias assessment of outcomes included in the vote-counting analysis.
Discussion
This systematic review synthesized results from four articles, reporting three unique studies, that assessed the effectiveness of implementation strategies used to enhance fall prevention interventions for community-dwelling older adults. The studies employed various multifaceted implementation strategies, whereof all contained single strategies aimed at training and educating healthcare providers or service users. The vote-counting analysis demonstrated that employing an implementation strategy can be useful in increasing the number of fall prevention workshops held by counties and communities. However, the use of implementation strategies did not consistently reduce the number of falls leading to referral to acute care.
Surprisingly, only three unique studies met our eligibility criteria. The reasons for the low number of relevant studies are not obvious. One plausible reason could be that there has been lacking interest for implementation and challenging to publish studies with such focus. Additionally, it could be related to less funding for implementation science, which results in less expensive study designs. Another reason may be lack of implementation scientists in research teams. Other systematic reviews exploring implementation strategies have been less rigid regarding the designs included. For instance, Vandervelde et al. [15] imposed no restriction on study design when providing an overview of strategies used to implement multifactorial fall prevention interventions in the community. They included qualitative studies and studies conducted in various settings. Additionally, they utilized a slightly different definition of implementation strategies, describing them as methods or techniques aimed at enhancing the adoption of a “clinical intervention.” Still, they included three RCTs and three non-RCTs out of the 18 studies included [15]. However, the systematic review by Vandervelde et al. [15] aimed at summarize implementation strategies in multifactorial fall prevention interventions and had other eligibility criteria than used in this current systematic review. Similar results were seen in the review of Goodwin et al. [26] on the effectiveness of methods to implement falls prevention programs among community dwelling older adults. They neither limited the eligible criteria for study design, and only one of the six included studies had a controlled design. Despite this, randomized controlled designs are the most robust design to compare implementation strategies and evaluate effectiveness of implementation strategies [27].
The implementation strategies described in this review represented clusters of single strategies, where all of them aimed at training and educating stakeholders (healthcare providers or older adults) to enhance the implementation of fall prevention interventions. This was not surprising, as these strategies are suggested to enhance competence levels of the innovation, willingness to change, and create motivation among stakeholders [28]. The use of strategies to train and educate stakeholders was also identified as key in multifactorial fall prevention interventions, and more specifically, active learning, in the systematic review by Vandervelde et al. [15]. The use of education as part of the implementation strategy, to enhance competence is often employed in other clinical areas as well, such as the implementation of practice guidelines [14] or guidelines in nursing [29].
The vote-counting analysis for clinical outcomes yielded one study in favor of the implementation strategy and one in favor of the control, thereby not providing a clear direction of overall effect for the outcome. With so few studies reporting on clinical outcomes, it is difficult to determine if more studies would have provided a different result. It has been suggested to not employ clinical outcomes as measures of effect of implementation strategies, as they make it harder to distinguish the effects of the fall prevention intervention from the effects of the implementation strategy [30]. The progress of employing implementation outcomes has been criticized for being slow [31]. This also seems to be the case for implementation strategies for fall prevention, as only two of the included studies in our review reported effect estimates on implementation outcomes.
The included studies did not describe in detail their implementation strategy and lacked sufficient information for comparison. This finding aligns with the systematic review of Vandervelde et al. [15], indicating poor reporting practice when reporting guidelines have been available since 2013 [32]. Consequently, when implementation studies are included in systematic reviews the poor reporting also influenced the risk of bias assessment. The outcomes in our review were all assessed as either some concern or with high risk of bias.
Strengths and limitations
The strength of this review lies in the systematic nature of the review process and the transparency in reporting amendments and the use of PRISMA and SWiM reporting guidelines. The search strategy included going through the literature lists of relevant publications and systematic reviews identified in the search. Nevertheless, we did not search for grey literature or perform forward snowballing. Therefore, it is possible that we missed relevant studies. The included studies also demonstrated poor reporting on implementation strategies, thereby challenging the comparisons of implementation strategies. To ensure transparency in the review process, we registered the protocol in PROSPERO. However, the changes to the protocol may have introduced bias. These changes included specification of the aim, type of intervention, and control/comparison condition.
Implications for practice and research
This study does not provide sufficient evidence to determine which implementation strategies are most effective to employ when implementing fall prevention interventions in practice. For the implementation of such interventions, the use of a multifaceted implementation strategy should be considered to increase the success of these strategies and the uptake of evidence. Future research should consider providing thorough descriptions of implementation strategies and employing robust designs to further explore the effectiveness of these strategies and provide results on which ones to use.
Conclusion
This systematic review highlights a gap in research on the effectiveness of implementation strategies for the uptake of fall prevention interventions in practice. Employing an implementation strategy aimed at training and education stakeholders can be useful for increasing engagement in conducting fall prevention intervention. Considering the substantial evidence supporting effective interventions for fall prevention, it is critical to prioritize implementation studies in the field and secure financial support for implementation research. Researchers should strive to provide detailed descriptions of implementation strategies in accordance with reporting guidelines. There is a need for future studies with robust designs to determine the effectiveness of implementation strategies in fall prevention among community-dwelling older adults.
Supporting information
S1 FigPrisma checklist.Additional file 1: Prisma checklist.(DOCX)
S2 TableSearch strategy.Additional file 2: Search strategy.(DOCX)
S3 TableList of all included references.Additional file 3: List of all included references.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Montero-Odasso M, van der Velde N, Martin FC, Petrovic M, Tan MP, Ryg J, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. 2022;51(9):afac 205. doi: 10.1093/ageing/afac 205 36178003 PMC 9523684 · doi ↗ · pubmed ↗
- 2Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J Am Geriatr Soc. 2018;66(4):693–8. doi: 10.1111/jgs.15304 29512120 PMC 6089380 · doi ↗ · pubmed ↗
- 3Sherrington C, Michaleff ZA, Fairhall N, Paul SS, Tiedemann A, Whitney J. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51(24):1750–8.27707740 10.1136/bjsports-2016-096547 · doi ↗ · pubmed ↗
- 4Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;2012(9):CD 007146. doi: 10.1002/14651858.CD 007146.pub 3 22972103 PMC 8095069 · doi ↗ · pubmed ↗
- 5Child S, Goodwin V, Garside R, Jones-Hughes T, Boddy K, Stein K. Factors influencing the implementation of fall-prevention programmes: a systematic review and synthesis of qualitative studies. Implement Sci. 2012;7:91. doi: 10.1186/1748-5908-7-91 22978693 PMC 3576261 · doi ↗ · pubmed ↗
- 6van Rhyn B, Barwick A. Health Practitioners’ Perceptions of Falls and Fall Prevention in Older People: A Metasynthesis. Qual Health Res. 2019;29(1):69–79. doi: 10.1177/1049732318805753 30311840 · doi ↗ · pubmed ↗
- 7Linnerud S, Kvael LAH, Graverholt B, Idland G, Taraldsen K, Brovold T. Stakeholder development of an implementation strategy for fall prevention in Norwegian home care - a qualitative co-creation approach. BMC Health Serv Res. 2023;23(1):1390. doi: 10.1186/s 12913-023-10394-x 38082278 PMC 10714538 · doi ↗ · pubmed ↗
- 8Vandervelde S, Van den Bosch N, Vlaeyen E, Dierckx de CasterléB, Flamaing J, Belaen G, et al. Determinants influencing the implementation of multifactorial falls risk assessment and multidomain interventions in community- dwelling older people: a systematic review. Age Ageing. 2024;53(7):afae 123. doi: 10.1093/ageing/afae 123 38952187 · doi ↗ · pubmed ↗