A paediatric patient with PRAKG2 cardiomyopathy: Look at the red flags
Ana Rita Bello, João Franco-Machado, Inês Carmo Mendes, Bruno M L Rocha

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
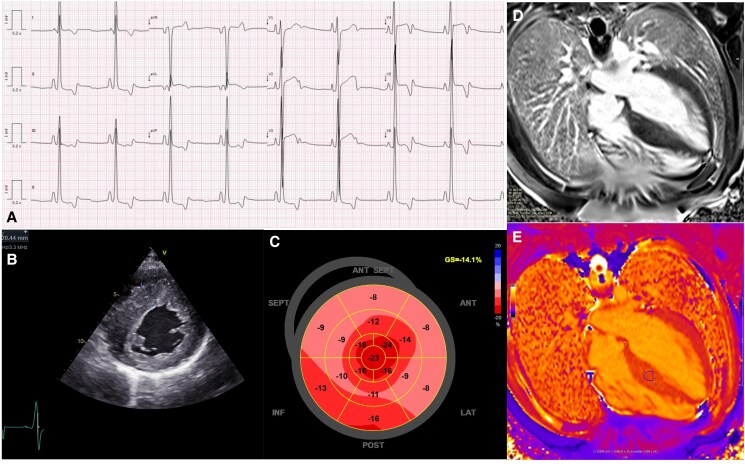 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Congenital heart defects research · Cardiovascular Function and Risk Factors
Case presentation
A 13-year-old Pakistani boy was referred for cardiovascular screening due to unexplained syncope. The first episodes began at the age of 8 years old, associated with physical activity, and became increasingly more frequent in the last months. He had no other complaints (e.g. fatigue, palpitations, chest discomfort). There was no family history of sudden cardiac death (SCD) nor known structural heart disease.
The ECG (Figure 1A) showed sinus bradycardia, short PR interval, no pre-excitation, and biphasic T-waves. The transthoracic echocardiogram showed severe left ventricular (LV) hypertrophy, preserved LV ejection fraction, and mildly reduced global longitudinal strain (Figure 1B; Supplementary Material online, Video S1A–C). On magnetic resonance, there was discrete late gadolinium enhancement in the septum, with normal global T1 mapping values (Figure 1D and E). The laboratory assessment showed a slightly elevated NT-proBNP (230 pg/mL) and spurious proteinuria (urine protein-to-creatinine ratio: 2105 mg/g). The latter, most probably, due to analytical interference of a glycogen metabolite (see Supplementary material online, Figure S1).
(A) ECG—Sinus bradycardia at 50bpm, short PR interval (100 ms), without delta waves (pre-excitation), and difuse biphasic/inversion of T-waves (pre-cordial leads, DI and aVL leads and V4-6 and DII), and borderline QTc (automatic 452 ms). (B) TTE—short axis demonstrating increased asymmetrical septal LV wall thickness (19 mm; z score 6). (C) TTE—reduced global longitudinal strain (−14.1%). (D, E) Cardiac magnetic resonance—presence of mild patchy late-gadolinium enhancement in the interventicular septum and increased T1 mapping values (E, circle) in the same region; there were no morphological signs suggestive of sarcomeric hypertophic cardiomyopathy; global T1 mapping values were within normal range (1010 ms; reference centre: 900 to 1050 ms).
Following genetic counselling, the patient underwent testing following a hypertrophic cardiomyopathy panel including 38 genes (see Supplementary Material online), revealing a heterozygous pathogenic variant in the PRKAG2 gene [OMIM#602743] [NM_016203.4:c.905G > A (p.Arg302Glu)]. His parents tested negative for this variant, supporting a de novo mutation. Recurrent syncope on exertion, massive LV hypertrophy and PRKAG2 Glycogen Storage Disease Cardiomyopathy were considered to potentially increase the risk of SCD, despite no malignant arrhythmias on 48h-Holter monitoring and exercise stress test. Accordingly, the multidisciplinary discussion favoured the use of an implantable cardio-defibrillator. A transvenous approach was preferred, since SCD is reported in up to 10% of the patients, often due to advanced heart block^1,2^
This case underscores the importance of the genetic aetiological identification in paediatric cardiomyopathy. Moreover, it suggests that spurious proteinuria, arising from the interference of a glycogen metabolite, may be a potential new diagnostic ‘red flag’.^3^
Supplementary Material
ytaf302_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Porto AG, Brun F, Severini GA, Losurdo P, Fabris E, Taylor MRG, et al Clinical spectrum of PRKAG 2 syndrome. Circ Arrhythm Electrophysiol 2016;9:e 003121.26729852 10.1161/CIRCEP.115.003121 PMC 4704128 · doi ↗ · pubmed ↗
- 2Sternick EB, Oliva A, Magalhães LP, Gerken LM, Hong K, Santana O, et al Familial pseudo-wolff-Parkinson-white syndrome. J Cardiovasc Electrophysiol 2006;17:724–732.16836667 10.1111/j.1540-8167.2006.00485.x · doi ↗ · pubmed ↗
- 3Piraud M, Pettazzoni M, Antonio M, Vianey-Saban C, Froissart R, Chabrol B, et al Urine glucose tetrasaccharide: a good biomarker for glycogenoses type II and III? A study of the French cohort. Molec Genet Metab Rep 2020;23:100583.32382504 10.1016/j.ymgmr.2020.100583 PMC 7200937 · doi ↗ · pubmed ↗