Effect of Prophylactic Tranexamic Acid on Peripartum Changes in Haemoglobin Concentration After Vaginal Delivery
Ezukwa E. Omoronyia, Moses I. Ekuma, Edu Eyong, Sylvester E. Abeshi, Ubong B. Akpan

TL;DR
This study shows that adding tranexamic acid to oxytocin after vaginal delivery helps prevent a drop in hemoglobin levels, which is important for preventing postpartum anemia.
Contribution
The study demonstrates that prophylactic tranexamic acid, when combined with oxytocin, effectively reduces postpartum hemoglobin decline in low-risk deliveries.
Findings
Tranexamic acid plus oxytocin significantly increased postpartum hemoglobin concentration compared to oxytocin alone.
No major maternal side effects were observed in either group.
The combination is recommended for active management of the third stage of labor.
Abstract
This study aimed to evaluate the effect of prophylactic intravenous tranexamic acid on postpartum haemoglobin (Hb) concentration values compared to a control group. This randomised controlled study took place from May to July 2023 and included parturients with no apparent risk for postpartum haemorrhage from the University of Calabar Teaching Hospital in Calabar, Nigeria. Participants were divided equally into 2 groups. Group A (intervention group) received 10 IU of intramuscular oxytocin along with 1,000 mg of intravenous tranexamic acid within 1 minute of vaginal delivery, while Group B (control group) received 10 IU of intramuscular oxytocin with 10 mL of sterile water. The primary outcome measure was the difference in admission and postpartum Hb concentration. A total of 80 parturients were included in this study; 40 were allocated to each study arm. The demographic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
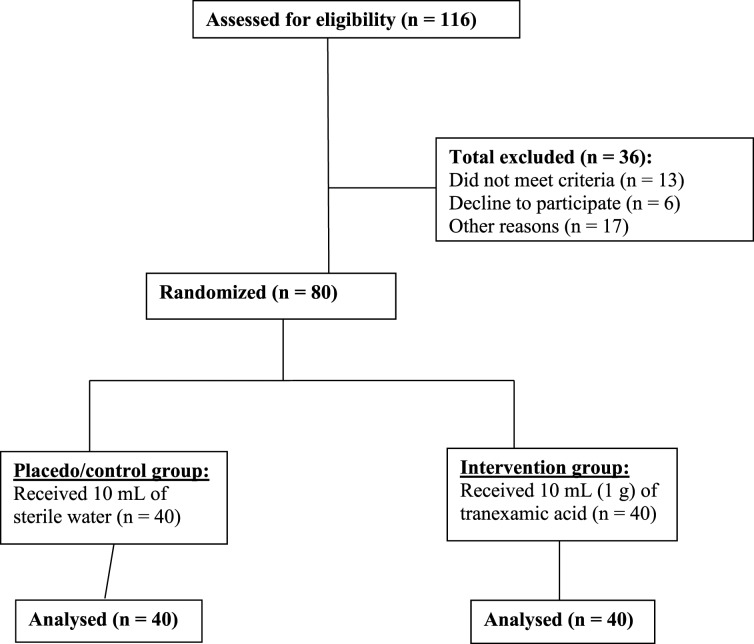 Fig. 1
Fig. 1| n (%) | |||
|---|---|---|---|
|
| |||
| Variable | Group A (n = 40) | Group B (n = 40) | |
| Age group in years | |||
| 21–25 | 8 (20.0) | 6 (15.0) | 0.44 |
| 26–30 | 12 (30.0) | 14 (35.0) | |
| 31–35 | 20 (50.0) | 20 (50.0) | |
| Parity | |||
| 1 | 2 (5.0) | 2 (5.0) | |
| 2 | 25 (62.5) | 24 (60.0) | |
| 3 | 7 (17.5) | 9 (22.5) | |
| 4 | 6 (15.0) | 5 (12.5) | |
| Variable | Mean ± SD | T | |
|---|---|---|---|
|
| |||
| Group A | 28.88 ± 3.67 | - 0.26 | 0.798 |
| Group B | 29.08 ± 3.29 | ||
|
| |||
| Group A | 38.85 ± 0.74 | - 0.38 | 0.708 |
| Group B | 38.93 ± 1.02 | ||
|
| |||
| Group A | 3.50 ± 0.60 | - 0.39 | 0.699 |
| Group B | 3.55 ± 0.55 |
| Variable | Mean ± SD | T | |
|---|---|---|---|
|
| |||
| Group A | 10.95 ± 0.44 | - 0.24 | 0.809 |
| Group B | 10.97 ± 0.49 | ||
|
| |||
| Group A | 10.28 ± 0.59 | 6.21 | <0.001 |
| Group B | 9.44 ± 0.62 |
| Mean Hb | ||||
|---|---|---|---|---|
| Hb Concentration | Mean ± SD | difference | T | |
|
| ||||
| Admission Hb | 10.95 ± 0.45 | 0.67 | 10.37 | <0.001 |
| Post-delivery Hb | 10.28 ± 0.59 | |||
|
| ||||
| Admission Hb | 10.98 ± 0.49 | 1.53 | 18.78 | <0.001 |
| Post- delivery Hb | 9.44 ± 0.62 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Maternal and fetal healthcare
1. Introduction
Over half a million women die each year while attempting to give birth, with 99% of all maternal deaths occurring in underdeveloped countries. These tragedies are largely preventable.^1^ Maternal death plunges the immediate family into profound hardship, deprives children of essential maternal care and leaves partners in loneliness, agony and despair as they lose both economic and emotional support. Additionally, the country suffers a loss of both material and human resources, as these women often represent the cornerstone of their families.^2^
Postpartum haemorrhage (PPH), along with hypertension and infection, constitutes the triad of causes of maternal deaths in both underdeveloped and developed countries.^1^ Postpartum blood loss of 500 mL or more following a vaginal delivery, 1,000 mL or more following a caesarean delivery or any amount of blood loss that causes haemodynamic compromise after delivery is referred to as PPH.^3^ The most common cause of PPH is uterine atony, with genital tract lacerations, retained products of conception, ruptured uterus and coagulation defects being other causes.^3456^
Apart from maternal mortality, morbidities that may complicate PPH include anaemia, renal failure, puerperal sepsis and Sheehan's syndrome. Although blood transfusions may alleviate anaemia and some other complications of PPH, they carry risks of transfusion reactions and infections, especially HIV and hepatitis B.^78^
The availability of blood and blood products remains precarious, especially in developing countries with inadequate blood banking services and epileptic power supply. Furthermore, blood and blood products are often expensive. Several preventive measures have been implemented to reduce postpartum blood loss. Prostaglandin E1 analogue (misoprostol) or oxytocin in the active management of the third stage of labour (AMTSL) is effective in reducing maternal blood loss by 30%, lowering PPH risk, shortening the third stage of labour duration and decreasing the need for blood transfusion.^910^
A meta-analysis on the use of oxytocin in the AMTSL found that PPH still occurs despite the use of this gold-standard first-line drug.^10^ Additionally, considering that many women in developing countries enter pregnancy and labour with borderline haemoglobin (Hb) levels, even minimal blood loss can become critical.^10^ Hence, there is a continued need to explore more effective methods for reducing postpartum blood loss, minimising the decrease in postpartum Hb levels, alleviating postpartum anaemia and decreasing the need for blood transfusions.
Tranexamic acid is a potent anti-fibrinolytic agent derived from lysine that inhibits both plasminogen activation and plasmin activity by blocking their binding sites, thereby preventing the breakdown of already-formed blood clots.^1112^ Its safety has been established over several years. Tranexamic acid is largely available, affordable and stable at room temperature, which means it does not depend on an erratic power supply or inadequate infrastructure for preservation. The World Health Organization recommends that tranexamic acid be administered via the intravenous route when used in the treatment of primary PPH.
Tranexamic acid is rapidly absorbed, with an onset of action occurring within 5 to 15 minutes and a duration of action lasting 3 hours. Approximately 3% of the drug is protein-bound, primarily to plasminogen. Its half-life is approximately 2 hours, and about 95% is excreted unchanged in the urine.^12^ Tranexamic acid is administered as a loading dose of 1,000 mg in 10 mL, infused over 10 minutes. This medication is heat-stable, safe and well-tolerated. It is effective in preventing bleeding after trauma, managing primary menorrhagia and treating intrauterine contraceptive device-induced bleeding.^13^
The results of the World Maternal Anti-Fibrinogen Trial (a large randomised controlled trial), published in 2017, showed that the early administration of intravenous tranexamic acid (1 g) within 3 hours of the onset of PPH in women, where uterotonics have failed to control bleeding, significantly reduces mortality due to haemorrhage, regardless of the underlying cause, and does not result in any adverse maternal effects.^141516^ The current study aimed to examine whether the prophylactic addition of tranexamic acid to the routine AMTSL following vaginal delivery is an effective strategy for reducing postpartum blood loss, postpartum anaemia and other complications associated with postpartum anaemia, including the need for blood transfusions and related products.
2. Methods
This study was conducted in the labour ward of the University of Calabar Teaching Hospital, Calabar, Nigeria, which also serves as a referral centre for primary, secondary and private health facilities in the state and surrounding areas. Additionally, it functions as a training and research centre. The study took place over a 3-month period, from May to July 2023.
The participants in this study were pregnant women at term who were in the active phase of labour for vaginal delivery with a single fetus in a longitudinal lie and cephalic presentation. They had no contraindications to vaginal delivery, were willing to participate in the study and had no contraindications to the use of tranexamic acid. The exclusion criteria were as follows: induction of labour, augmentation of labour, fetal macrosomia, prolonged labour, grand multiparity, caesarean deliveries, polyhydramnios, previous history of primary PPH, previous uterine surgery, pre-eclampsia/eclampsia, placental abruption, retained placenta, use of high doses of low molecular weight heparin, bleeding from genital tract lacerations/episiotomies, maternal age over 35 years and primigravidae.
This study was a randomised experimental investigation into the effects of prophylactic intravenous tranexamic acid plus oxytocin versus oxytocin plus placebo on the peripartum change in Hb concentration after vaginal delivery.
The minimum sample size for the study was determined using the sample size formula for a randomised controlled trial with a numerical outcome, as stated below:
Where, N = minimum sample size, Zα = standard normal deviation correspondingly to an α level of 5% (i.e. 1.96), Zβ = standard normal deviation corresponding to a power of 80% (i.e. 0.84), σ = standard deviation of postpartum Hb concentration (i.e. 1.4 g/dL) and μt – μs = minimum clinically important difference between pre and postpartum Hb concentrations (assumed to be 1.0 g/dL for this study).
By assuming a non-response rate of 10% and an attrition rate of 10% (i.e. r = 20% or 0.2), the calculated sample size was rounded up to 40 parturients in each of the arm of the study.
Each participant was randomised using a computer-generated random number from the software Research Randomizer, Version 4.0 (Urbaniak GC, Plous S. Research Randomizer software). The generated random numbers were then followed sequentially across the rows to determine the group allocation of eligible participants. Even numbers were allocated to Group A (intervention group), while odd numbers were assigned to Group B (control group). The resulting allocation sequence was concealed in opaque envelopes labelled from 1 to 80, which were used to determine the group assignment of each eligible participant as they presented in the labour ward.
Group A received 1,000 mg (10 mL) of tranexamic acid intravenously, along with 10 IU of intramuscular oxytocin, within 1 minute of the baby's delivery. Group B received 10 mL of sterile water intravenously in addition to 10 IU of oxytocin within 1 minute of the baby's delivery. Tranexamic acid and sterile water were drawn into separate white 10 cc syringes, which were then capped and labelled as A or B. The concealment process was done by a pharmacist at the hospital, who transferred the contents of the tranexamic acid ampoules into the syringes and subsequently labelled them as sterile water without informing the researcher of the actual contents. The labelled syringes containing either tranexamic acid or sterile water were stored in the refrigerator in the labour ward, where trained research team members could access them.
A thorough history and clinical examination were done to confirm the active phase of labour. A proforma was used to document the sociodemographic characteristics, vital signs and other relevant information about the patients. The consenting women had a tourniquet applied to their arms, and the site for blood collection was cleaned with a methylated spirit swab. An amount of 2 mL of blood was drawn into an ethylenediaminetetraacetic acid sample container for the determination of admission Hb concentration.
The third stage of labour was actively managed in both arms using 10 IU of intramuscular oxytocin administered within 1 minute of the baby's delivery. The deliveries were conducted by experienced resident doctors and/or experienced midwives to minimise genital tract trauma and associated bleeding. Patients who voluntarily withdrew from the study, as well as those who needed a blood transfusion or caesarean section during labour, were excluded. Additionally, patients with PPH were also removed.
The Hb concentration was analysed using the ‘Mission RHb Hemoglobin Testing System’, a digital Hb meter manufactured by ACON Laboratories Incorporation (Mesa Rim Road, San Diego, CA, USA). The Mission RHb Hemoglobin test strip was also used.
The results from the haemoglobinometer were periodically evaluated by conducting repeat tests at the main laboratory and comparing these results with those previously obtained from the haemoglobinometer. The Hb concentration of all participants was repeated 48 hours after delivery. All participants were monitored until their discharge from the hospital, after which they left the study.
To ensure quality control, all tranexamic acid used in the study was procured from a company (Protech Biosystems Pvt. Ltd, Haryana, India) under the same brand name (Prexam Injection) and batch number. Similarly, the oxytocin was sourced from a company (Shanxi Shuguang Pharm. Co., Ltd., JinZhong City, China) under the same brand name (Pitons Oxytocin Injection) and batch number. Both the drugs were stored at a consistent temperature and administered only to those who met the inclusion criteria by trained personnel.
The outcome measures were as follows: (1) estimation of admission Hb concentration; (2) estimation of postpartum Hb concentration; (3) postpartum drop in Hb concentration after 48 hours of delivery, calculated as the difference between the admission Hb concentration and the Hb concentration at 48 hours after delivery; and (4) maternal adverse effects of tranexamic acid.
Data collected were tabulated and analysed using the Statistical Package for the Social Sciences (SPSS) software, Version 23 (IBM, Chicago, IL, USA). The outcome measures were compared between the 2 groups. The mean values of continuous variables were tested for statistical significance using an independent t-test, while discrete values were analysed for statistical significance using the Chi-square test. The level of statistical significance was set at P <0.05.
3. Results
A total of 116 parturients were assessed for eligibility. Of these, 36 were excluded; the remaining 80 parturients were randomised to receive either Group A or B [Fig. 1]. The mean ages of the parturients in Group A and B were 28.88 ± 3.67 and 29.08 ± 3.29 years, respectively. Pregnant women in both groups were comparable in terms of age distribution and parity [Table 1]. Additionally, the expected gestational ages and babies' birth weights were not significantly different between the two groups [Table 2].
Flowchart showing the selection process of parturients.
The proportion of parturients who reported side effects (e.g., nausea and vomiting) from the drugs was 2.5% in each group. There was no significant difference (P = 0.809) in the mean admission Hb concentration between the 2 groups. A significant difference was observed (P <0.001) in the post-delivery Hb concentrations between the 2 groups [Table 3].
There were significant differences when comparing admission Hb concentrations to post-delivery Hb concentrations in both Group A and B (P <0.001 each). Specifically, there was a reduction in the mean Hb concentrations post-delivery compared to the time of admission. However, the mean reduction in Hb concentration was greater in Group B (1.53 mg/dL) compared to the mean Hb reduction in Group A (0.67 mg/dL) [Table 4].
4. Discussion
PPH is a life-threatening event. Interventions to prevent PPH have always been the basic standard of care provided to women during delivery. This study aimed to evaluate the effect of prophylactic administration of tranexamic acid on Hb concentration in the peripartum period after vaginal delivery.
The results of the present study demonstrate that the prophylactic addition of 1,000 mg of intravenous tranexamic acid to routine AMTSL after vaginal delivery is associated with a statistically significant reduction in postpartum Hb drop in the intervention group (tranexamic acid; Group A) compared to the control group (placebo; Group B). This finding is consistent with other studies.^171819^ The significant reduction in postpartum Hb drop observed in Group A may be explained by the effect of tranexamic acid in reducing postpartum blood loss. This effect is due to its action in inhibiting the lysis of fibrinogen formed on the placental bed and on minor lacerations that may have occurred in the genital tract during vaginal delivery.
The significant reduction in postpartum Hb drop is particularly important for women in developing countries, where anaemia, caused by either nutritional or environmental factors, is prevalent among pregnant women.^20^ A relatively small reduction in postpartum Hb drop may be clinically relevant, especially considering the mean pre-delivery Hb of women in this study was 10.96%. This finding further bolsters the need to minimise postpartum blood loss.
The present study further confirms the safety of tranexamic acid when used prophylactically to reduce postpartum blood loss, as 97.5% of the study subjects had no side effects from the drug. Only 2.5% of the participants reported nausea and vomiting, which was not significantly higher in Group A compared to Group B. This finding is consistent with previous studies.^171819212223^ Other side effects recorded in the study conducted by Ducloy-Bouthors et al. may be attributed to the higher dose (4 g) of tranexamic acid used by them compared to the 1 g of tranexamic acid administered in the current study.^24^
5. Conclusion
The mean postpartum Hb concentration in the intervention group (tranexamic acid) was significantly higher than that in the control group (placebo). This finding indicates that the prophylactic administration of tranexamic acid during vaginal delivery is effective in reducing postpartum Hb drop. Additionally, tranexamic acid demonstrates a favourable safety profile when used for this purpose.
Authors' Contribution
Ezukwa E. Omoronyia: Conceptualization, Methodology, Investigation, Data Curation, Writing – Original Draft. Moses I. Ekuma: Conceptualization, Methodology, Investigation, Data Curation, Writing – Original Draft. Edu Eyong: Writing – Original Draft. Sylvester E. Abeshi: Methodology, Investigation, Data Curation, Writing – Original Draft. Ubong B. Akpan: Writing – Original Draft, Writing – Review & Editing.
Ethics Statement
Ethical clearance was obtained from the Health Research Ethics Committee of the University of Calabar Teaching Hospital before commencing the study (HREC/07/10/2012). The study was registered as a randomised controlled trial with the Pan African Clinical Trial Registry. A signed or thumb-printed consent was obtained from each participant before their recruitment into the study. Participants were educated about the study's aims, objectives and procedures and informed that they could withdraw from the study at any time without facing any adverse consequences. All information, including patient identities and the results obtained, was kept confidential by the researcher.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received for this study.
Data Availability Statement
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cunningham FG Leveno K Bloom Spong C Dashe J Hoffman B Casey B. Williams Obstetrics, 24th ed. New York City, New York, USA: Mc Graw-Hill Education, 2014. pp. 780–828.
- 2Sambo AA Ijaiya MA Nwachukwu D Nwosu IC Idris H Abdullateef RM. A randomized controlled study comparing oral misoprostol with intramuscular oxytocin in active management of third stage of labour. Obstet Gynecol Sci 2024; 67:279–85. https://doi.org/10.5468/ogs.23128.10.5468/ogs.2312838409787 PMC 11099097 · doi ↗ · pubmed ↗
- 3World Health Organization. Postpartum Hemorrhage. Geneva, Switzerland:World Health Organization, 2019.
- 4Patek K Friedman P. Postpartum hemorrhage-epidemiology, risk factors, and causes. Clin Obstet Gynecol 2023; 66:344–56. https://doi.org/10.1097/GRF.0000000000000782.10.1097/GRF.000000000000078237130373 · doi ↗ · pubmed ↗
- 5Du Y Ye M Zheng F. Active management of the third stage of labor with and without controlled cord traction: A systematic review and meta-analysis of randomized controlled trials. Acta Obstet Gynecol Scand 2014; 93:626–33. https://doi.org/10.1111/aogs.12424.10.1111/aogs.1242424828584 · doi ↗ · pubmed ↗
- 6Scott JR Gibbs RS Karlan BY. Complications of delivery. In: Danforth's Obstetrics and Gynecology, 11th ed. Philadelphia, PA, USA:Lippincott Williams & Wilkins, 2022. pp. 452–61.
- 7Charles D Anger H Dabash R Darwish E Ramadan MC Mansy A. Intramuscular injection, intravenous infusion, and intravenous bolus of oxytocin in the third stage of labor for prevention of postpartum hemorrhage: A three-arm randomized control trial. BMC Pregnancy Childbirth 2019; 19:38. https://doi.org/10.1186/s 12884-019-2181-2.10.1186/s 12884-019-2181-230658605 PMC 6339323 · doi ↗ · pubmed ↗
- 8Pacheco LD Hankins GDV Saad AF Costantine MM Chiossi G Saade GR. Tranexamic acid for the management of obstetric hemorrhage. Obstet Gynecol 2017; 130:765–9. https://doi.org/10.1097/AOG.0000000000002253.10.1097/AOG.000000000000225328885402 · doi ↗ · pubmed ↗