Antibiotic Use by Paediatric Residents of the Oman Medical Specialty Board: Identifying opportunities for antimicrobial stewardship
Shaima Alshukaili, Hussain Al-Saffar, Hatem Al-Rawahi, Laila Al Yazidi

TL;DR
This study assesses how well pediatric residents in Oman follow antibiotic guidelines and finds areas needing improvement to reduce antibiotic resistance.
Contribution
The study identifies specific gaps in antibiotic prescription knowledge among pediatric residents in Oman, highlighting the need for targeted educational interventions.
Findings
Residents showed high adherence to guidelines for acute sinusitis and meningitis but low adherence for acute otitis media and cellulitis.
There was no significant difference in antibiotic knowledge between senior and junior residents.
Residents demonstrated good clinical judgment by consulting specialists when needed.
Abstract
This study aimed to evaluate antibiotic prescription knowledge and practices among Oman Medical Specialty Board (OMSB) paediatric residents. The goal was to identify educational opportunities to reduce antimicrobial resistance and improve patient care. A survey-based cross-sectional study was conducted among the OMSB paediatric residents from August 2023 to September 2023. The online survey involved three parts: residents' demographics, knowledge of 12 common paediatric infection scenarios and clinical practice. Participants were asked to choose the proper antibiotic choices and duration for each scenario. Data analysis was performed using SPSS. A total of 74 responses were obtained, resulting in an 84% response rate. No significant differences were observed in the knowledge of antibiotic prescriptions among paediatric residents at different stages of their residency. The highest…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
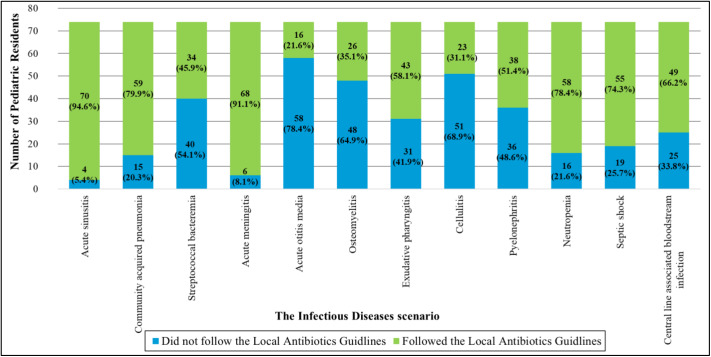 Fig. 1
Fig. 1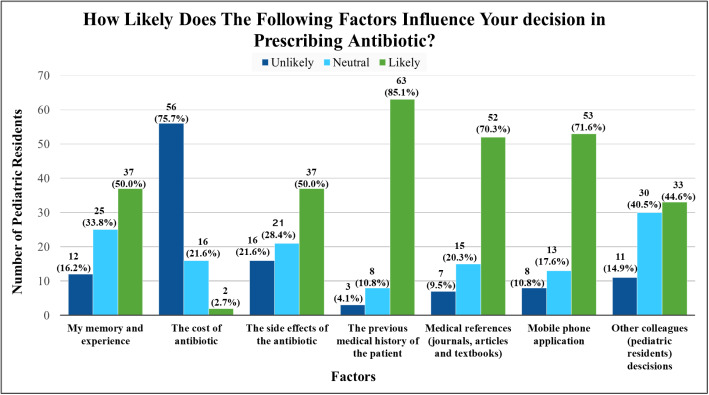 Fig. 2
Fig. 2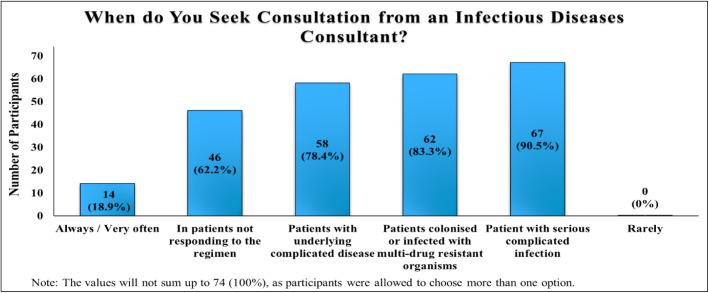 Fig. 3
Fig. 3| Demographics | n (%) |
|---|---|
|
| |
| Male | 13 (17.6) |
| Female | 61 (82.4) |
|
| |
| ≤27 | 13 (17.6) |
| 28 | 14 (18.9) |
| 29 | 19 (25.7) |
| 30 | 19 (25.7) |
| ≥31 | 9 (12.2) |
|
| |
| SQU | 44 (59.5) |
| Non-SQU | 30 (40.5) |
|
| |
| R1 | 23 (31.1) |
| R2 | 19 (25.7) |
| R3 | 18 (24.3) |
| R4 | 14 (18.9) |
|
| |
| No | 53 (71.6) |
| Yes | 21 (28.4) |
| Being in an ID rotation, n (%) | |||||
|---|---|---|---|---|---|
|
| |||||
| Cases | No | Yes | Total (N = 74) | CI | |
|
| |||||
| Inappropriate antibiotic | 3 (5.7) | 1 (4.8) | 4 (5.4) | 1.000 | 0.118–12.233 |
| Appropriate antibiotic | 50 (94.3) | 20 (95.2) | 70 (94.6) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 1 (2.0) | 1 (5.0) | 2 (2.7) | 0.493 | 0.023–6.518 |
| Appropriate duration | 49 (98.0) | 19 (95.0) | 68 (91.9) | ||
| Duration total | 50 (67.6) | 20 (27.0) | 70 (94.6) | ||
|
| |||||
| Inappropriate antibiotic | 11 (20.8) | 4 (19.0) | 15 (20.3) | 1.000 | 0.311–3.986 |
| Appropriate antibiotic | 42 (79.2) | 17 (81.0) | 59 (79.7) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 25 (59.5) | 12 (70.6) | 37 (50.0) | 0.618 | 0.182–2.058 |
| Appropriate duration | 17 (40.5) | 5 (29.4) | 22 (29.7) | ||
| Duration total | 42 (56.7) | 17 (23.0) | 59 (79.7) | ||
|
| |||||
| Inappropriate antibiotic | 30 (56.6) | 10 (47.6) | 40 (54.1) | 0.660 | 0.520–3.956 |
| Appropriate antibiotic | 23 (43.4) | 11 (52.4) | 34 (45.9) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 14 (60.9) | 9 (81.8) | 23 (31.0) | 0.271 | 0.060–1.981 |
| Appropriate duration | 9 (39.1) | 2 (18.2) | 11 (14.9) | ||
| Duration total | 23 (31.0) | 11 (14.9) | 34 (45.9) | ||
|
| |||||
| Inappropriate antibiotic | 5 (9.4) | 1 (4.8) | 6 (8.1) | 0.668 | 0.229–18.981 |
| Appropriate antibiotic | 48 (90.6) | 20 (95.2) | 21 (28.4) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 9 (18.8) | 5 (25.0) | 14 (18.9) | 0.743 | 0.199–2.404 |
| Appropriate duration | 39 (81.3) | 15 (75.0) | 54 (72.9) | ||
| Duration total | 48 (64.8) | 20 (27.0) | 68 (91.8) | ||
|
| |||||
| Inappropriate antibiotic | 41 (77.4) | 17 (81.0) | 58 (78.4) | 1.000 | 0.227–2.848 |
| Appropriate antibiotic | 12 (22.6) | 4 (19.0) | 16 (21.6) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 3 (25.0) | 1 (25.0) | 4 (5.4) | 1.000 | 0.073–13.644 |
| Appropriate duration | 9 (75.0) | 3 (75.0) | 12 (16.2) | ||
| Duration total | 12 (16.2) | 4 (5.4) | 16 (21.6) | ||
|
| |||||
| Inappropriate antibiotic | 34 (64.2) | 14 (66.7) | 48 (64.9) | 1.000 | 0.308–2.600 |
| Appropriate antibiotic | 19 (35.8) | 7 (33.3) | 26 (35.1) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - |
| Appropriate duration | 19 (100.0) | 7 (100.0) | 26 (35.1) | ||
| Duration total | 19 (100.0) | 7 (100.0) | 26 (35.1) | ||
|
| |||||
| Inappropriate antibiotic | 25 (47.2) | 6 (28.6) | 31 (41.9) | 0.230 | 0.751–6.636 |
| Appropriate antibiotic | 28 (52.8) | 15 (71.4) | 43 (58.1) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 10 (35.7) | 2 (13.3) | 12 (16.2) | 0.164 | 0.675–19.326 |
| Appropriate duration | 18 (64.3) | 13 (86.7) | 31 (41.9) | ||
| Duration total | 28 (37.8) | 15 (20.3) | 43 (58.1) | ||
|
| |||||
| Inappropriate antibiotic | 39 (73.6) | 12 (57.1) | 51 (68.9) | 0.272 | 0.725–6.020 |
| Appropriate antibiotic | 14 (26.4) | 9 (42.9) | 23 (31.1) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 2 (14.3) | 0 (0.0) | 2 (2.7) | 0.502 | - |
| Appropriate duration | 12 (85.7) | 9 (100) | 21 (28.4) | ||
| Duration total | 14 (18.9) | 9 (12.2) | 23 (31.1) | ||
|
| |||||
| Inappropriate antibiotic | 27 (50.9) | 9 (42.9) | 36 (48.6) | 0.71 | 0.500–3.833 |
| Appropriate antibiotic | 26 (49.1) | 12 (57.1) | 38 (51.3) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 2 (7.7) | 0 (0.0) | 2 (2.7) | 1.000 | - |
| Appropriate duration | 24 (92.3) | 12 (100) | 36 (48.6) | ||
| Duration total | 26 (35.1) | 12 (16.2) | 38 (51.3) | ||
|
| |||||
| Inappropriate antibiotic | 12 (22.6) | 4 (19.0) | 16 (21.6) | 1.000 | 0.351–4.407 |
| Appropriate antibiotic | 41 (77.4) | 17 (81.0) | 58 (78.4) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 41 (100) | 15 (88.2) | 56 (75.7) | 0.082 | - |
| Appropriate duration | 0 (0.0) | 2 (11.8) | 2 (2.7) | ||
| Duration total | 41 (55.4) | 17 (23) | 58 (78.4) | ||
|
| |||||
| Inappropriate antibiotic | 16 (30.2) | 3 (14.3) | 19 (25.7) | 0.264 | 0.669–10.065 |
| Appropriate antibiotic | 37 (69.8) | 18 (85.7) | 55 (74.3) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 7 (18.9) | 0 (0.0) | 7 (9.4) | 0.082 | - |
| Appropriate duration | 30 (81.1) | 18 (100) | 48 (64.9) | ||
| Duration total | 37 () | 18 (24.3) | 55 (74.3) | ||
|
| |||||
| Inappropriate antibiotic | 19 (35.8) | 6 (28.6) | 25 (33.8) | 0.746 | 0.465–4.200 |
| Appropriate antibiotic | 34 (64.2) | 15 (71.4) | 49 (66.2) | ||
| Antibiotic total | 53 (71.6) | 21 (28.3) | 74 (100) | ||
| Inappropriate duration | 1 (2.9) | 0 (0.0) | 1 (1.3) | 1.000 | - |
| Appropriate duration | 33 (97.1) | 15 (100) | 48 (64.9) | ||
| Duration total | 34 (45.9) | 15 (20.3) | 49 (66.2) | ||
| Year of residency, n (%) | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Cases | R1 | R2 | R3 | R4 | Total (N = 74) | |
|
| ||||||
| Inappropriate antibiotic | 1 (4.3) | 1 (5.3) | 1 (5.6) | 1 (7.1) | 4 (5.4) | 1.000 |
| Appropriate antibiotic | 22 (95.7) | 18 (94.7) | 17 (94.4) | 13 (92.9) | 70 (94.6) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 0 (0.0) | 0 (0.0) | 1 (5.9) | 1 (7.7) | 2 (2.7) | 0.243 |
| Appropriate duration | 22 (100) | 18 (100) | 16 (94.1) | 12 (92.3) | 68 (91.9) | |
| Duration total | 22 (29.7) | 18 (24.3) | 17 (23) | 13 (17.6) | 70 (94.6) | |
|
| ||||||
| Inappropriate antibiotic | 8 (34.8) | 1 (5.3) | 3 (16.7) | 3 (21.4) | 15 (20.3) | 0.122 |
| Appropriate antibiotic | 15 (65.2) | 18 (94.7) | 15 (83.3) | 11 (78.6) | 59 (79.7) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 8 (53.3) | 11 (61.1) | 10 (66.7) | 8 (72.7) | 37 (50.0) | 0.764 |
| Appropriate duration | 7 (46.7) | 7 (38.9) | 5 (33.3) | 3 (27.3) | 22 (29.7) | |
| Duration total | 15 (20.3) | 18 (24.3) | 15 (20.3) | 11 (14.9) | 59 (79.7) | |
|
| ||||||
| Inappropriate antibiotic | 16 (69.6) | 10 (52.6) | 10 (55.6) | 4 (28.6) | 40 (54.0) | 0.116 |
| Appropriate antibiotic | 7 (30.4) | 9 (47.4) | 8 (44.4) | 10 (71.4) | 34 (45.9) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 7 (100) | 4 (44.4) | 4 (50.0) | 8 (80.0) | 23 (31.1) | 0.056 |
| Appropriate duration | 0 (0.0) | 5 (55.6) | 4 (50.0) | 2 (20.0) | 11 (14.9) | |
| Duration total | 7 (9.4) | 9 (12.1) | 8 (10.8) | 10 (13.5) | 34 (45.9) | |
|
| ||||||
| Inappropriate antibiotic | 3 (13.0) | 2 (10.5) | 1 (5.6) | 0 (0.0) | 6 (8.1) | 0.618 |
| Appropriate antibiotic | 20 (87.0) | 17 (89.5) | 17 (94.4) | 14 (100.0) | 68 (91.9) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 2 (10.0) | 4 (23.5) | 7 (41.2) | 1 (7.1) | 14 (18.9) | 0.072 |
| Appropriate duration | 18 (90.0) | 13 (76.5) | 10 (58.8) | 13 (92.9) | 54 (73.0) | |
| Duration total | 20 (27.0) | 17 (23.0) | 17 (23.0) | 14 (18.9) | 68 (91.9) | |
|
| ||||||
| Inappropriate antibiotic | 17 (73.9) | 12 (63.2) | 17 (94.4) | 12 (85.7) | 58 (78.4) | 0.108 |
| Appropriate antibiotic | 6 (26.1) | 7 (36.8) | 1 (5.6) | 2 (14.3) | 16 (21.6) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 2 (33.3) | 2 (28.6) | 0 (0.0) | 0 (0.0) | 4 (5.4) | 1.000 |
| Appropriate duration | 4 (66.7) | 5 (71.4) | 1 (100) | 2 (100) | 12 (16.2) | |
| Duration total | 6 (8.1) | 7 (9.4) | 1 (1.3) | 2 (2.7) | 16 (21.6) | |
|
| ||||||
| Inappropriate antibiotic | 17 (73.9) | 14 (73.7) | 10 (55.6) | 7 (50.0) | 48 (64.9) | 0.319 |
| Appropriate antibiotic | 6 (26.1) | 5 (26.3) | 8 (44.4) | 7 (50.0) | 26 (35.1) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Appropriate duration | 6 (100) | 5 (100) | 8 (100) | 7 (100) | 26 (35.1) | |
| Duration total | 6 (8.1) | 5 (6.8) | 8 (10.8) | 7 (9.4) | 26 (35.1) | |
|
| ||||||
| Inappropriate antibiotic | 14 (60.9) | 6 (31.6) | 6 (33.3) | 5 (35.7) | 31 (41.9) | 0.172 |
| Appropriate antibiotic | 9 (39.1) | 13 (68.4) | 12 (66.7) | 9 (64.3) | 43 (58.1) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 2 (22.2) | 3 (23.1) | 5 (41.7) | 2 (22.2) | 12 (16.2) | 0.778 |
| Appropriate duration | 7 (77.8) | 10 (76.9) | 7 (58.3) | 7 (77.8) | 31 (41.9) | |
| Duration total | 9 (12.2) | 13 (17.5) | 12 (16.2) | 9 (12.2) | 43 (58.1) | |
|
| ||||||
| Inappropriate antibiotic | 19 (82.6) | 14 (73.7) | 10 (55.6) | 8 (57.1) | 51 (68.9) | 0.202 |
| Appropriate antibiotic | 4 (17.4) | 5 (26.3) | 8 (44.4) | 6 (42.9) | 23 (31.1) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 0 (0.0) | 0 (0.0) | 2 (25.0) | 0 (0.0) | 2 (2.7) | 0.407 |
| Appropriate duration | 4 (100) | 5 (100) | 6 (75.0) | 6 (100) | 21 (28.4) | |
| Duration total | 4 (5.4) | 5 (6.7) | 8 (10.8) | 6 (8.1) | 23 (31.1) | |
|
| ||||||
| Inappropriate antibiotic | 14 (60.9) | 8 (42.1) | 9 (50.0) | 5 (35.7) | 36 (48.6) | 0.449 |
| Appropriate antibiotic | 9 (39.1) | 11 (57.9) | 9 (50.0) | 9 (64.3) | 38 (51.4) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 1 (11.1) | 0 (0.0) | 0 (0.0) | 1 (11.1) | 2 (2.7) | 0.579 |
| Appropriate duration | 8 (88.9) | 11 (100) | 9 (100) | 8 (88.9) | 36 (48.6) | |
| Duration total | 9 (12.1) | 11 (14.9) | 9 (12.1) | 9 (12.1) | 38 (51.4) | |
|
| ||||||
| Inappropriate antibiotic | 7 (30.4) | 3 (15.8) | 3 (16.7) | 3 (21.4) | 16 (21.6) | 0.704 |
| Appropriate antibiotic | 16 (69.6) | 16 (84.2) | 15 (83.3) | 11 (78.6) | 58 (78.4) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 15 (93.8) | 15 (93.8) | 15 (100) | 11 (100) | 56 (75.7) | 1.000 |
| Appropriate duration | 1 (6.3) | 1 (6.3) | 0 (0.0) | 0 (0.0) | 2 (2.7) | |
| Duration total | 16 (21.6) | 16 (21.6) | 15 (20.3) | 11 (14.9) | 58 (78.4) | |
|
| ||||||
| Inappropriate antibiotic | 6 (26.1) | 7 (36.8) | 5 (27.8) | 1 (7.1) | 19 (25.7) | 0.239 |
| Appropriate antibiotic | 17 (73.9) | 12 (63.2) | 13 (72.2) | 13 (92.9) | 55 (74.3) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 3 (17.6) | 1 (8.3) | 3 (23.1) | 0 (0.0) | 7 (9.4) | 0.318 |
| Appropriate duration | 14 (82.4) | 11 (91.7) | 10 (76.9) | 13 (100) | 48 (64.9) | |
| Duration total | 17 (23.0) | 12 (16.2) | 13 (17.6) | 13 (17.6) | 55 (74.3) | |
|
| ||||||
| Inappropriate antibiotic | 9 (39.1) | 10 (52.6) | 4 (22.2) | 2 (14.3) | 25 (33.8) | 0.08 |
| Appropriate antibiotic | 14 (60.9) | 9 (47.4) | 14 (77.8) | 12 (85.7) | 49 (66.2) | |
| Antibiotic total | 23 (31.1) | 19 (25.7) | 18 (24.3) | 14 (18.9) | 74 (100) | |
| Inappropriate duration | 0 (0.0) | 1 (11.1) | 0 (0.0) | 0 (0.0) | 1 (1.3) | 0.184 |
| Appropriate duration | 14 (100) | 8 (88.9) | 14 (100) | 12 (100) | 48 (64.9) | |
| Duration total | 14 (18.9) | 9 (12.2) | 14 (18.9) | 12 (16.2) | 49 (66.2) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Innovations in Medical Education · Healthcare Systems and Technology
1. Introduction
Antibiotics are among the most commonly prescribed drugs for children.^1^ Reports have shown that more than 50% of all antibiotics are prescribed and dispensed inappropriately, and 50% of patients do not use antibiotics correctly.^23^ Unfortunately, the misuse and overuse of antibiotics in recent decades have led to the development of antibiotic resistance.^4^ Antimicrobial resistance (AMR) has emerged as a critical health concern and a global threat. Currently, there is a significant increase in morbidity and mortality associated with infections caused by multidrug-resistant microorganisms.^5^ Infections with these organisms result in approximately 700,000 deaths annually, including 200,000 deaths among children.^6^ Cassini et al. reported that one-third of the deaths related to infections caused by multidrug-resistant microorganisms in Europe occur in children.^7^
A cross-sectional study conducted in 2020 at the Royal Hospital, a tertiary care facility in Oman, assessed the knowledge, attitudes and practices of physicians across various experience levels and specialities regarding antibiotic use. The study revealed that the five primary factors contributing to AMR are inadequate handwashing, the widespread use of antibiotics, the prescribing of broad-spectrum antibiotics, a lack of effective narrow-spectrum antibiotics and inappropriate durations of antibiotic therapy.^8^
Identifying opportunities for antimicrobial stewardship programmes, addressing the knowledge gaps regarding antimicrobial usage among physicians and planning interventions that promote the judicious use of antimicrobials are crucial for reducing AMR worldwide.^89^ Paediatric residents represent the future of paediatric medicine, and providing them with proper training in antibiotic usage is essential to mitigate the risk of AMR. A study conducted at King Abdulaziz Medical City in Saudi Arabia compared the knowledge, attitudes and practices of antibiotic prescription among surgical and non-surgical residents. The study revealed that only 55% of all residents followed their local antibiotic guidelines.^10^ It was found that residents in non-surgical specialities were significantly more likely to follow established guidelines, undergo formal training and review patients' previous medical histories. Conversely, surgical residents exhibited higher rates of antibiotic prescriptions due to fear of infection spread.^10^
Another cross-sectional survey performed among paediatric residents at Nicklaus Children's Hospital and Children's National Medical Center, Columbia, revealed a significant deviation from clinical guidelines in prescribing antibiotics for children with acute sinusitis and community-acquired pneumonia. Conversely, the least deviation in antibiotic prescriptions at these two hospitals was recorded in children with otitis media and group A Streptococcal pharyngitis. Notably, only 57% of the residents completed the survey using an antibiogram.^11^ In the study, general paediatricians covering inpatients were identified as the most influential source of knowledge on antibiotics for paediatric residents. When asked to identify the reasons for their antibiotic prescriptions, 63% indicated that they were following the requests of senior residents and attending physicians, 21% cited precautionary measures due to concerns about the potential development of serious bacterial infections in the future, and 16% attributed their antibiotic prescriptions to parental pressure.^11^
The current study evaluates the antibiotic prescription knowledge and practices of paediatric residents affiliated with the Oman Medical Specialty Board (OMSB) for common paediatric infections. The aim is to identify issues and implement necessary interventions early to reduce AMR and improve patient care. The study also seeks to investigate the impact of the ‘infectious disease (ID)' rotation, the level of training, paediatric residents' antibiotic usage deviation from local guidelines and the factors influencing these practices. Accurate data on antibiotic prescriptions is crucial for further research and antimicrobial stewardship improvements.
2. Methods
This cross-sectional study was conducted among the paediatric residents of the OMSB in Muscat, Oman, from August 2023 to September 2023.
OMSB is an independent medical institution in Oman, accredited by the Council for Higher Medical Education. It is the sole institution in Oman responsible for higher medical education and setting standards for healthcare professions and practices in the country. The paediatric training programme spans four years, during which residents are required to achieve specific competencies by completing a well-structured clinical training programme and passing both written and clinical exams. The training period is divided into blocks of four weeks. As of 2023, there are 88 paediatric residents actively undergoing training at OMSB. The ID rotation is a four-week rotation that was previously an elective component of the paediatric residency programme. Since 2023, ID training has become mandatory for first-year (R1) paediatric residents. Therefore, only R1 residents participated in the rotation, while a few residents from the second year (R2) and fourth year (R4) opted to take it as an elective. Considering the population size of paediatric residents at OMSB during the study period, a 95% confidence level and a 5% margin of error indicate that the minimum accepted sample size should be 72. The total sample size gathered for this study was 74.
An anonymous, self-administered electronic questionnaire was developed using Google Forms based on several relevant international literature.^1011^ The questionnaire consisted of three parts: assessing demographics, knowledge and current practices [Supplementary Questionnaire]. The survey was open to all OMSB paediatric residents during the academic year (September 2022 to August 2023), excluding those who joined after the specified period or who did not consent to participate in the survey.
The demographics section includes age, gender, the institution from which they obtained their doctor of medicine (MD) degree, the year of residency and whether they participated in an ID rotation during their residency programme.
The second part was designed to assess the residents' knowledge regarding the indications for antibiotic prescribing. It included 12 clinical case scenarios of the most common infections in children, such as acute sinusitis, community-acquired pneumonia, streptococcal bacteraemia, acute meningitis, acute otitis media, osteomyelitis, exudative pharyngitis, cellulitis, pyelonephritis, neutropenic fever, septic shock and central line-associated bloodstream infections. Participants were asked to choose the proper antibiotic and specify the duration of treatment for each case. The third part of the questionnaire was created to evaluate the paediatric residents' practices in their daily antibiotic prescribing and to explore the factors influencing their prescribing behaviours. This part included three questions: a Likert scale question addressing seven factors that influence their prescriptions, a question regarding the rationale behind antibiotic prescribing and a question about the practice of seeking consultation from an ID consultant.
The questionnaire included closed-ended questions in a multiple-choice format that assessed the choices of antibiotics and short-answer questions that evaluated the duration of antibiotic use for each scenario.
Face validity was examined by six subject matter experts from the Child Health Department at Sultan Qaboos University Hospital (SQUH), Royal Hospital and Nizwa Hospital.
The electronic questionnaire was distributed individually to participants via their institutional e-mail addresses provided by OMSB. A follow-up e-mail was sent as a reminder three weeks after the initial distribution. Data collection was completed over the course of one month (16th August 2023–19th September 2023).
The data were entered into a Microsoft Excel spreadsheet (97-2003) and analysed using the Statistical Package for the Social Sciences (SPSS), Version 25.0 (IBM Corp., Armonk, New York, USA). Qualitative variables, including gender, MD degree-accrediting college and prior completion of an ID rotation, were described using absolute numbers (n) and relative frequencies (%). Quantitative variables, such as age and residency year, were summarised by their means and standard deviations. Fisher's exact test was used to determine the association between ID rotation completion and residents' decisions regarding antibiotic prescriptions. The chi-square test was used to evaluate the relationship between residency year and residents' antibiotic prescribing decisions. A stacked bar chart illustrated the deviations between local antibiotic guidelines (SQUH and Royal Hospital guidelines) and the antibiotic choices made by paediatric residents in each scenario. Bar charts were used to display the answers to the third part of the questionnaire, which addressed factors influencing antibiotic prescriptions, the rationale behind antibiotic prescribing and the practice of consulting an ID specialist. In analysing the ranking of the likelihood that specific factors influence antibiotic prescriptions, both very likely and likely options were combined into one category (overall: likely), while very unlikely and unlikely were grouped into another category (overall: unlikely). A P value ≤0.05 was considered statistically significant.
3. Results
During the study period, 74 out of 88 paediatric residents (84.0%) in the paediatric training programme agreed to participate and completed the questionnaire. Females comprised 82.4% of the participants, while males accounted for 17.6%. The distribution of participants across different years of the paediatric residency programme was as follows: 31.1% in R1 residents, 25.7% in R2 residents, 24.3% in the third year (R3) residents and 18.9% in R4 residents. Less than one-fourth of the residents (n = 21; 28.4%) completed ID rotation during their training. Among the 21 (28.4%) participants who completed the ID rotation, there were seven individuals from R1 residents, four from R2 residents and 10 from R4 residents. Thus, more than 50% of those who completed the rotation were in either R1 or R2 [Table 1].
Based on the local antibiotic guidelines at SQUH and the Royal Hospital, the highest adherence to the guidelines for antibiotic selection was observed in cases of acute sinusitis (n = 70; 94.6%), followed by acute meningitis (n = 68; 91.9%), community-acquired pneumonia (n = 59; 79.9%) and septic shock (n = 55; 74.3%). Conversely, the lowest adherence to the local guidelines was noted in the acute otitis media scenario (n = 16; 21.6%), followed by cellulitis (n = 23; 31.1%), osteomyelitis (n = 26; 35.1%), pyelonephritis (n = 38; 51.4%) and acute exudative pharyngitis (n = 43; 58.1%) [Supplementary Table 1 and Figure 1].
The adherence of the antibiotic choices to the local guidelines in the 12 infectious disease scenarios.
Table 2 demonstrates the association between ID rotation completion and paediatric residents' knowledge in choosing proper antibiotics and determining the duration of treatment for 12 ID scenarios in paediatric patients. Residents who participated in the ID rotation showed no significant difference in antibiotic prescription knowledge compared to those who did not across all 12 scenarios (P >0.05). Additionally, no significant differences were observed in antibiotic prescription knowledge among paediatric residents at different stages of their residency [Table 3].
Fig. 2 illustrates the responses of paediatric residents when asked to rank the likelihood that seven specific factors influence their choice of antibiotics in daily antibiotic prescriptions for paediatric patients. The top three highest ‘likely' factors were the patient's previous medical history (n = 63; 85.1%), mobile phone applications (n = 53; 71.6%) and medical references such as journals, articles and textbooks (n = 52; 70.3%). Conversely, the most ‘unlikely’ factor was the cost of the antibiotic (n = 56; 75.7%).
Factors influencing the paediatric residents in their daily antibiotic prescriptions.
The primary source of guidance used by residents was local guidelines (n = 59; 79.9%), followed by both international guidelines (n = 40; 54.1%) and senior consultants' decisions (n = 40; 54.1%).
Most residents indicated that they would seek ID consultations for patients with serious, complicated infections (n = 67; 90.5%), followed by those colonised or infected with multidrug-resistant microorganisms (n = 62; 83.3%) and patients with underlying complicated conditions (n = 58; 78.4%) [Fig. 3].
Seeking consultation from an infectious disease consultant.
4. Discussion
Paediatric residents are the first-line healthcare staff making decisions regarding antibiotic options for managing paediatric patients with various infections. This study is the first of its kind in Oman to evaluate antibiotic prescription knowledge among paediatric residents.
In Oman, general paediatricians manage common childhood infections and serve as a primary training site for paediatric residents during their general paediatric rotations. Paediatric residents acquire most of their knowledge and skills regarding common infections during these rotations. Collaborating with the ID team enhances their understanding of antibiotic resistance, the significance of local antibiograms and guidelines and the benefits of antimicrobial stewardship programmes. Co-working with the ID team during rotations improves their antibiotic-prescribing skills for common paediatric infections.
Based on the paediatric residents' choices of antibiotics and the duration of treatment in the chosen 12 ID scenarios, the results revealed that there are no significant differences in antibiotic prescription knowledge according to the residents' level of seniority. It is imperative to acknowledge the inherent educational progression within paediatric residency programmes. The early years of residency, specifically R1 and R2, are characterised by a steep learning curve where residents acquire fundamental clinical knowledge and skills under the supervision of consultants and senior colleagues. Consequently, variations in antibiotic prescriptions during these stages may be expected as part of the educational process. However, the main concern emerges when such knowledge gaps persist into the later years of the residency programme, mainly in R4. As residents reach the end of their residency programme, the expectation for proficiency in antibiotic prescribing practices becomes vital, as they will soon be working independently in healthcare settings. R4 represents a crucial stage in the paediatric residency programme, where residents are expected to display a professional and extensive understanding of appropriate prescribing skills. This includes adherence to local antibiotic guidelines and the judicious prescription of antimicrobial agents to achieve improved outcomes in the antimicrobial stewardship programme. Antibiotic prescription knowledge deficiencies and the failure to address this issue among R4 residents pose significant implications. Such deficiencies may compromise the quality of patient care and contribute to the rise of AMR. Furthermore, they may undermine the fundamental principles of patient safety and medical professionalism. Therefore, it is imperative to implement comprehensive educational interventions, mentorship initiatives and continuous assessments to bridge knowledge gaps and enhance excellence in antimicrobial stewardship among paediatric residents.
In discussing the results, the paediatric residents notably exhibited excellent performance in managing life-threatening infections, including acute meningitis and septic shock. An analysis of adherence to local antibiotic guidelines across 12 ID scenarios revealed that the highest compliance was observed in the cases of acute sinusitis and acute meningitis. Conversely, acute otitis media and cellulitis scenarios exhibited the greatest deviation from the recommended antibiotic guidelines. When comparing Shukla et al.'s results at Children's National Medical Center and Nicklaus Children's Hospital, the most significant deviation from antibiotic guidelines was observed in managing sinusitis and community-acquired pneumonia, while the lowest deviation occurred in the cases of otitis media and group A streptococcal pharyngitis.^11^ A study conducted in Egypt revealed that paediatric residents possessed a solid theoretical understanding of antibiotics; however, inappropriate prescribing practices remained widespread, with only 8.3% of prescriptions deemed appropriate.^12^ Similarly, a survey in China highlighted that, although paediatricians demonstrated excellent theoretical knowledge of antibiotics, a substantial proportion continued to misuse them in cases of upper respiratory tract infections.^13^ This misuse was attributed to factors such as diagnostic uncertainty and pressure from parents. These findings underscore the persistent gap between knowledge and practice in antibiotic prescribing, even among well-informed healthcare providers.
The concerning aspect of this result is the low adherence to antibiotic guidelines in managing acute otitis media, cellulitis and suppurative pharyngitis, as these are prevalent paediatric infections frequently encountered in clinical practice. Such discrepancies pose significant concerns for patient care, as inappropriate antibiotic selection may compromise treatment efficacy and contribute to AMR. Given the prevalence of these infections, it is crucial to address deviations to ensure optimal patient outcomes and maintain antimicrobial stewardship principles within paediatric healthcare management.
Factors influencing inappropriate antibiotic use commonly include non-adherence to guidelines, inadequate training and external pressures such as patient expectations.^13^ In exploring the factors that influence paediatric residents in their daily antibiotic prescriptions, the patient's previous medical history and mobile phone applications emerged as the most significant factors. In contrast, a study by Alowfi et al. at King Abdulaziz Medical City identified the use of medical references as the most influential factor.^10^ Additionally, the Shukla et al. study found that the most significant influence came from other general paediatric colleagues.^11^
Residents' willingness to use local antibiotic guidelines and evidence-based knowledge in their prescriptions was demonstrated by the fact that 59 (79.7%) of the paediatric residents indicated prescribing antibiotics according to local guidelines and that 52 (70.3%) of them cited medical references, including journals, articles and textbooks, as influential factors in their antibiotic prescriptions. Furthermore, paediatric residents showed a strong understanding of when to seek assistance from an ID consultant regarding antibiotic prescriptions in their daily practice.
Addressing antibiotic prescription issues among paediatric residents necessitate a primary focus on general paediatric rotations. Throughout the four-year residency programme, continuous education on managing ID and antibiotic prescriptions in paediatrics should be delivered through ongoing workshops and teaching sessions. The objectives for the general paediatric rotation should encompass both general paediatric ID topics and self-learning case-module development. ID rotations enhance their knowledge and improve their antibiotic-prescribing skills. Madigan et al. reported highly positive feedback from pediatric residents following the introduction of a 10-minute ‘Antibiotic of the Month’ session within a continuous education programme. The initiative significantly improved residents' knowledge and comfort with antimicrobial prescribing, demonstrating that brief, regular educational interventions can enhance prescribing practices more effectively than infrequent, longer sessions.^14^
Although the overall results revealed that the ID rotation did not enhance paediatric residents' knowledge of antibiotic prescription, this outcome can be attributed to the relatively small number of residents who participated in the ID rotation. Additionally, the rotation's short duration of only four weeks may have limited its effectiveness. Moreover, a four-week ID rotation could be further compromised by other academic activities and commitments, which may reduce clinical exposure and ID-related learning during this period. It is worth mentioning that the ID rotation was previously an elective component of the paediatric residency programme; however, since 2022, it has become a mandatory placement for all residents during their R1 training.
Paediatric residents should be aware of and consider the local antibiotic guidelines as early as their R1. Various strategies can be implemented in this area, including the use of an antibiotic reference card, which is used in different international hospitals. This card provides recommended antibiotic choices for the most common ID in paediatrics and can be conveniently carried alongside their ID card during daily practice. Additionally, from the outset of their residency, residents should receive updated antibiogram charts whenever they become available.
The main limitation of this study was the small population size (N = 88), which resulted in a limited sample size (N = 74). However, the significance of the findings should not be underestimated, as the survey responses accounted for 84% of the entire population. Additionally, the non-homogeneity of the groups based on years of residency is noteworthy; R1, R2 and R4 completed the ID rotation, while R3 did not. Moreover, there is a potential for participation bias, as participants in survey-based studies may attempt to provide answers they believe the investigator desires. Additionally, recall bias, which is inherent in survey-based research, should be considered as another limitation. Further studies should be conducted to validate these results and explore additional areas for improvement.
5. Conclusion
This study assessed antibiotic prescriptions made by paediatric residents at the OMSB and uncovered significant findings. The main finding is that there were no substantial differences in paediatric residents' understanding of antibiotic prescriptions across different years of the residency programme. Notable deviations from local antibiotic guidelines were observed in managing acute otitis media, cellulitis and pharyngitis, whereas the strictest adherence to these guidelines was noted in managing acute sinusitis. Residents showed competent clinical judgement by consulting ID consultants as needed in their daily practice. Comprehensive interventions are required within the residency programme to enhance Oman's antimicrobial stewardship efforts and improve the paediatric residency curriculum. Continuous education and quality improvement initiatives are deemed essential.
Authors' Contribution
Shaima Alshukaili: Investigation, Data Curation, Formal Analysis, Writing – Original Draft. Hussain Al-Saffar: Conceptualization, Methodology, Writing – Review & Editing. Hatem Al-Rawahi: Conceptualization, Methodology, Writing – Review & Editing. Laila Al Yazidi: Conceptualization, Methodology, Formal Analysis,. Supervision, Writing – Review & Editing.
Acknowledgements
The authors would like to acknowledge all the paediatric residents of OMSB who completed the questionnaire.
Ethics Statement
The survey was conducted with anonymous participation, and paediatric residents were assigned numerical codes during data analysis to ensure confidentiality. Informed consent was obtained from all subjects. The purpose of the study and the right to withdraw at any time were clearly explained at the beginning of the questionnaire. Only the study investigator had access to the study data. The study received ethical approval from the Research and Ethics Committee at OMSB (REC/02/2023) in July 2023.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received for this study.
Data Availablility
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chai G Governale L Mc Mahon AW Trinidad JP Staffa J Murphy D. Trends of outpatient prescription drug utilization in US children, 2002–2010. Pediatrics 2012; 130:23–31. https://doi.org/10.1542/peds.2011-2879.10.1542/peds.2011-287922711728 · doi ↗ · pubmed ↗
- 2Ofori-Asenso R Agyeman AA. Irrational use of medicines—a summary of key concepts. Pharmacy (Basel) 2016; 4:35. https://doi.org/10.3390/pharmacy 4040035.10.3390/pharmacy 404003528970408 PMC 5419375 · doi ↗ · pubmed ↗
- 3Atif M Ashgar S Mushtaq I Malik I Amin A Babar ZUD. What drives inappropriate use of antibiotics? A mixed methods study from Bahawalpur, Pakistan. Infect Drug Resist 2019; 12:687–99. https://doi.org/10.2147/IDR.S 189114.10.2147/IDR.S 18911430988635 PMC 6440533 · doi ↗ · pubmed ↗
- 4Sengupta S Chattopadhyay MK Grossart HP. The multifaceted roles of antibiotics and antibiotic resistance in nature. Front Microbiol 2013; 4:47. https://doi.org/10.3389/fmicb.2013.00047.10.3389/fmicb.2013.0004723487476 PMC 3594987 · doi ↗ · pubmed ↗
- 5Romandini A Pani A Schenardi PA Pattarino GAC De Giacomo C Scaglione F. Antibiotic resistance in pediatric infections: Global emerging threats, predicting the near future. Antibiotics (Basel) 2021; 10:393. https://doi.org/10.3390/antibiotics 10040393.10.3390/antibiotics 1004039333917430 PMC 8067449 · doi ↗ · pubmed ↗
- 6Interagency Coordination Group on Antimicrobial Resistance. No time to wait: Securing the future from drug-resistant infections. Interagency Coordination Group on Antimicrobial Resistance; 2019.
- 7Cassini AHögberg LD Plachouras D Quattrocchi A Hoxha A Simonsen GS. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect Dis 2019; 19:56–66. https://doi.org/10.1016/S 1473-3099(18)30605-4.10.1016/S 1473-3099(18)30605-430409683 PMC 6300481 · doi ↗ · pubmed ↗
- 8Rahbi FA Salmi IA Khamis F Balushi ZA Pandak N Petersen E. Physicians' attitudes, knowledge, and practices regarding antibiotic prescriptions. J Glob Antimicrob Resist 2023; 32:58–65. https://doi.org/10.1016/j.jgar.2022.12.005.10.1016/j.jgar.2022.12.00536584969 · doi ↗ · pubmed ↗