Clinical Predictors of Inherited Breast Cancer at a Comprehensive Cancer Centre in Oman: Is it time for universal germline genetic testing?
Reem Abdulrahim, Hasan Al-Sayegh, Sara Al-Kiyumi, Ilse Crous, Khalid Al Baimani, Adil Aljarrah, Chantel Van Wyk, Abeer Alsayegh

TL;DR
This study examines whether universal genetic testing for inherited breast cancer is needed in Oman, as current guidelines may miss many cases.
Contribution
The study evaluates the effectiveness of NCCN guidelines in an Omani population and suggests universal testing may be more appropriate.
Findings
Age was not a reliable predictor of positive genetic test results for inherited breast cancer.
NCCN guidelines may lead to underdiagnosis of hereditary breast cancer in Omani patients.
Universal germline genetic testing could be more effective for Omani breast cancer patients.
Abstract
This study aimed to explore the clinical, histopathological and demographic characteristics of female Omani breast cancer (BC) patients to identify possible predictors of a positive test result. Additionally, it aimed to evaluate the applicability of the National Comprehensive Cancer Network (NCCN) guidelines for germline genetic testing in risk assessment. This study was conducted at the Sultan Qaboos Comprehensive Cancer Centre, Oman, between September 2021 and September 2022. The variables examined included age, disease stage, presence of metastasis at diagnosis, hormone receptor status, human epidermal growth factor receptor 2 status, histopathological type, Ki-67 levels, family history of cancer (presence/absence) and the applicability of NCCN guidelines. Data were retrieved and summarised using electronic patient files and family pedigrees collected by geneticists and genetic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
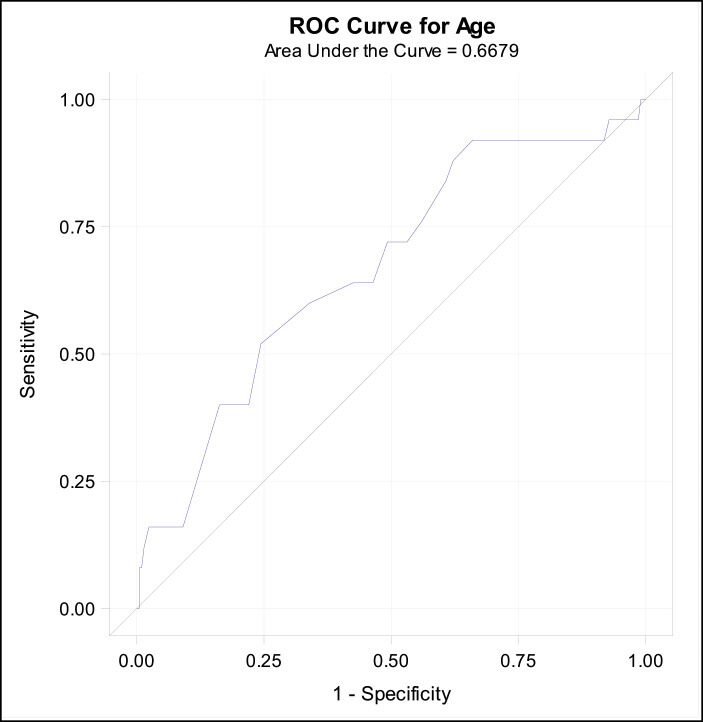 Fig. 1
Fig. 1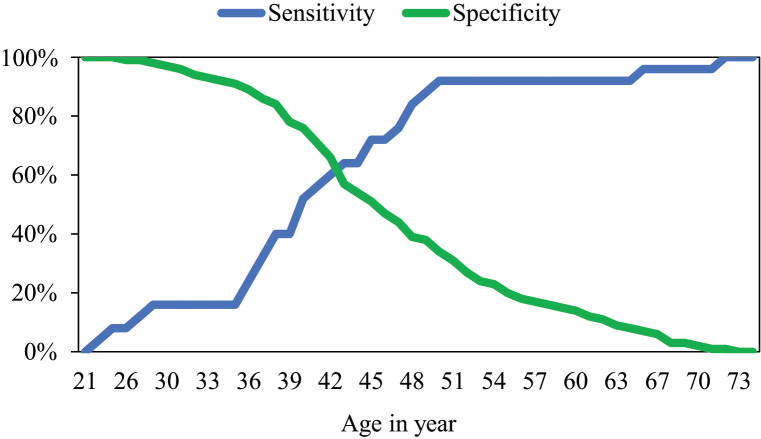 Fig. 2
Fig. 2| Total | Tested negative (n = 209) | Tested positive (n = 25) | ||
|---|---|---|---|---|
| n (%) or Median (IQR) | n (%) or Median (IQR) | n (%) or Median (IQR) | ||
|
| 45 (21–74) | 209 (89.3) | 25 (10.7) | 0.006 |
| 46 (21–74) | 40 (23–72) | |||
|
| 30 (1–95) | 168 (89.4) | 20 (10.6) | 0.29 |
| 32.5 (1–95) | 27.5 (10–95) | |||
|
| 197 (89.5) | 23 (10.5) | 0.98 | |
| None | 57 (25.9) | 52 (26.4) | 5 (21.7) | |
| First degree | 78 (35.5) | 68 (34.5) | 10 (43.5) | |
| Second or higher degree | 85 (38.6) | 77 (39.1) | 8 (34.8) | |
|
| 197 (89.5) | 23 (10.5) | 0.8 | |
| Positive | 163 (74.1) | 145 (73.6) | 18 (78.3) | |
| Negative | 57 (25.9) | 52 (26.4) | 5 (21.7) | |
|
| 209 (89.3) | 25 (10.7) | 0.55 | |
| Unilateral | 227 (97) | 203 (97.1) | 24 (96) | |
| Bilateral | 7 (3) | 6 (2.9) | 1 (4) | |
|
| 209 (89.3) | 25 (10.7) | 0.16 | |
| Yes | 7 (3) | 5 (2.4) | 2 (8) | |
| No | 227 (97) | 204 (97.6) | 23 (92) | |
|
| 209 (89.3) | 25 (10.7) | 0.61 | |
| Yes | 52 (22.2) | 47 (22.5) | 4 (16) | |
| No | 183 (78.2) | 162 (77.5) | 21 (84) | |
|
| 183 (90.1) | 20 (9.9) | 0.91 | |
| I | 18 (8.9) | 17 (9.3) | 1 (5) | |
| II | 71 (35) | 64 (35) | 7 (35) | |
| III | 62 (30.5) | 54 (29.5) | 8 (40) | |
| IV | 52 (22.2) | 48 (26.2) | 4 (20) | |
|
| 205 (89.1) | 25 (10.9) | 0.31 | |
| Negative | 179 (77.8) | 157 (76.6) | 22 (88) | |
| Positive | 51 (22.2) | 48 (23.4) | 3 (12) | |
|
| 208 (89.3) | 25 (10.7) | ||
| Yes | 38 (16.31) | 35 (16.8) | 3 (12) | 0.78 |
| No | 195 (83.69) | 173 (83.2) | 22 (88) | |
|
| 181 (89.2) | 22 (10.8) | 0.52 | |
| IDC | 186 (91.6) | 166 (91.7) | 20 (90.9) | |
| ILC | 12 (5.9) | 11 (6.1) | 1 (4.5) | |
| Mixed | 2 (1) | 2 (1.1) | 0 (0.0) | |
| Other | 3 (1.5) | 2 (1.1) | 1 (4.5) | |
|
| 209 (89.3) | 25 (10.7) | 0.48 | |
| Yes | 210 (89.7) | 186 (89) | 24 (96) | |
| No | 24 (10.3) | 23 (11) | 1 (4) | |
|
| ||
|---|---|---|
|
| 0.94 (0.9–0.99) | 0.01 |
|
| 1.01 (0.99–1.03) | 0.22 |
|
| 0.69 | |
| First degree | 1.53 (0.49–4.75) | 0.46 |
| Second or higher degree | 1.08 (0.33–3.49) | 0.9 |
| None | 1 (Reference) | |
|
| ||
| Positive | 1.29 (0.46–3.65) | 0.63 |
| Negative | 1 (Reference) | |
|
| ||
| Bilateral | 1.41 (0.16–12.21) | 0.75 |
| Unilateral | 1 (Reference) | |
|
| ||
| Yes | 3.55 (0.65–19.34) | 0.14 |
| No | 1 (Reference) | |
|
| ||
| Yes | 0.66 (0.21–2.01) | 0.46 |
| No | 1 (Reference) | |
|
| 0.74 | |
| II | 1.86 (0.21–16.16) | 0.57 |
| III | 2.52 (0.29–21.6) | 0.4 |
| IV | 1.42 (0.15–13.58) | 0.76 |
| I | 1 (Reference) | |
|
| ||
| Negative | 2.24 (0.64–7.82) | 0.21 |
| Positive | 1 (Reference) | |
|
| ||
| Yes | 0.67 (0.19–2.38) | 0.54 |
| No | 1 (Reference) | |
|
| ||
| ILC/Mixed/Other | 1.11 (0.24–5.2) | 0.9 |
| IDC | 1 (Reference) | |
|
| ||
| Yes | 2.84 (0.37–21.99) | 0.32 |
| No | 1 (Reference) |
| Positive | Negative | |||
|---|---|---|---|---|
| Age | Sensitivity | Specificity | predictive value | predictive value |
| 26 | 8% | 99% | 50% | 90% |
| 30 | 16% | 97% | 40% | 91% |
| 35 | 16% | 91% | 17% | 90% |
| 40 | 52% | 76% | 20% | 93% |
| 45 | 72% | 51% | 15% | 94% |
| 50 | 92% | 34% | 14% | 97% |
| 55 | 92% | 20% | 12% | 95% |
| 60 | 92% | 14% | 11% | 94% |
| 65 | 96% | 7% | 11% | 94% |
| 70 | 96% | 2% | 11% | 83% |
| 74 | 100% | 0% | 11% | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Genomics and Rare Diseases · Genomic variations and chromosomal abnormalities
1. Introduction
Breast cancer (BC) is the most common malignancy among women and has the highest disease-specific mortality rate of all cancer types.^1^ Approximately 5–10% of BC cases are hereditary, with 20% of these attributed to mutations in the breast cancer gene 1 and 2 (BRCA1 and BRCA2).^2^ The National Comprehensive Cancer Network (NCCN) guidelines provide widely acceptable genetic testing criteria to identify high-risk patients who may benefit from such testing. These criteria consider factors such as young age (≤50), gender, presence of bilateral breast disease, hormonal receptor and human epidermal growth factor receptor 2 (HER2) status, histological type, family history of cancer and relevant therapeutic indications.^3^ Interestingly, the prevalence of these indicators varies among different populations, which can be attributed to differences in risk factor distribution, such as pregnancy and breastfeeding practices, usage of hormone replacement therapy and the ages of menarche and menopause.^4^ Triple-negative breast cancer (TNBC) is associated with poor outcomes and is found in more than 85% of BC cases characterised by homologous recombination deficiency due to pathogenic variants in BRCA1 and BRCA2, as well as other associated genes, including PALB2, RAD51C and BARD1.^5^
Globally, the greatest BC burden is reported in individuals aged 50 years and older.^6^ In 2020, an analysis of Oman's cancer registry data showed a rising trend of BC among the younger population. Although the highest age-specific incidence rates were observed in the 65–70 age group (100.7/100,000), the incidence rates were comparable in the 50–54 age group (83.8/100,000) and in the 45–49 age group (82.1/100,000), with more than 67% of cases occurring in individuals under the age of 50.^7^ The younger age of presentation in the Gulf Cooperation Council (GCC) countries is attributed to the obesity epidemic, which is a consequence of sedentary lifestyles and unhealthy dietary habits.^89^
Furthermore, some studies postulated the possibility of inherent differences in the genetic makeup of GCC populations; however, this remains to be elaborated on in future studies.^10^ Inherited BC tends to occur in younger age groups compared to non-inherited BC, making it a useful factor for risk assessment.^11^ This study aims to identify the prevalence of these important risk assessment factors among Omani women with BC and to evaluate the effectiveness of NCCN guidelines as a screening tool for patients with pathogenic (P) or likely pathogenic (LP) variants in BC-associated genes, as classified by the American College of Medical Genetics and Genomics and the Association for Molecular Pathology variant curation guidelines.
2. Methods
This retrospective study was conducted at the Sultan Qaboos Comprehensive Cancer Centre, Oman, between September 2021 and September 2022. It included all BC patients referred for genetic evaluation based on the oncologist's decision, primarily due to factors such as young age, immunohistochemistry status for HER2, family history of cancer and therapeutic implications. Patients who underwent germline molecular genetic testing, with results available at the time of the study, were enrolled. Basic clinical characteristics were described, including age at diagnosis, presence of bilateral disease, history of another primary cancer, disease stage, Ki-67 levels, histopathological type, tissue receptor status, presence or absence of a family history of cancer and applicability of NCCN guideline criteria. Data were retrieved from electronic patient files.
The 127-gene Full Comprehensive Cancer Panel from Fulgent Genetics Laboratories, USA, was used on patients' blood samples. This panel includes sequencing, deletion and duplication analysis, with a coverage of 99% at 50x. Results may be classified as positive (P or LP variants), negative (no variant identified) or inconclusive (a variant of uncertain significance [VUS]).
In the descriptive analysis, this study reported the median and range for continuous variables, as well as the frequency and percentages for categorical variables. The Wilcoxon rank-sum test was employed to compare continuous variables between groups with positive and negative genetic test results. The Fisher exact test was used to compare categorical variables, while the Cochran-Armitage trend test was applied to assess ordinal variables (affected relatives and stage) between the two groups. Logistic regression predictive models were used to examine the association of various predictive factors with positive genetic testing outcomes. Odds ratios (OR) and their 95% confidence intervals (CI) were reported. A P value of 0.05 or lower was considered statistically significant. The receiver operating characteristic (ROC) curve was used to examine the ability of age to discriminate between positive and negative genetic testing results, with the area under the curve (AUC) reported. Using ROC analysis, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for various cutoff age values in predicting positive genetic testing outcomes. All analyses were performed using Statistical Analysis System software, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
3. Results
A total of 234 women diagnosed with BC received genetic testing and were included in the study. The median age at diagnosis was 45 years (range: 21–74 years). Among the participants, 163 (74%) had a positive family history of cancer, and in 78 (36%) cases, the affected relative was a first-degree relative. Regarding receptor status, 179 (78%) patients were HER2 negative, 38 (16%) were classified as TNBC and 51 (22%) patients presented with metastasis at the time of diagnosis [Table 1].
The overwhelming majority of patients had unilateral lesions and did not have other primary tumours, with 227 (97%) for both variables. Most patients were at Stages II and III of the disease, with 71 (35%) and 62 (31%), respectively, while 52 (26%) were at Stage IV. Regarding histopathology, most of the patients (n = 186, 92%) were diagnosed with invasive ductal carcinoma, while 12 (6%) were diagnosed with invasive lobular carcinoma. Of the 234 patients, 25 (11%) tested positive for P or LP variants, 27 (11%) tested negative, 12 (5%) were carriers of P/LP variants associated with autosomal recessive (AR) conditions and 170 (73%) had VUSs. Except for age, there were no statistically significant differences in baseline characteristics between the positive and negative genetic test groups.
The prevalence of P variants was as follows*: BRCA2* in 11 patients (2.9%), PALB2 and BRIP1 in three patients each (1.3%), TP53 in two patients (0.9%) and NBN in one patient (0.4%). Three P variants were considered positive despite the lack of a clear association with BC due to repeated clinical observations suggesting a potential link that is currently under study. Additionally, these findings are important secondary results associated with well-characterised inherited cancer syndromes, which have significant implications for the surveillance of cancers beyond BC. This includes one P variant in the FH gene found in one patient (0.4%) and two P variants in the SDHB gene found in two patients (0.9%). Furthermore, three of the 25 patients carried a P/LP variant in AR genes, in addition to the autosomal dominant P/LP variants, which included the RECQL4, ERCC5 and MUTYH genes.
In the logistic regression predictive models, only age emerged as a significant predictor of positive genetic testing outcomes. The odds of obtaining a positive genetic test result decreased by 5% for each additional year of age (OR = 0.94, 95% CI = 0.91–0.99, P = 0.01) [Table 2]. Age showed low discrimination between positive and negative genetic testing results (AUC = 0.67, 95% CI = 0.55–0.78) [Table 3; Fig. 1, Fig. 2]. The analysis indicated that a cutoff age of 50 years for genetic testing would yield 92% sensitivity, 34% specificity, 14% PPV and 97% NPV. This implies that if all BC patients aged ≤50 years old are tested, one can expect to identify 92% of the positive cases; however, this comes with low specificity (34%), meaning that 66% of the negative population will also be tested, and only 14% of those tested will have positive genetic results. NCCN guidelines were applicable to 90% of the patients, while around 10% did not meet the criteria. To optimise patient testing, the intention was to utilise specific patient criteria to detect predictors of positive test results. Younger age was the only predictor significantly associated with an increased likelihood of a positive test result.
The receiver operating characteristic curve for age: discriminating between positive and negative genetic test results.ROC = receiver operating characteristic.
Sensitivity and specificity for various age cut-off points predicting positive genetic test using the receiver operating characteristic curve analysis.
All the BRCA-positive patients were HER2-negative; however, none were classified as TNBC. Only three positive patients were TNBC, including P/LP variants in the FH, TP53 and BRIP1 genes.
4. Discussion
This is the first Omani study to explore the clinical, histopathological and demographic characteristics of female Omani BC patients to identify possible predictors of a positive genetic test. Analysing the patients' characteristics, the median age was found to be 45 years, which aligns with evidence supporting that BC occurs at a younger age in GCC countries compared to developed nations.^12^ Patients who tested positive for genetic markers were significantly younger than those who tested negative (P = 0.006). However, age was determined to be a poor predictor of variability in test results, as indicated by an overall area under the ROC curve of 0.67. Besides age, regression analysis did not identify any association between the predictive variables and the outcome of positive genetic test results. The percentages of patients with and without a reported family history of cancer were comparable between the positive and negative groups. In a further step to delineate the association between consanguinity of the proband and affected family members (first-degree relatives vs second-degree or farther) and positive test results, it was found that the degree of consanguinity did not seem to explain the variability in test outcomes. This may be due to the presence of low-penetrance genes. Additionally, studies have shown that approximately 70% of familial clustering of BC remains unexplained.^13^
Among Omani patients, TNBC was found to have comparable percentages in both positive and negative test results. This observation can be explained by the fact that only 10–15% of TNBC cases are associated with BRCA1/BRCA2 germline P variants.^14^ Similarly, HER2-negative patients seemed to be equally represented in both groups. This finding aligns with recent evidence from a multicentre study reporting the comparable prevalence of germline BRCA P variants in both HER2-positive and HER2-negative BC groups.^15^ Regarding FH and SDHB P variants, these were considered positive results given their importance in other cancer surveillance and in cascade testing for affected families. Furthermore, literature has begun to suggest a possible association between FH and P variants and an increased risk of BC.^161718^ However, this association may require further validation in future studies.
In this cohort of 234 Omani patients with BC, the genetic test yield was found to be 11%, which is comparable to international data.^19^ The applicability of NCCN guidelines on patients did not seem to improve genetic test yield, as reported in recent years.^2021^
In this study, around 73% of the patients received VUS results. This percentage is higher than that reported in other studies.^2223^ This increase can be attributed to the use of an expanded comprehensive cancer panel approach. However, this method can be quite challenging in a clinical setting, as these results are often considered unactionable for disease management, surveillance and risk reduction interventions, potentially leading to increased levels of patient anxiety.^24^ Despite these challenges, many authors advocate for expanded testing to include additional genes, given the importance of some secondary findings in non-BC-associated genes that may be overlooked when using a BC-focused panel.^252627^ The SDHB gene is one of the most important genes associated with hereditary pheochromocytoma/paraganglioma, which tends to grow substantially in a subclinical manner, making it difficult to identify vague symptoms of increased catecholamine secretion. Consequently, early detection is crucial for improved management and better prognosis.^28^ Furthermore, the rates of consanguinity in the Omani population have been found to be as high as 49%.^29^ This underscores the importance of identifying carrier status for heterozygous P/LP variants, which can be very useful for families considering their reproductive options.
Recently, universal testing for all BC patients has been advocated, regardless of family history, particularly for BRCA1/2 and PALB2 mutations.^3031^ The detection of familial P variants is crucial for cancer prevention endeavours and can complement population-based screening programmes.^3233^ Some authors have suggested a hybrid approach that involves testing all patients younger than 60–65 years while applying NCCN guidelines for older patients.^34^ However, this strategy should be implemented with careful consideration of cost-effectiveness, especially in the context of HER2-negative disease.^35^ Fortunately, studies from the United States and the United Kingdom have indicated that a universal testing policy can be cost-effective when considering quality-adjusted life years.^36^
This is a single-centre study that includes a relatively limited number of participants, which may impact the generalisability of the results. Consequently, the study results may not be enough to inform clinical practice. Additionally, relying on a patient's knowledge of their family cancer history may be prone to inaccuracies, potentially leading to erroneous conclusions about the possible association between a family history of cancer and the identification of positive genetic test results. Therefore, future studies should focus on recruiting participants in a way that is representative of the BC patient population. Furthermore, collaboration among different healthcare facilities is necessary to link various family members in order to identify family history precisely, following ethical clearance from the relevant authorities and without breaching patient confidentiality.
5. Conclusion
This study provides preliminary evidence that available testing criteria such as NCCN guidelines can be weak predictors for risk assessment in Omani women with BC. Moreover, despite the significant association between younger age and identifying a positive germline genetic test result, age appears to be a poor screening tool for differentiation between patients with positive and negative germline test results, as indicated by a small area under the ROC curve. This finding may support the case for universal germline testing for all patients with BC. Further studies are needed to compare the effectiveness of comprehensive cancer panels vs focused BC panels to reduce the likelihood of VUSs, which can be challenging to interpret and may lead to indecisiveness, patient anxiety and confusion.
Authors' Contribution
Reem Abdulrahim: Conceptualization, Methodology, Investigation, Formal Analysis, Writing - Original Draft, Writing - Review & Editing. Hasan Al-Sayegh: Visualization, Formal Analysis, Writing - Original Draft, Writing – review & editing. Sara Al-Kiyumi: Investigation, Resources. Ilse Crouse: Investigation, Resources, Writing - Original Draft, Writing – Review & Editing. Khalid Albaimani: Writing - Review & Editing. Adil Aljarrah: Writing - Review & Editing. Chantel Van Wyk: Investigation, Writing - Original Draft, Writing - Review & Editing. Abeer Alsayegh: Conceptualization, Methodology, Writing - Review & Editing.
Ethics Statement
Data were retrieved from electronic patient files after participants signed a research consent form. The genetic test consent form, which is routinely signed by all patients, includes a section for research consent. Only patients who consented to participate in future research projects were included in the study. The study was approved by the ethical committees at the Sultan Qaboos Comprehensive Cancer Care and Research Centre, Muscat, Oman (CCCRC-81-2023).
Conflict of Interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smolarz B Zadrozna Nowak A Romanowicz H. Breast cancer—epidemiology, classification, pathogenesis and treatment (review of literature). Cancers 2022; 14.35626173 10.3390/cancers 14102569 PMC 9139759 · doi ↗ · pubmed ↗
- 2Sokolova A Johnstone KJ Mc Cart Reed AE Simpson PT Lakhani SR. Hereditary breast cancer: Syndromes, tumour pathology and molecular testing. Histopathology 2023; 82:70–82.10.1111/his.1480836468211 PMC 10953374 · doi ↗ · pubmed ↗
- 3Daly MB Pal T Maxwell KN Churpek J Kohlmann W Al Hilli Z. NCCN guidelines®insights: Genetic/familial high-risk assessment: Breast, ovarian, and pancreatic, version 2.2024: Featured updates to the NCCN guidelines. J Natl Compr Canc Netw 2023; 21:1000–10.10.6004/jnccn.2023.005137856201 · doi ↗ · pubmed ↗
- 4Łukasiewicz S Czeczelewski M Forma A Baj J Sitarz R Stanisławek A. Breast cancer-epidemiology, risk factors, classification, prognostic markers, and current treatment strategies–an updated review. Cancers (Basel) 2021; 13. https://pubmed.ncbi.nlm.nih.gov/34503097/.34503097 10.3390/cancers 13174287 PMC 8428369 · doi ↗ · pubmed ↗
- 5Derakhshan F Reis-Filho JS. Pathogenesis of triple-negative breast cancer. Annu Rev Pathol Mech Dis 2022; 17:181–204. https://doi.org/10.1146/annurev-pathol-042420-.10.1146/annurev-pathol-042420-PMC 923150735073169 · doi ↗ · pubmed ↗
- 6Arnold M Morgan E Rumgay H Mafra A Singh D Laversanne M. Current and future burden of breast cancer: Global statistics for 2020 and 2040. The Breast 2022; 66:15–23.10.1016/j.breast.2022.08.01036084384 PMC 9465273 · doi ↗ · pubmed ↗
- 7Al- N Nabil L Salim AS Reviewers AW Al-Raisi S Al-Bahrani B. Cancer incidence in Oman 2020. 2023. www.moh.gov.om.
- 8Alduraidi H Tarazi A Theeb L Al Kasaji M. Knowledge, attitudes, and practices toward breast cancer and breast cancer screening among Arab females in the Middle East: A literature review. Public Health Nurs 2024. https://onlinelibrary.wiley.com/doi/full/10.1111/phn.13447.10.1111/phn.1344739415538 · doi ↗ · pubmed ↗