Bullous Diabeticorum
Maisam Alsalmani, Ayida Al Khalili, Maiya Al Bahri

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
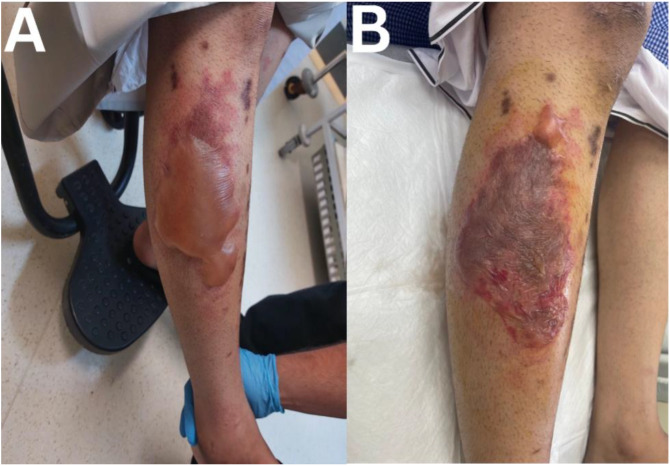 Figure 1
Figure 1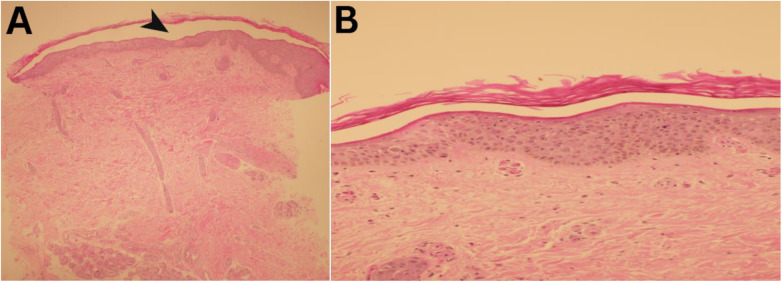 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Skin Diseases and Diabetes · Nail Diseases and Treatments
A 25-year-old male patient known for poorly controlled type 1 diabetes mellitus, presented with 1-day history of acute onset asymptomatic blister on right leg. It was not preceded by trauma, an insect bite or application of any products. There was no recent introduction of new medications and he had no history of fever or constitutional symptoms. He denied any similar previous eruptions. Skin examination revealed tense bullae of approximately 8 × 15 cm on his right lateral leg with mild rim of erythema [Fig. 1]. There were no oedema, mucosal involvement or lymphadenopathy and Nikolsky sign was negative. Differential diagnoses included bullous diabeticorum, exaggerated bullous insect bite reaction, bullous fixed drug reaction and immunobullous disorders. His glycated haemoglobin ranged between 14–15%. Skin biopsy revealed cell poor subcorneal blister with no inflammatory or acantholytic cells [Fig. 2]. Immunofluorescence for IgA, IgG, IgM and C3 were negative from perilesional skin. Fluid swab culture grew light growth of staphylococcus argenteus. Subsequently, he was diagnosed with bullous diabeticorum and managed with optimal wound care and prophylactic systemic antibiotic to prevent bacterial superinfection given large area of involvement. He healed completely in 10 weeks with post inflammatory hyperpigmentation.
1. Comment
Bullous diabeticourm is a rare cutaneous complication of diabetes mellitus. It is characterised by the abrupt spontaneous onset of asymptomatic non inflammatory bullous eruption.^1^ It preferentially occurs on distal acral areas, lower extremities followed by upper extremities and rarely the trunk.^2^ Its aetiology is not fully known but multifactorial theories and hypotheses have been proposed. Microangiopathy, sympathetic autonomic denervation, increased venous pressure, diabetic neuropathy, ultraviolet exposure and trauma are some suggested mechanisms for the formation of diabetic bullae.^12345^ There is risk of recurrence at the same or different sites.^5^ It could be complicated by secondary bacterial infection and rarely osteomyelitis.^15^
Differential diagnoses include autoimmune blistering disorders (e.g., bullous pemphigoid, porphyria cutanea tarda, pseudoporphyria) and friction or oedema blister.^5^ Diagnosis is mainly clinical; however, other autoimmune blistering disorders could be excluded with direct immunofluorescence. Culture from the fluid is advised if secondary bacterial infection is suspected.^25^ Diabetic bulla affects mainly diabetic patients with long standing disease with complications. Although it is often linked to poor glycaemic control, the association between its occurrence and glycaemic control seems inconsistent.^2^ In the United States, its incidence is 0.5% of diabetic population and males are twice as affected as females.^3^
Supportive therapy is the mainstay of treatment as it is a self-limiting condition. Aspiration of the fluid to prevent accidental deroofing and wound care are suggested in large bullae. Resolution generally occurs with 2–6 weeks.^12^ In the current case, diagnosis was supported with history and clinical morphology. Pathology ruled out other differential diagnoses and his swab culture grew light growth of Staphylococcus argenteus, which was thought to be due to contamination rather than infection as no clinical or pathological features were suggestive of infection.
Authors' Contribution
Maisam Al Salmani: Investigation, Visualization, Writing - Original Draft. Ayida Al Khalili: Project administration, Supervision, Writing - Review & Editing. Maya Al Bahri: Investigation, Resources, Writing - Review & Editing.
Ethics Statement
Patient consent was obtained for publication purposes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Paul AJ Louis RS Julien AAI Florvil F Blaise W. Bullosis Diabeticorum in a Morbidly Obese Woman in Haiti. Arch Clin Cases 2023; 10:196–9. https://doi.org/10.22551/2023.41.1004.10274.10.22551/2023.41.1004.1027438155997 PMC 10754039 · doi ↗ · pubmed ↗
- 2Bhutani R Walton S. Diabetic Bullae. Br J Diabetes 2015; 15:8. https://doi.org/10.15277/bjdvd.2015.004.10.15277/bjdvd.2015.004 · doi ↗
- 3Michael MJ Mefford JM Lahham S Chandwani CE. Bullosis Diabeticorum. West J Emerg Med 2016; 17:188. https://doi.org/10.5811/westjem.2016.1.29710.10.5811/westjem.2016.1.2971026973748 PMC 4786242 · doi ↗ · pubmed ↗
- 4Chiriac A Costache I Podoleanu C Naznean A Stolnicu S. Bullosis Diabeticorum in a Young Child: Case Report of a Very Rare Entity and a Literature Review. Can J Diabetes 2017; 41:129–31. https://doi.org/10.1016/j.jcjd.2016.10.005.10.1016/j.jcjd.2016.10.00528017292 · doi ↗ · pubmed ↗
- 5Bello F Samaila OM Lawal Y Nkoro UK. 2 Cases of Bullosis Diabeticorum following Long-Distance Journeys by Road: A Report of 2 Cases. Case Rep Endocrinol 2012; 2012:367218. https://doi.org/10.1155/2012/367218.10.1155/2012/36721823119191 PMC 3479936 · doi ↗ · pubmed ↗