Effectiveness of Myofascial Release Compared to Manual Lymphatic Drainage in Reducing Post-Treatment Shoulder Pain and Stiffness Among Patients Who Underwent Breast Cancer Surgery and Adjuvant Radiotherapy: Randomised controlled trial
Chellappa Vijayakumar, Ankit Jain, M. Kalaranjani, Uday S. Kumbhar, N. Kumar, G.S. Sreenath

TL;DR
This study found that myofascial release massage is more effective than lymphatic drainage in reducing shoulder pain and improving movement after breast cancer surgery and radiotherapy.
Contribution
The study demonstrates that myofascial release is superior to manual lymphatic drainage in improving post-treatment shoulder outcomes in breast cancer patients.
Findings
MRT significantly reduced pain compared to MLD (P < 0.001).
MRT improved shoulder range of motion more than MLD (P < 0.001).
MRT reduced shoulder dysfunction more effectively than MLD (P < 0.001).
Abstract
This study aimed to adapt the myofascial release technique (MRT) in the form of massage, which will reduce pain and functional restriction of the shoulder joint compared to manual lymphatic drainage (MLD). This study was conducted in a tertiary care hospital in South India from September 2021 to September 2023. The study population included 98 patients older than 18 years who underwent surgery/adjuvant radiotherapy for breast cancer and developed complications. Patients with tendon/muscle injuries in neck/skin conditions, which made MRT difficult, were excluded. A trained physiotherapist delivered the interventions. Patient pain, range of movements at shoulder joint, shoulder dysfunction and quality of life were assessed at the time of the first (T0) and fourth session (T1) and after one month of the completion of treatment (T2). Compared to the MLD group, the MRT group experienced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
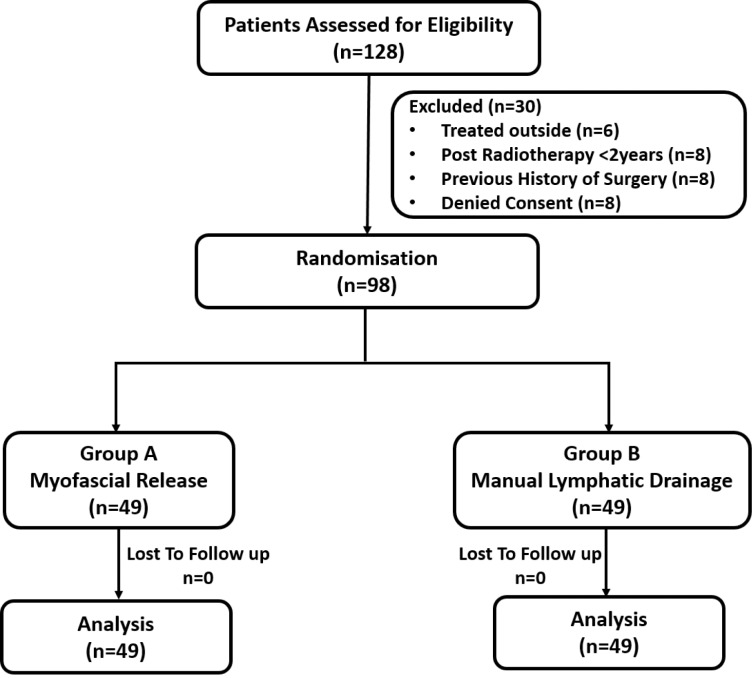 Fig. 1
Fig. 1| n (%) | ||
|---|---|---|
|
| ||
| Baseline Characteristics | MLD group (n = 49) | MRT group (n = 49) |
|
| 50.7 ± 10.3 | 49.7 ± 11.0 |
|
| 30 (61.2) | 24 (48.9) |
|
| ||
| Stage II | 20 (40.8) | 21 (42.9) |
| Stage III | 29 (59.2) | 28 (57.1) |
|
| ||
| N+ | 36 (73.5) | 37 (75.5) |
| N- | 13 (26.5) | 12 (24.5) |
|
| ||
| Breast conservating therapy | 11 (22.4) | 10 (20.4) |
| Modified radical mastectomy | 38 (77.6) | 39 (79.6) |
|
| ||
| Axilla levels 1, 2, 3 and SCF | 16 (32.6) | 17 (34.7) |
| Axilla levels 3 and 4 | 23 (47.0) | 24 (49.0) |
| No axilla radiation | 10 (20.4) | 8 (16.3) |
|
| ||
| Pain | 34 (69.4) | 32 (65.3) |
| Stiffness | 9 (18.4) | 11 (22.4) |
| Lymphoedema | 6 (12.2) | 5 (10.2) |
|
| ||
| VAS | 6 (2) | 7 (2) |
| Flexion ROM | 130.0 (6.0) | 124.0 (32.0) |
| Extension ROM | 38.0 (10.5) | 36.0 (7.0) |
| Abduction ROM | 128.0 (26.0) | 121.0 (20.7) |
| Adduction ROM | 24.0 (7.0) | 23.0 (3.0) |
| DASH | 45.0 (22.0) | 52.0 (24.7) |
| FACT-G | 79.0 (14.5) | 83.5 (21.5) |
| QOL score | 102.0 (17.5) | 103.5 (24.5) |
| Pre MRT | Post MRT | ||||||
|---|---|---|---|---|---|---|---|
|
|
| ||||||
| Variable | 25th | 50th (median) | 75th | 25th | 50th (median) | 75th | |
| VAS | 6.0 | 7.0 | 8.0 | 3.0 | 3.0 | 4.0 | <0.001 |
| Flexion ROM | 100.0 | 124.0 | 132.0 | 114.0 | 130.0 | 140.0 | <0.001 |
| Extension ROM | 31.0 | 36.0 | 38.0 | 36.0 | 40.0 | 45.0 | <0.001 |
| Abduction ROM | 109.2 | 121.0 | 130.0 | 120.0 | 134.0 | 138.0 | <0.001 |
| Adduction ROM | 20.0 | 23.0 | 26.0 | 24.0 | 26.0 | 27.0 | <0.001 |
| DASH | 45.0 | 52.0 | 69.7 | 36.0 | 40.0 | 50.0 | <0.001 |
| FACT-G | 70.0 | 83.5 | 91.5 | 80.0 | 92.0 | 97.5 | <0.001 |
| QOL score | 91.0 | 103.5 | 115.5 | 104.5 | 114.5 | 123.5 | <0.001 |
| Pre MLD | Post MLD | ||||||
|---|---|---|---|---|---|---|---|
|
|
| ||||||
| Variable | 25th | 50th (median) | 75th | 25th | 50th (median) | 75th | |
| VAS | 5.0 | 6.0 | 7.0 | 3.5 | 4.0 | 5.0 | <0.001 |
| Flexion ROM | 126.0 | 130.0 | 132.0 | 128.0 | 132.0 | 138.0 | <0.001 |
| Extension ROM | 31.5 | 38.0 | 42.0 | 37.0 | 40.0 | 44.0 | <0.001 |
| Abduction ROM | 110.0 | 128.0 | 136.0 | 114.0 | 130.0 | 140.0 | <0.001 |
| Adduction ROM | 20.0 | 24.0 | 27.0 | 23.0 | 26.0 | 27.0 | <0.001 |
| DASH | 38.0 | 45.0 | 60.0 | 36.0 | 40.0 | 52.0 | <0.001 |
| FACT-G | 73.5 | 79.0 | 88.0 | 80.0 | 83.0 | 90.0 | <0.001 |
| QOL score | 95.5 | 102.0 | 113.0 | 104.0 | 106.0 | 117.0 | <0.001 |
| Median (IQR) | |||
|---|---|---|---|
|
| |||
| MLD | MRT | ||
|
| |||
| Baseline | 6 (2) | 7 (2) | |
| Post-intervention | 4 (2) | 3 (1) | |
| Median change | 2 (2) | 3 (2) | <0.001 |
|
| |||
| Baseline | 130.0 (6.0) | 124.0 (32.0) | |
| Post-intervention | 132.0 (10.0) | 130.0 (26.0) | |
| Median change | - 4.0 (4.0) | - 9.5 (4.0) | <0.001 |
|
| |||
| Baseline | 38.0 (10.5) | 36.0 (7.0) | |
| Post-intervention | 40.0 (7.0) | 40.0 (9.0) | |
| Median change | - 1.0 (4.0) | - 5.0 (2.5) | <0.001 |
|
| |||
| Baseline | 128.0 (26.0) | 121.0 (20.7) | |
| Post-intervention | 130.0 (26.0) | 134.0 (18.0) | |
| Median change | - 2.0 (4.0) | - 9.0 (4.0) | <0.001 |
|
| |||
| Baseline | 24.0 (7.0) | 23.0 (3.0) | |
| Post-intervention | 26.0 (4.0) | 26.0 (3.0) | |
| Median change | 0 (2.0) | - 3.0 (4.0) | <0.001 |
|
| |||
| Baseline | 45.0 (22.0) | 52 (24.7) | |
| Post-intervention | 40.0 (16.0) | 40.0 (14.0) | |
| Median change | 4.0 (4.0) | 10.0 (8.0) | <0.001 |
|
| |||
| Baseline | 79.0 (14.5) | 83.5 (21.5) | |
| Post-intervention | 83.0 (10.0) | 92.0 (17.5) | |
| Median change | - 4.0 (4.0) | - 6.0 (4.0) | 0.005 |
|
| |||
| Baseline | 102.0 (17.5) | 103.5 (24.5) | |
| Post-intervention | 106.0 (13.0) | 114.5 (19.0) | |
| Median change | - 4.0 (3.0) | - 8.0 (6.0) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Lymphatic System and Diseases · Nerve Injury and Rehabilitation
1. Introduction
Breast cancer (BC) is the most common cancer in India, affecting one in every 29 women.^1^ The treatment strategy for BC includes a combination of surgery, radiotherapy, chemotherapy and targeted therapy. There are various complications of these treatment modalities, the most common being lymphoedema and pain in the upper limb, leading to restriction in the shoulder joint mobility and decreased shoulder function. The incidence of lymphoedema in the upper limb varies between 2% and 40% in patients treated with surgery, radiation or both.^2^ This causes significant patient morbidity, especially now that the survival rates are significantly improved.
Several methods and techniques have been tried to prevent and treat lymphoedema and pain after surgery and radiotherapy of the breast. These include complete decongestive therapy, an intermittent pneumatic compression pump and oral pharmaceuticals.^3^ One such option, the myofascial release technique (MRT), is a form of massage involving sequential palpation to identify areas of tension, restriction or pain and thereby applying graded pressure until there is a release.^4^ This release reduces lymphoedema and, subsequently, pain and improves the functionality of the shoulder joint. The effectiveness of MRT as a tool to reduce lymphoedema and, subsequently, pain and improvement in functionality of the shoulder joint has been introduced in some studies.^5^ However, more studies with convincing evidence are needed. Therefore, this study was planned to compare the effectiveness of MRT and manual lymphatic drainage (MLD) in reducing post-treatment morbidity in BC patients who have undergone surgery and adjuvant radiotherapy. As a manual therapy focused on restoring fascia length and reducing pain, MRT has shown benefits like improved range of motion across various populations. Although it seems suitable for addressing post-treatment impairments in BC survivors, no systematic reviews or meta-analyses have yet explored its effects in this group.^6^ Adding MRT to a 12-week standard physical therapy program may help reduce scapular protraction and anterior tilting at the scapulothoracic joint during arm movements. However, as these findings are from exploratory secondary analyses, further investigation is needed to determine their clinical significance.^7^
2. Methods
2.1. Study design
This prospective randomised controlled trial was conducted in a tertiary care centre in South India from September 2021 to September 2023. All BC patients older than 18 years who underwent surgery and adjuvant radiotherapy and developed complications like lymphoedema, shoulder dysfunction, pain, heaviness and numbness were enrolled in the study. Patients treated partially elsewhere, having tendon/muscle injuries in the neck and ipsilateral arm, skin conditions like eczema, psoriasis, local or generalised infection, neck or ipsilateral limb venous thrombosis, embolus and those on anticoagulation and with previous surgical history to the ipsilateral arm, shoulder, neck and chest, which made MRT difficult, were excluded from the study. The efficacy of the MRT is low after two years of surgery/radiotherapy. Hence, the upper limit was fixed as two years post-treatment.^8^ Randomisation was done at the first visit to the physiotherapy outpatient department, four months after adjuvant radiotherapy, based on computer-generated permuted random size blocks of sizes four and six. Allocation was concealed using a sequentially numbered, opaque, sealed envelope technique. The physiotherapist opened a sealed envelope prepared by a person independent of the investigators.
Sample size calculation was done using Open Source Epidemiologic Statistics for Public Health, Version 3.01 (OpenEpi, Emory University, Georgia, USA). The sample size was calculated to be a minimum of 49 subjects in each group respectively, with an attrition rate of 10%, considering the mean difference ± standard deviation of the angle in abduction between baseline and end of the study to be 36 ± 35.84 in the intervention group (MRT) and 17.18 ± 26.15 in the control group (MLD), with power of 80%.^5^
The current study is a single-blinded study in which only the assessor (physiotherapist different from the physiotherapist who provided intervention) assessing the pain and range of motion was not aware of the therapy received by the patient. Possible injuries in each session were recorded. In both groups, patients were positioned in supine decubitus with an arm extender along the body, with the affected arm slightly flexed and lifted to 30 degrees. Patients were administered MRT using four manoeuvres applied in the order of sterno-pectoral, global pectoral, pectoral and subscapularis. Each manoeuvre was applied by placing both hands in contact with the skin to perform three-dimensional fascial movements with graded pressure and stretching of the connective tissue. The approximate duration of each manoeuvre was 10 minutes. This would release the most relevant fascial and fibrosis-related restrictions. Standardisation of the technique was carried out by similarly training all physiotherapists. For MLD, gentle massage and superficial manipulation of the axillary, chest and ipsilateral upper arm were performed in the same order sequence. The duration of each manoeuvre was 10 minutes.
2.2. Outcome parameters
Patient pain was measured as self-perceived pain intensity recorded using a visual analogue scale, with 0 being “no pain at all” and 10 being “maximum tolerable pain.”
Range of movements (ROMs) at the shoulder joint was measured using goniometry. The active angular reach was measured for all movements of the shoulder (i.e. flexion, extension, abduction, adduction) using a manual goniometer. Goniometric measurements were performed by aligning the fulcrum of the goniometer with the corresponding location of the glenohumeral joint axis and aligning the goniometer arms with different bony landmarks depending on the movement. The patient was asked to lift the affected limb after sitting comfortably on a rigid seat with their trunk upright, with knees flexed at 90 degrees and feet flat on the ground. Two repetitions of each movement were conducted, and the average of two measurements was taken for further analysis.
Shoulder dysfunction was also assessed. The disabilities of the arm, shoulder and hand (DASH) scale questionnaire was used to measure the perception of disability in performing daily activities as well as pain, stiffness or loss of strength. Quality of life (QOL) was assessed using the 37-item Functional Assessment of Cancer Therapy for BC Patients (FACT-B) scale, which consists of 27-core FACT-General (FACT-G) scales and 10-item BC subscales.
All outcomes were assessed at the time of the first session (T0), the end of the fourth session (T1) and after one month of the completion of treatment (T2). Baseline comparisons between treatment groups for pain scores, shoulder-active ROM measurements, DASH and QOL were analysed.
2.3. Statistical analysis
The data was analysed using the Statistical Package for the Social Sciences (SPSS), Version 26.0 (IBM Corp., Armonk, New York, USA). Continuous data was summarised as mean and standard deviation. The categorical variable was summarised in the median with quartiles, and the change in median within the group was evaluated using the Wilcoxon signed-rank test and the Mann-Whitney U test between the groups. The change in mean within the group was analysed with paired t-tests, and between the groups, the difference in the mean was obtained with an independent t-test.
3. Results
A total of 98 patients participated in the study with no dropouts [Fig. 1]. The radiation dose schedule used was 40.05 Gy with or without tumour bed boost in 15 fractions, 42.56 Gy in 16 fractions and 50 Gy in 25 fractions. Of these, 40.05 Gy was used in the majority of patients in both groups (44.9% in the MRT group and 38.7% in the MLD group). The demographic profile is tabulated [Table 1].
Consort diagram showing the patient recruitment process in the study.
Among the 98 patients, eight in the MRT group and 10 in the MLD group did not undergo irradiation of their lymph node stations, as there was no clinical indication for the same. Pre- and post-intervention scores for MRT and MLD are tabulated, respectively [Table 2, Table 3].
3.1. Visual analogue scale score
There was a significant difference in subjective pain in both groups, which was more significant in the MRT group. The median VAS score for MLD patients pre-intervention was six, which decreased to four (P values < 0.001), whereas in the MRT group, the pre-intervention VAS score was seven, which decreased to three (P < 0.001).
3.2. Shoulder range of movements
There was a significant improvement in shoulder movements, including flexion, extension, abduction and adduction, after MRT. However, improvement was also seen in the MLD group, which was less than that of MRT [Table 2, Table 3].
3.3. Disabilities of the arm, shoulder and hand score
In the MRT group, the median DASH score pre-intervention was 52, which decreased to 40 (P < 0.001), while in the MLD group, the pre-intervention DASH score was 45 and decreased to 40 (P < 0.001). The median difference in pre- and post-intervention scores was significantly higher in the MR group [Table 4].
3.4. Quality of life
In the MRT group, the median pre-intervention score for FACT-G was 83.50, while post-intervention, the score increased to 92.00 (P < 0.001). The total QOL score also increased significantly from 103.50 to 114.50 (P < 0.001). However, in the MLD group, the median pre- and post-intervention FACT-G scores were 79.00 and 83.00, respectively. Although significant, the QOL did not increase much in this group.
4. Discussion
This randomised trial enrolled 98 BC patients with complications post-surgery and adjuvant radiotherapy and showed that pain and shoulder joint function improvement was better with MRT than with MLD. Improvement in QOL was seen post-intervention in both groups. However, it was significantly higher in the MRT group than in the MLD group.
Pain was one of the most common symptoms in BC patients who participated in this study. The VAS scale is the most reliable in assessing pain subjectively.^9^ The MRT uses the principles of biomechanical loading of soft tissue and the modification of neuronal reflexes through the stimulation of mechanoreceptors in the fascia, which is a three-dimensional connective tissue network that surrounds and supports the musculoskeletal and visceral components in the body.^10^ Fascial restriction causes pressure on them, leading to pain and dysfunction. Through MRT, fascial restrictions are released, and it facilitates the restoration of healthy tissue, thus having a potential effect on pain perception.^11^
The study results were consistent with previous studies of the effect of fascial release on the management of BC with or without lymphoedema and also in cervical, lumbar and epicondylitis pain.^121314^ In this study, the MLD was also effective in decreasing pain but not as significant as the MRT. A significant improvement in the range of movements was noted at the shoulder joints, especially flexion and abduction, in the MRT group. In the MLD group, there was a difference in the movements, but it did not go beyond the minimum detectable change.^15^ As supported by the previous studies, MRT focuses on reducing fibrosis and scarring as well as improving the range of movements in BC and other diseases involving joints.^121617^
A statistically significant decrease in the DASH score suggests that the functionality of the shoulder joint improved in MRT compared to the MLD group. This is due to an improved range of motion at the shoulder joint and subjectively improved pain. The QOL score was statistically improved in the MRT group, whereas in the MLD group, although statistically significant, the improvement in scores was much less. Conversely, the previous studies have shown no improvement in the FACT scores after MRT, which is in contrast to the current study, probably because of drastic improvement in pain and improved shoulder function.^12^
Like the other study, this study also found notable improvements in shoulder ROM (abduction, flexion and internal/external rotation) in the MRT group, likely due to neurobiological self-regulation responses that helped normalise movement.^18^ A recent systematic review highlighted the need for well-designed studies to evaluate the potential impact of massage therapy on upper limb impairment in BC patients.^19^
4.1. Limitations
This study has some limitations. The overall intervention effect might not be due to the intervention alone. It might also be due to the interaction of other treatments for concerns such as pain and lymphoedema. Hence, type II errors may persist. It is not easy to prove the long-term effect of the MRT on lymphoedema and shoulder dysfunction with a one-month follow-up study. Therefore, long-term follow-up studies and parallel randomised control trials are needed to analyse the long-term effectiveness of MRT.
5. Conclusion
This study showed a significant improvement in postoperative pain, shoulder function and QOL in patients who underwent MRT. There was also improvement in the MLD group, but it was inferior to that of the MRT group. Hence, further studies are needed to establish the long-term effectiveness of MRT and study the synergistic effect of manual lymphatic drainage technique.
Authors' Contribution
Chellappa Vijayakumar: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing - Original Draft, Validation, Supervision. Ankit Jain: Formal Analysis, Writing - Original Draft. M. Kalaranjani: Investigation, Data Curation, Formal Analysis. Uday S. Kumbhar: Conceptualization, Methodology, Validation, Supervision, Writing - Review & Editing. N. Kumar: Conceptualization, Methodology, Writing - Review & Editing. G.S. Sreenath: Validation, Supervision, Writing - Review & Editing.
Acknowledgement
The authors extend their sincere gratitude to Dr. Shyama Prem, Professor, Department of Radiation Oncology, JIPMER, Puducherry, India, for her invaluable support of this study. The authors also express their heartfelt appreciation to all the physiotherapists in the Department of PMRC, JIPMER, Puducherry, for their significant contributions to this research.
Ethics Statement
The study protocol was approved by the Institute Ethics Committee of Jawaharlal Institute of Postgraduate Medical Education and Research and conducted per the standards of the Declaration of Helsinki. Written and well-informed consent was obtained from all the participants before commencing the study, and measures were taken to protect patient privacy. The trial was registered at www.ctri.gov.in (CTRI number: REF/2022/02/052016).
Conflicts of Interest
The authors declare no conflict of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mathur P Sathishkumar K Chaturvedi M Das P Sudarshan KL Santhappan S. Cancer statistics, 2020: Report from National Cancer Registry programme, India. JCO Glob Oncol 2020; 6:1063–75. https://doi.org/10.1200/go.20.00122.10.1200/go.20.0012232673076 PMC 7392737 · doi ↗ · pubmed ↗
- 2Deo SV Ray S Rath GK Shukla NK Kar M Asthana S. Prevalence and risk factors for development of lymphedema following breast cancer treatment. Indian J Cancer 2004; 41:8–12.10.4103/0019-509X.1233815105573 · doi ↗ · pubmed ↗
- 3Li L Yuan L Chen X Wang Q Tian J Yang K. Current treatments for breast cancer-related lymphoedema: A systematic review. Asian Pac J Cancer Prev 2016; 17:4875–83. https://doi.org/10.22034/apjcp.2016.17.11.4875.10.22034/apjcp.2016.17.11.487528030915 PMC 5454690 · doi ↗ · pubmed ↗
- 4Marshall-Mc Kenna R Paul L Mc Fadyen AK Gilmartin A Armstrong A Rice AM. Myofascial release for women undergoing radiotherapy for breast cancer: A pilot study. Eur J Physiother 2014; 16:58–64. https://doi.org/10.3109/21679169.2013.872184.10.3109/21679169.2013.872184 · doi ↗
- 5Ajimsha MS Al-Mudahka NR Al-Madzhar JA. Effectiveness of myofascial release: Systematic review of randomized controlled trials. J Bodyw Mov Ther 2015; 19:102–12. https://doi.org/10.1016/j.jbmt.2014.06.001.10.1016/j.jbmt.2014.06.00125603749 · doi ↗ · pubmed ↗
- 6Lara-Palomo IC Castro-Sánchez AMCórdoba-Peláez MM Albornoz-Cabello M Ortiz-Comino L. Effect of myofascial therapy on pain and functionality of the upper extremities in breast cancer survivors: A systematic review and meta-analysis. Int J Environ Res Public Health 2021; 18:4420. https://doi.org/10.3390/ijerph 18094420.10.3390/ijerph 1809442033919315 PMC 8122330 · doi ↗ · pubmed ↗
- 7De Baets L De Groef A Hagen M Neven P Dams L Geraerts I. The effect of myofascial and physical therapy on trunk, shoulder, and elbow movement patterns in women with pain and myofascial dysfunctions after breast cancer surgery: Secondary analyses of a randomized controlled trial. PM R 2023; 15:1382–91. https://doi.org/10.1002/pmrj.12975.10.1002/pmrj.1297536989084 · doi ↗ · pubmed ↗
- 8De Groef A Van Kampen M Vervloesem N Dieltjens E Christiaens MR Neven P. Effect of myofascial techniques for treatment of persistent arm pain after breast cancer treatment: Randomized controlled trial. Clin Rehabil 2018; 32:451–61. https://doi.org/10.1177/0269215517730863.10.1177/026921551773086328914087 · doi ↗ · pubmed ↗