Erythema Multiforme Triggered by Trichophyton mentagrophytes: An unusual association
María Zulaika-Lloret, álvaro Prados-Carmona, Mar Rodríguez-Troncoso, Ricardo Ruiz-Villaverde

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
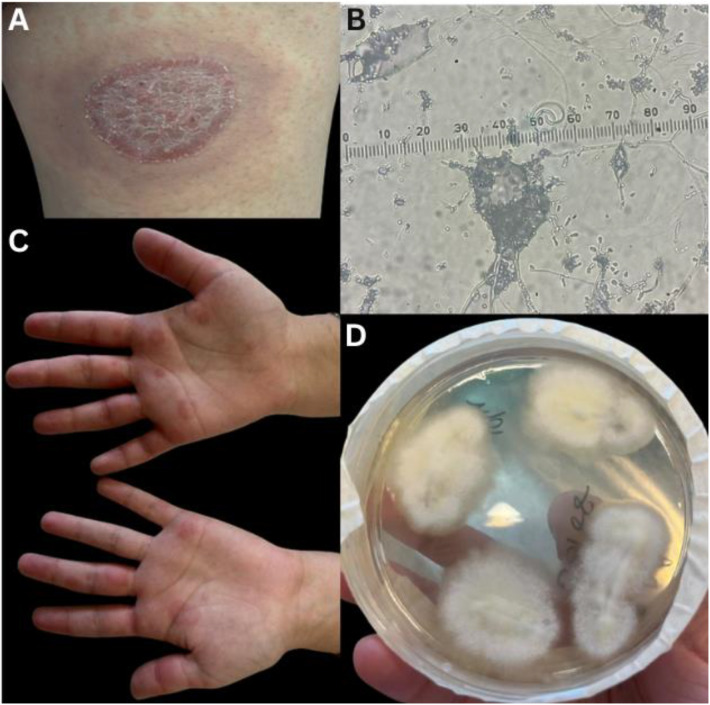 Fig. 1
Fig. 1| Authors and year of publication | Journal | Microorganism identified |
|---|---|---|
| Subban |
|
|
| Rahman |
|
|
| Salim and Young |
|
|
|
| ||
| Atzori |
|
|
|
| ||
| Gilaberte |
|
|
| Cañueto |
|
|
|
| ||
| Tanimura and Ota |
|
|
| Silvestre-Torner |
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNail Diseases and Treatments · Oral Health Pathology and Treatment · Cancer and Skin Lesions
1. Introduction
A 22-year-old female patient was referred to a dermatology outpatient clinic at a tertiary care hospital in Granada, Spain, in 2024, complaining a pruritic rash on the hands, feet, elbows and back that had been present for 3 days.
She had been attended at the emergency department the previous week with a 2-week-old round erythematous scaly plaque on her right thigh, which had been diagnosed as tinea corporis and treated with topical clotrimazole. The patient reported no improvement of the latter lesion despite treatment and the appearance of new pruritic lesions on the back, palms, soles and elbows. She denied fever, contact with animals, previous upper respiratory tract infections or recent episodes of herpes. She denied the intake of medical drugs regularly or sporadically.
Physical examination revealed an erythematous plaque 4 cm in diameter with a raised border and a scaly centre on the posterior aspect of the right thigh, compatible with the initial diagnosis of tinea corporis [Fig. 1A]. Direct examination was performed at that time and macroconidia were seen [Fig. 1B]. A sample of scales was taken for culture. In addition, she had erythematous oedematous target lesions with a violet border and a whitish centre on her palms and soles, as well as confluent urticariform papules with a symmetrical distribution at the elbows and on the back without compromise of mucous membranes being consistent with erythema multiforme (EM) [Fig. 1C].
A: Erythematous plaque with raised border and desquamative centre, compatible with tinea corporis. B: Presence of macroconidia on direct examination. C: Target lesions with a purplish rim and a whitish centre, compatible with erythema multiforme. D: Culture of scales is the growth of T. mentagrophytes.
The culture was positive for Trichophyton mentagrophytes [Fig. 1D]. Oral terbinafine 250 mg daily was prescribed for 4 weeks with complete resolution of the fungal lesion and the EM lesions resolved in 3 weeks. Bilastine 20 mg was added for symptomatic control of pruritus secondary to EM.
2. Comment
EM is a self-limited skin condition characterised by the abrupt appearance of rounded erythematous oedematous papules with concentric areas of dianiform or annular colour change. The centre of the lesions may become violaceous, necrotic or even a central blister may be observed. Although usually asymptomatic, they may be pruritic. It mainly affects the acral areas, frequently palms and soles, with a bilateral and symmetrical distribution. Although infrequently, it may involve mucous membranes, producing erythematous macules, erosions and painful bullae.^12^
EM is often triggered by herpes simplex virus (HSV) and other infections. There is a low percentage of cases associated with drugs though some cases remain idiopathic.^2^ In children, common causes include Mycoplasma pneumoniae, upper respiratory tract infections and HSV.^3^ While EM is rarely associated with superficial mycoses, recent reports suggest that Trichophyton infection can induce EM, likely as an id reaction. Less than 8 cases have been described in the literature, most in association with infection to T. mentagrophytes compared to T. rubrum [Table 1]. T. mentagrophytes provokes a stronger immune response related to acute fungal infections, which may explain its more frequent association with EM.
Although EM linked to T. mentagrophytes is rare, its temporal association with fungal infections suggests a potential causal relationship.^10^ Accurate diagnosis of dermatophyte-associated EM requires mycological studies and clinical correlation, particularly given the rare occurrence of dermatophyte-induced EM.^2310^ Antifungal treatment typically resolves both conditions, further supporting a connection between the fungal infection and EM. Symptomatic control with antihistamines and/or corticosteroids is important in cases where EM does not resolve as a result of antifungal treatment.
Authors' Contribution
All authors substantially contributed to the manuscript and revised it critically. All authors approved the final version of the manuscript.
Ethics Statement
Informed consent for publication was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ito H. Erythema Multiforme Due to Mycoplasma with False-positive H Bs Antigen. Vis J Emerg Med 2023; 33:101845. https://doi.org/10.1016/j.visj.2023.101845.10.1016/j.visj.2023.101845 · doi ↗
- 2Cañueto J Roncero M Unamuno P. Erythema Multiforme Triggered by Tricophytum Mentagrophytes? J Eur Acad Dermatol Venereol 2009; 23:586–7. https://doi.org/10.1111/j.1468-3083.2008.02975.x.10.1111/j.1468-3083.2008.02975.x 18771444 · doi ↗ · pubmed ↗
- 3Silvestre-Torner N Román-Sainz J Gruber-Velasco F. Erythema Multiforme Associated With Trichophyton Mentagrophytes Infection. Actas Dermosifiliogr 2022; 113:966–7. https://doi.org/10.1016/j.ad.2022.01.043.10.1016/j.ad.2022.01.04335724709 · doi ↗ · pubmed ↗
- 4Subban SA Kamalam A Thambiah AS. Erythema Multiforme in Dermatophytosis. Mycosen 1979; 23:452–5.10.1111/j.1439-0507.1980.tb 02630.x 6775223 · doi ↗ · pubmed ↗
- 5Rahman SA Setoyama M Kawahira M Tashiro M. Erythema Multiforme Associated with Superficial Fungal Disease. Cutis 1995; 55:249–51.7796619 · pubmed ↗
- 6Salim A Young E. Erythema Multiforme Associated with Trichophyton Mentagrophytes Infection. J Eur Acad Dermatol Venereol 2002; 16:645–6.10.1046/j.1468-3083.2002.00653_6.x 12482059 · doi ↗ · pubmed ↗
- 7Atzori L Pau M Aste M. Erythema Multiforme ID Reaction in Atypical Dermatophytosis: A Case Report. J Eur Acad Dermatol Venereol 2003; 17:699–701.10.1046/j.1468-3083.2003.00698.x 14761142 · doi ↗ · pubmed ↗
- 8Gilaberte Y Coscojuela C García-Prats MD Mairal MP. Erythema Multiforme Associated with Inflammatory Ringworm On the Hand. Br J Dermatol 2003; 149:1078–9.10.1111/j.1365-2133.2003.05609.x 14632823 · doi ↗ · pubmed ↗