Readmission After Ischemic Stroke in Ningxia, China, From 2017 to 2021: Retrospective Cohort Study
Hua Meng, Xingtian Wang, Dongfeng Pan, Xinya Su, Wenwen Lu, Zhuo Liu, Yuhui Geng, Xiaojuan Ma, Ting Pan, Peifeng Liang

TL;DR
This study analyzed readmission rates after ischemic stroke in China and found diabetes increases risk while being female reduces it.
Contribution
Identified consistent risk factors for ischemic stroke readmission over time using a large retrospective cohort in Ningxia, China.
Findings
12.7% of ischemic stroke patients were readmitted within 5 years.
Diabetes increased readmission risk, while female gender was a protective factor.
Risk factors remained consistent across different time points.
Abstract
Stroke remains a major cause of death and disability worldwide. Ischemic stroke is the most common type of stroke. Readmissions after hospitalization increase the patient burden and waste health resources. This study aimed to calculate rehospitalization rates and explore risk factors associated with rehospitalization in ischemic stroke. In this retrospective cohort study, we identified 12,782 patients admitted for ischemic stroke at People’s Hospital of Ningxia Hui Autonomous Region between January 2017 and December 2021. Groups were determined based on the ID number. The most important factors were selected using the Least Absolute Shrinkage and Selection Operator regression model. Stabilized inverse probability of treatment weighting (SIPTW) was used to correct baseline imbalances between groups. The adjusted hazard ratios and Kaplan-Meier survival curves of significant factors…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
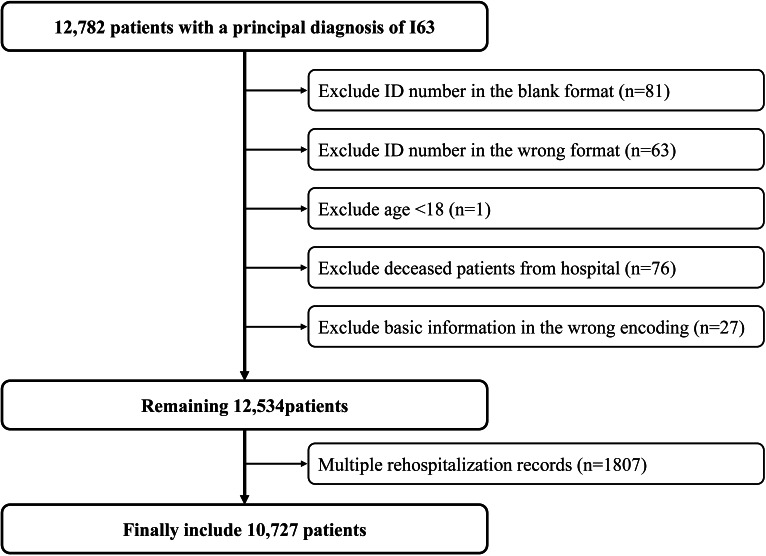 Figure 1
Figure 1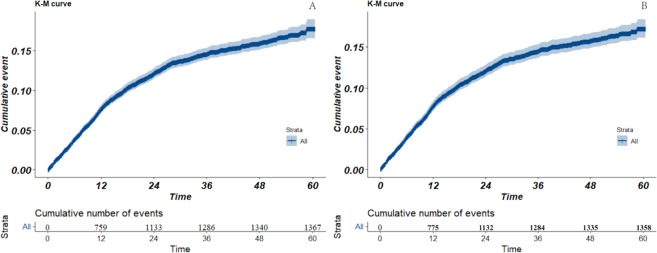 Figure 2
Figure 2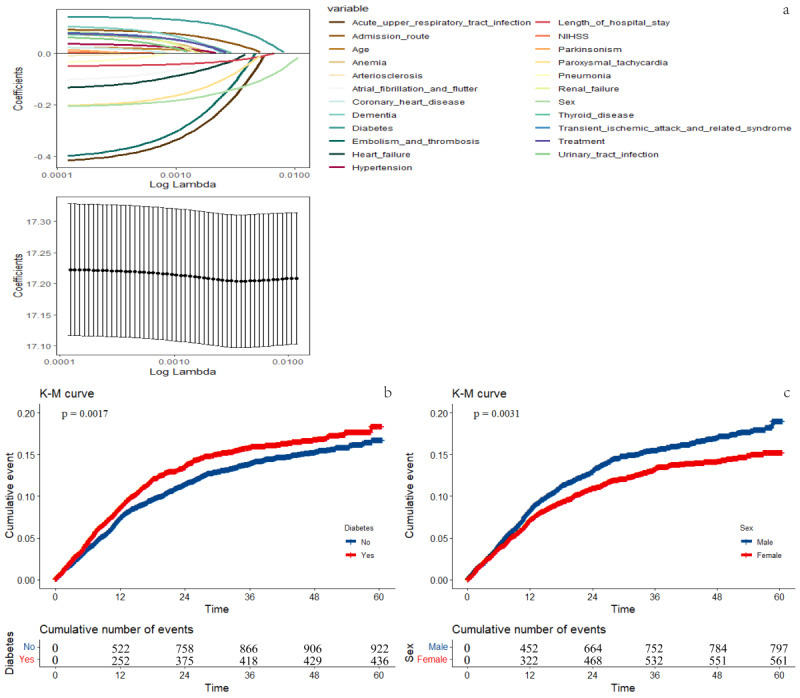 Figure 3
Figure 3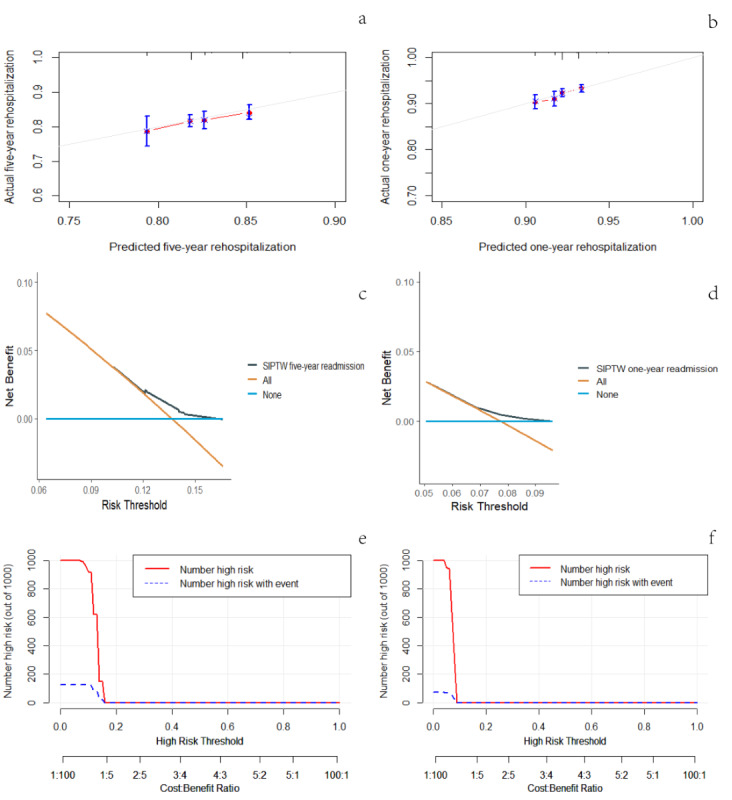 Figure 4
Figure 4| Cohort data | SIPTW | |||||||
|---|---|---|---|---|---|---|---|---|
| No readmission | Readmission | SMD | No readmission | Readmission | SMD | |||
| N=9360 | N=1367 | N=9360.8 | N=1358.1 | |||||
| Male (n, %) | 5159 (55.1) | 794 (58.1) | .039 | 0.060 | 5148.3 (55.0) | 797.0 (58.7) | .020 | 0.075 |
| Age, years (n, %) | ||||||||
| <60 | 2267 (24.2) | 227 (16.6) | <.001 | 0.211 | 2175.2 (23.2) | 305.5 (22.5) | .863 | 0.021 |
| 60‐69 | 2650 (28.3) | 375 (27.4) | 2639.6 (28.2) | 388.8 (28.6) | ||||
| 70‐79 | 2911 (31.1) | 481 (35.2) | 2960.1 (31.6) | 427.1 (31.5) | ||||
| ≥80 | 1532 (16.4) | 284 (20.8) | 1585.8 (16.9) | 236.6 (17.4) | ||||
| Admission route (n, %) | ||||||||
| Emergency | 4579 (48.9) | 629 (46.0) | .187 | 0.060 | 4567.3 (48.8) | 625.7 (46.1) | .259 | 0.065 |
| Others | 1 (0.0) | 0 (0.0) | 1.0 (0.0) | 0.0 (0.0) | ||||
| Outpatient | 4768 (51.0) | 736 (53.8) | 4780.2 (51.1) | 728.4 (53.6) | ||||
| Transferred | 12 (0.1) | 2 (0.1) | 12.2 (0.1) | 3.9 (0.3) | ||||
| Treatment (n, %) | ||||||||
| Anticoagulants | 8847 (94.5) | 1328 (97.1) | <.001 | 0.133 | 8879.2 (94.9) | 1295.3 (95.4) | .931 | 0.028 |
| Thrombectomy | 19 (0.2) | 1 (0.1) | 17.5 (0.2) | 2.7 (0.2) | ||||
| Thrombectomy and thrombolysis | 38 (0.4) | 2 (0.1) | 34.9 (0.4) | 3.7 (0.3) | ||||
| Thrombolysis | 456 (4.9) | 36 (2.6) | 429.2 (4.6) | 56.4 (4.2) | ||||
| Disease (n, %) | ||||||||
| Parkinsonism (n, %) | 111 (1.2) | 25 (1.8) | .047 | 0.053 | 112.8 (1.2) | 18.5 (1.4) | .586 | 0.014 |
| Anemia (n, %) | 367 (3.9) | 28 (2.0) | .001 | 0.110 | 344.9 (3.7) | 52.9 (3.9) | .786 | 0.011 |
| Thyroid disease (n, %) | 1249 (13.3) | 190 (13.9) | .574 | 0.016 | 1253.0 (13.4) | 190.6 (14.0) | .550 | 0.019 |
| Dementia (n, %) | 184 (2.0) | 33 (2.4) | .272 | 0.031 | 186.5(2.0) | 33.5 (2.5) | .300 | 0.032 |
| Transient ischemic attack and related syndrome (n, %) | 643 (6.9) | 108 (7.9) | .163 | 0.039 | 647.1 (6.9) | 111.2 (8.2) | .129 | 0.048 |
| Hypertension (n, %) | 6606 (70.6) | 1045 (76.4) | <.001 | 0.133 | 6677.2 (71.3) | 973.1 (71.7) | .835 | 0.007 |
| Coronary heart disease (n, %) | 2132 (22.8) | 383 (28.0) | <.001 | 0.121 | 2196.0 (23.5) | 327.4 (24.1) | .616 | 0.015 |
| Paroxysmal tachycardia (n, %) | 660 (7.1) | 68 (5.0) | .004 | 0.087 | 668.3 (7.1) | 65.3 (4.8) | .003 | 0.099 |
| Diabetes (n, %) | 2706 (28.9) | 446 (32.6) | .005 | 0.081 | 2738.5 (29.3) | 435.6 (32.1) | .052 | 0.061 |
| Atrial fibrillation and flutter (n, %) | 564 (6.0) | 72 (5.3) | .267 | 0.033 | 570.5 (6.1) | 67.4 (5.0) | .124 | 0.050 |
| Heart failure (n, %) | 735 (7.9) | 122 (8.9) | .172 | 0.039 | 758.5 (8.1) | 102.2 (7.5) | .476 | 0.022 |
| Arteriosclerosis (n, %) | 5190 (55.4) | 812 (59.4) | .006 | 0.080 | 5221.6 (55.8) | 792.1 (58.3) | .113 | 0.051 |
| Embolism and thrombosis (n, %) | 165 (1.8) | 18 (1.3) | .234 | 0.036 | 167.3 (1.8) | 14.8 (1.1) | .074 | 0.059 |
| Acute upper respiratory tract infection (n, %) | 127 (1.4) | 11 (0.8) | .091 | 0.053 | 128.5 (1.4) | 11.9 (0.9) | .192 | 0.047 |
| Pneumonia (n, %) | 309 (3.3) | 43 (3.1) | .763 | 0.009 | 315.1 (3.4) | 47.2 (3.5) | .869 | 0.006 |
| Renal failure (n, %) | 148 (1.6) | 20 (1.5) | .742 | 0.010 | 148.7 (1.6) | 21.0 (1.5) | .915 | 0.004 |
| Urinary tract infection (n, %) | 324 (3.5) | 32 (2.3) | .031 | 0.067 | 310.4 (3.3) | 42.8 (3.2) | .815 | 0.009 |
| Length of hospital stay (n, %) | ||||||||
| <Q1 (<8) | 2394 (25.6) | 162 (11.9) | <.001 | 0.414 | 2229.9 (23.8) | 311.2 (22.9) | .545 | 0.023 |
| Q1-Q2 (8‐10) | 2029 (21.7) | 262 (19.2) | 1999.3 (21.4) | 291.2 (21.4) | ||||
| Q2-Q3 (10‐13) | 2728 (29.1) | 440 (32.2) | 2764.9 (29.5) | 410.7 (30.2) | ||||
| ≥Q3 (≥13) | 2209 (23.6) | 503 (36.8) | 2366.7 (25.3) | 344.9 (25.4) | ||||
| NIHSS (n, %) | ||||||||
| Q1 (≤1) | 2459 (26.3) | 389 (28.5) | .008 | 0.100 | 2483.9 (26.5) | 351.6 (25.9) | .476 | 0.023 |
| Q1-Q2 (1‐2) | 2766 (29.6) | 361 (26.4) | 2728.6 (29.1) | 396.8 (29.2) | ||||
| Q2-Q3 (2‐4) | 2125 (22.7) | 348 (25.5) | 2159.7 (23.1) | 325.1 (23.9) | ||||
| >Q3 (>4) | 2010 (21.5) | 269 (19.7) | 1988.5 (21.2) | 284.6 (21.0) | ||||
| B | SE | HR | Lower limit | Upper limit | ||
|---|---|---|---|---|---|---|
| 5 years | ||||||
| Sex (female) | −0.188 | 0.055 | .002 | 0.83 | 0.74 | 0.93 |
| Diabetes (yes) | 0.140 | 0.058 | .027 | 1.15 | 1.02 | 1.30 |
| Embolism and thrombosis (yes) | −0.388 | 0.262 | .155 | 0.68 | 0.40 | 1.16 |
| Paroxysmal tachycardia (yes) | −0.209 | 0.127 | .130 | 0.81 | 0.62 | 1.06 |
| Acute upper respiratory tract infection (yes) | −0.445 | 0.291 | .185 | 0.64 | 0.33 | 1.24 |
| 1 year | ||||||
| Sex (female) | −0.135 | 0.073 | .096 | 0.87 | 0.74 | 1.02 |
| Diabetes (yes) | 0.192 | 0.077 | .023 | 1.21 | 1.03 | 1.43 |
| Paroxysmal tachycardia (yes) | −0.319 | 0.168 | .107 | 0.73 | 0.49 | 1.07 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Stroke Rehabilitation and Recovery · Antiplatelet Therapy and Cardiovascular Diseases
Introduction
Because of its high mortality and disability rate, cerebrovascular disease (CVD) seriously threatens human health and brings great pressure to the medical care system, especially in limited-income countries [12]. CVD is the primary cause of death and disability in adults in China [34]. It is estimated that about 330 million patients experience difficulties from CVD in China [5]. The Annual Report on Cardiovascular Health and Diseases in China (2021) shows that, in 2019, the total number of discharged patients with CVD was 26.8441 million. The total hospitalization expenses of CVD were RMB 136.028 billion. After adjusting for price factors, the average annual growth rate of total hospitalization expenses for ischemic stroke and hemorrhagic stroke has been 18.82% and 13.51%, respectively, since 2004 [6]. Readmissions are common: up to 22% of individuals experience 30-day readmissions after neurologic hospitalization [7].
High readmission rates may indicate unresolved problems at initial discharge [8], the quality of immediate post-hospital care, a more chronically ill population, or combinations of these factors. High readmission rates are also associated with a substantial economic burden on the health care system and may represent opportunities to reduce avoidable costs [9]. Reduction of readmission rates has become the goal of national health care reform, health insurance, and Medicaid service centers.
To reduce rehospitalization rates in patients with ischemic stroke, it is essential to fully understand preventable and unpreventable predictors that may influence rehospitalization. Previous studies have reported that infection [10], advanced age [11], and diabetes [12] are the most common causes of rehospitalization in patients with stroke. Furthermore, because most readmissions were measured within 30 days of the event, it is unknown whether the reasons for long-term readmissions differ [13].
This study focused on 3 main areas to better understand the factors contributing to rehospitalization in patients with ischemic stroke: the rates of rehospitalization at various intervals (1 year and 5 years), the differences in patient characteristics between those who were rehospitalized and those who were not, and the factors influencing rehospitalization in patients.
Methods
Ethical Considerations
This study followed the principles of the Declaration of Helsinki and was approved by People's Hospital of Ningxia Hui Autonomous Region (2020-KY-053), and the informed consent was waived off by the review boards due to the nature of this research. All data in the manuscript and supplementary materials were anonymized in accordance with ethical standards, ensuring no personally identifiable information could be discerned.
Data Resources and Patients
This is a retrospective cohort study. In 2022, we examined electronic health record data from all patients who were discharged from People’s Hospital of Ningxia Hui Autonomous Region between January 2017 and December 2021. The electronic health record data were anonymized and accessed in a secure environment. The data have a hierarchical structure, including medical record number, demographic characteristics, primary and secondary diagnoses, procedures, method of payment, and a total of 642 variables. The hospital enforces rigorous follow-up and intervention protocols for patients with stroke. Qualified specialists in brain and heart health provide guidance on exercise and rehabilitation after discharge via the WeChat app. Public health physicians conduct telephone follow-ups at 3 and 6 months post-discharge, while a professional doctor performs an in-person visit at 12 months. This visit primarily includes blood sample testing, carotid ultrasound examinations, and adjustments to the patient’s medication regimen.
The criteria for data included in this study were as follows: (1) patients aged 18 years or older with a principal diagnosis of ischemic stroke (International Classification of Diseases, Tenth Edition [ICD]-10: I63); (2) patients readmitted to any hospital after discharge due to an ischemic stroke-related condition. The first onset of ischemic stroke was considered the index event, and readmission was the endpoint event. Patients discharged from the hospital who were deceased, under 18 years of age, or had incorrect ID numbers and encoding formats were excluded. If the same patient had multiple rehospitalization records, only the first 2 hospitalization records were retained.
Outcome Measures
Rehospitalization for ischemic stroke refers to the same individual being readmitted to the hospital with ischemic stroke as the primary diagnosis. The rehospitalization rate was calculated by dividing the number of patients readmitted after hospitalization by the total number of patients discharged alive during the same period [14].
Rehospitalizations were identified using ID numbers and the main diagnostic code for the disease from the electronic health data of The People’s Hospital of Ningxia Hui Autonomous Region from 2017 to 2021. The primary outcome was a 5-year rehospitalization rate, and the secondary outcomes were 1-year rehospitalization rates.
Study Variables
Published relevant literature was reviewed to summarize and integrate the factors involved [79111215-20undefinedundefinedundefinedundefinedundefined]. Covariates considered for confounding adjustment included sex, age (<60, 60‐69, 70‐79, ≥80), admission route, length of stay (LOS), anemia (D50-64), thyroid disease (E00-07), diabetes (E10-14), dementia (F00-03), parkinsonism (G20), transient ischemic attack and related syndrome (G45), hypertension (I10-15), coronary heart disease (CHD) (I20-25), paroxysmal tachycardia (I47), atrial fibrillation and flutter (I48), heart failure (I50), arteriosclerosis (I70), embolism and thrombosis (I74), acute upper respiratory tract infection (J00-06), pneumonia (J12-18), renal failure (N17-N19), and urinary tract infection (N39.000), treatment (anticoagulants, thrombectomy, thrombolysis, thrombectomy and thrombolysis), and NIH Stroke Scale (NIHSS) score.
Statistical Analysis
The variables of admission route and NIHSS score had missing values; the number of missing values was 5 (0.04%) and 10346 (96.4%), respectively. The missing mechanism was determined to be missing completely at random according to the correlation coefficient matrix between the missing values and other variables (Table S1 in Multimedia Appendix 1) [21]. Therefore, the incomplete data for admission route and NIHSS score were imputed simultaneously using multiple imputations (n=25) with the R package MICE (TNO and University of Twente) [2223]. Based on the Akaike information criterion (AIC) value, one of the imputed datasets was selected for analysis.
Some previous studies have demonstrated that the Least Absolute Shrinkage and Selection Operator (LASSO) method was superior to traditional methods [24-26]. LASSO regression was used to avoid overfitting and collinearity [26]. Therefore, LASSO analysis was used to select variables to be included in the Cox proportional hazards regression model (Cox model). The “glmnet” package was used to analyze the LASSO regression model [27].
Stabilized inverse probability of treatment weighting (SIPTW) was used to achieve a balanced comparison between the readmission and non-readmission groups. This method helps maintain the original data’s sample size and ensures an appropriate class I error rate [28]. Probability was estimated through a logistic regression model with rehospitalization as the dependent variable, considering variables such as age, anemia, hypertension, CHD, length of hospital stay, treatment, urinary tract infection, and NIHSS [29]. The balance of potential confounders at baseline was evaluated using the absolute standardized difference (SMD), where an SMD greater than 0.1 indicated a significant difference in potential confounders between cases and controls [30].
The Cox model was constructed by backward Cox regression using the AIC selection criteria, and the best model was chosen based on the least AIC [31-33]. The “survival” package was used for Cox analysis, and the “MASS” package was used to perform stepwise backward analysis. The log-rank test conducted stepwise backward Cox analysis of significant factors for rehospitalization rates for SIPTW. The Kaplan-Meier curve was obtained using the “survminer” package.
Model Evaluation
Calibration curves were plotted using the “rms” package, which compares the agreement between the model’s predicted and observed probabilities [34].
Decision curve analysis was conducted using the ‘ggDCA’ package to assess the utility of a model in supporting clinical decisions [35].
Clinical impact curves were drawn using the ‘rmda’ package to evaluate the model’s recognition value in rehospitalized patients [36].
A 2-sided P value of less than .05 indicated statistical significance. Data screening and extraction were performed using Excel version 2016, and other analyses were carried out using R (version 4.2.2).
Results
The results of the data inclusion procedure are shown in Figure 1. A total of 10,727 eligible patients with ischemic stroke were included in the study. Among all patients, 12.7% (1367) were readmitted within 5 years after discharge, and 7.2% (769) were rehospitalized within 1 year. The Kaplan-Meier curves are shown in Figure 2.
There was a significant imbalance in age, treatment, anemia, hypertension, CHD, and LOS between the 2 groups with or without rehospitalization within 5 years. After using the SIPTW, the SMD did not exceed 0.1. Baseline characteristics are shown in Table 1. Significant differences in age, anemia, hypertension, CHD, diabetes, LOS, and NIHSS were observed between the 2 groups with or without rehospitalization within 1 year. Following SIPTW adjustment, balance was achieved between the 2 groups (Table S2 in Multimedia Appendix 1).
On readmission within 5 years, sex, admission route, diabetes, heart failure, acute upper respiratory tract infection, paroxysmal tachycardia, LOS, embolism, and thrombosis were indicated for inclusion from a 5-year SIPTW LASSO regression. Analyzing the above variables mentioned above, stepwise backward Cox regression after SIPTW showed that the significant variable was diabetes, with a hazard ratio (HR) of 1.15 and a 95% confidence interval (95% CI) of 1.02 to 1.30. As shown in Figure 3, among 3175 patients with ischemic stroke with diabetes, 436 (13.7%) patients with ischemic stroke and diabetes were rehospitalized for treatment within five years. Sex (HR 0.83; 95% CI 0.74‐0.93) was identified as a protective factor for rehospitalization in patients with ischemic stroke (Table 2). The Kaplan-Meier curves are displayed in Figure 3(B and C).
Sex, diabetes, paroxysmal tachycardia, and urinary tract infection were indicated for inclusion from a 1-year SIPTW LASSO regression (Figure S1 in Multimedia Appendix 1). In the stepwise backward Cox analysis of SIPTW, the significant factor was diabetes (HR 1.21; 95% CI 1.03‐1.43).
Unweighted stepwise backward Cox analyses are listed in Table S3 in Multimedia Appendix 1.
Flowchart of patient selection for this study.
Kaplan-Meier curve of rehospitalization patients. A: cohort data; B: stabilized inverse probability of treatment weighting data. K-M curve: Kaplan-Meier curve.
Stabilized inverse probability of treatment weighting and Least Absolute Shrinkage and Selection Operator (LASSO) regression, Kaplan-Meier (K-M) curves of rehospitalization within 5 years in patients with ischemic stroke (a): LASSO regression; (b) within 5 years in patients with ischemic stroke without or with diabetes; and (c) within 5 years in different sex patients with ischemic stroke. NIHSS: NIH Stroke Scale.
Model Validation
After performing SIPTW and stepwise backward Cox analysis, it can be observed from Figure 4(A and B) that the calibration curve of the model closely aligns with the diagonal line, suggesting that the model has good predictive power.
The decision curve analysis of the model indicated that if the patient’s risk threshold probability for rehospitalization within 5 years was between 0.074 and 0.165 (Figure 4C), and within 1 year was between 0.057 and 0.096 (Figure 4D), then using the model to determine the need for rehospitalization offers added advantages over the options of full rehospitalization or no rehospitalization.
The clinical impact curve of the model showed that when the risk threshold was greater than 0.13, the high-risk rehospitalization cases of ischemic stroke predicted by the model within 5 years closely matched the true ischemic stroke rehospitalized cases (Figure 4E). When the threshold was above 0.07, the high-risk rehospitalization cases of ischemic stroke predicted by the model within 1 year closely resembled the true ischemic stroke rehospitalized cases (Figure 4F).
Model evaluation of results from 5-year and 1-year rehospitalization analysis after SIPTW (a, b: calibration curve; c, d: decision curve analysis; e, f: clinical impact curve. SIPTW: stabilized inverse probability of treatment weighting.
Discussion
Principal Findings and Comparison With Previous Works
In this study, there were similarities and differences in the influencing factors of rehospitalization at different times. The SIPTW and unweighted stepwise Cox analyses found gender to be significant among the LASSO regression factors for rehospitalization within 5 years.
A study in Sichuan Province included 1,066,752 patients with stroke with an average follow-up of 1.15 years, with a rehospitalization rate of 23% [37]. Between 1986 and 2001, there were 128,511 stroke hospitalizations in Scotland, and approximately 10.8% of patients were rehospitalized within 5 years due to stroke [38]. A study in Singapore included 12,559 patients with stroke, and the rehospitalization rate for recurrent stroke within 5 years was approximately 18.4% [39]. In our study, the low rate of rehospitalization may be attributed to the effective communication between medical staff and patients and their families upon discharge [40], which improved patient compliance with treatment and the professionalism of the accompanying staff. On the other hand, participants were from a single hospital, and in cases of acute illness, they may opt for medical care from nearby facilities like community general practitioners or other urban areas in Ningxia or other provinces [41]. Additionally, these patients are typically managed by specialized palliative care teams and may choose not to be readmitted in the event of complications, opting instead for care at the palliative care facility. The COVID-19 pandemic also had an indirect impact on readmission rates, which is primarily reflected in the reduced accessibility of medical resources and changes in patient health care-seeking behavior. Our study did not systematically collect data on telemedicine usage during the pandemic, which may result in a potential underestimation of readmission rates. Future research should incorporate indicators of health care resource utilization to more comprehensively evaluate the long-term effects of the pandemic on the management of ischemic stroke.
Relevant meta-analyses have shown that common patient-related risk factors associated with increased readmission rates include age, heart failure, nephropathy, respiratory disease, peripheral arterial disease, and diabetes [42]. This aligns with the variables initially screened by LASSO regression in this study. In this study, the results of weighted stepwise Cox regression analysis and unweighted stepwise Cox regression analysis are inconsistent due to variations in the distribution of these variables between the non-rehospitalization group and the rehospitalization group in the original cohort data. Through the SIPTW method used in this study, the original dataset is preserved while adjusting for individual differences between groups, leading to a more balanced data distribution and more reliable results [43].
After adjusting for confounding variables, the study found that women patients had a lower risk of re-hospitalization within 5 years. In the analysis of both 5-year rehospitalization and 1-year rehospitalization, diabetes was considered a risk factor, which aligns with findings from previous studies [193944]. This indicates that readmissions are more prevalent among men and individuals with diabetes, leading to higher health care costs [45]. Patients with diabetes exhibit a more pronounced procoagulant state [46] and experience delayed reperfusion of the ischemic penumbra [47], resulting in poorer recovery for patients with stroke. Experimental evidence suggests that hyperglycemia reduces the number of protective non-inflammatory macrophages, thereby increasing mediators of ischemic brain injury [48] and disrupting the blood-brain barrier [49], impacting the prognosis of patients with ischemic stroke.
Strengths
The main strength of this study is that we investigated patients with ischemic stroke at the People’s Hospital of Ningxia Hui Autonomous Region over a 5-year period. We conducted follow-ups using electronic medical records from multiple hospitals. We included comprehensive details from the initial page of each patient’s medical record for a comparative summary. Additionally, we used LASSO regression to screen factors, used SIPTW to adjust for confounding variables between groups, and conducted backward stepwise Cox analysis to refine the model.
Limitations
This study also has some potential limitations. First, we identified study subjects using ICD-10 diagnosis codes in the database. However, the coding accuracy may vary depending on the complexity of the disease or institution [50]. Second, risk adjustment may be inadequate due to limited information on the case’s front page and a lack of clinical details, such as the disease’s severity and death information. Laboratory tests for atmospheric environmental indicators are missing. Recent studies have suggested that neutrophil percentage, red blood cell distribution width, alkaline phosphatase [51], and ambient particulate matter pollution of different sizes (PM_1_, PM_2.5_, and PM_10_) [37] influence the readmission of patients with stroke prognosis after discharge. Third, the data came from only 1 hospital, and the findings may not represent other geographical areas or medical institutions, limiting the universality of the results. However, the results of the preliminary screening of factors in this study align with previous research results in different regions. Finally, our study primarily focuses on outcomes during hospitalization and mid- to long-term outcomes. However, it does not include long-term follow-up data after discharge, which limits a comprehensive assessment of patients’ long-term functional recovery, risk of recurrence, and quality of life.
Conclusions
In conclusion, our findings suggest inconsistent rehospitalization rates for ischemic stroke disease at different times and that the same factors influence rehospitalization rates. Early prevention and treatment of influencing factors are required for the prognosis of ischemic stroke. Future studies should evaluate whether targeted interventions in populations with high-risk factors reduce rehospitalization rates.
Supplementary material
10.2196/67522Multimedia Appendix 1Supplementary tables and figure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roth GA Abate D Abate KH Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet Nov 1020183921015917361788 doi 10.1016/S 0140-6736(18)32203-7Medline 30496103 PMC 6227606 · doi ↗ · pubmed ↗
- 2Katan M Luft A Global burden of stroke Semin Neurol Apr 2018382208211 doi 10.1055/s-0038-1649503 Medline 29791947 · doi ↗ · pubmed ↗
- 3Ma LY Chen WW Gao RL et al China cardiovascular diseases report 2018: an updated summary J Geriatr Cardiol 01202017118 doi 10.11909/j.issn.1671-5411.2020.01.001Medline 32133031 PMC 7008101 · doi ↗ · pubmed ↗
- 4Wang YJ Li ZX Gu HQ et al China Stroke Statistics: an update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations Stroke Vasc Neurol Oct 202275415450 doi 10.1136/s · doi ↗ · pubmed ↗
- 5Interpretation of Annual Report on Cardiovascular Health and Diseases in China 2019 Cardiology Discovery 202114269284 doi 10.1097/CD 9.0000000000000040 · doi ↗
- 6Writing committee of the report on cardiovascular health and diseases in China Report on cardiovascular health and diseases in China 2021: an updated summary Biomed Environ Sci 07202022357573603 doi 10.3967/bes 2022.079Medline 35945174 · doi ↗ · pubmed ↗
- 7Guterman EL Douglas VC Shah MP Parsons T Barba J Josephson SA National characteristics and predictors of neurologic 30-day readmissions Neurology (E Cronicon)Feb 162016867669675 doi 10.1212/WNL.0000000000002379 Medline 26791149 · doi ↗ · pubmed ↗
- 8Kilkenny MF Longworth M Pollack M et al Factors associated with 28-day hospital readmission after stroke in Australia Stroke Aug 201344822602268 doi 10.1161/STROKEAHA.111.000531 Medline 23800558 · doi ↗ · pubmed ↗