Prevalence, Factors and Impact of Migraine on Healthcare Professionals: A cross-sectional study in the United Arab Emirates
Syyeda Maleha Jeelani, Shatha Al Sharbatti

TL;DR
This study found that 18% of healthcare workers in the UAE suffer from migraines, which significantly affect their quality of life and work performance.
Contribution
The study identifies specific risk factors for migraines among UAE healthcare professionals and quantifies their impact on work and quality of life.
Findings
Migraine prevalence among UAE healthcare professionals was 18.2%.
Migraine sufferers reported significantly higher disability and work impairment compared to non-sufferers.
Factors like stress, sleep deprivation, and food triggers were strongly associated with increased migraine risk.
Abstract
This study aimed to determine the prevalence of migraines among healthcare professionals (HCPs) in the United Arab Emirates (UAE), identify associated factors and evaluate their impact on quality of life (QoL) and work performance. This cross-sectional study was conducted from January to June 2022 and included nurses and doctors across 4 healthcare settings in the UAE. Migraine prevalence was assessed using the Migraine Screen Questionnaire, while its impact on social support and work function was evaluated through the Migraine Disability Assessment, the Oslo Social Support Scale and the Headache Impact Test. Data were analysed using Chi-square tests, binary logistic regression and multivariable logistic regression. A total of 440 nurses and doctors were included. Migraine prevalence among participants was 18.2%. The likelihood of experiencing migraines was significantly higher among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
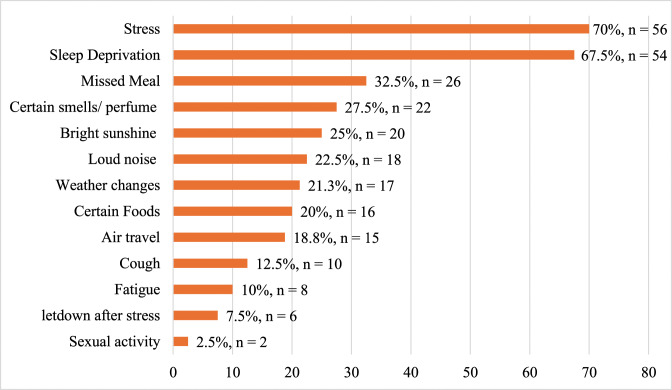 Fig. 1
Fig. 1| n (%) | |||
|---|---|---|---|
|
| |||
| Migraine | |||
|
| |||
| Characteristic | No | Yes | |
|
| |||
| <25 (n = 14) | 12 (85.7) | 2 (14.3) | 0.169 |
| 25–29 (n = 79) | 58 (73.4) | 21 (26.6) | |
| 30–34 (n = 80) | 65 (81.3) | 15 (18.8) | |
| 35–39 (n = 90) | 69 (76.7) | 21 (23.3) | |
| 40–44 (n = 59) | 53 (89.8) | 6 (10.2) | |
| 45–49 (n = 64) | 56 (87.5) | 8 (12.5) | |
| 50–54 (n = 19) | 17 (89.5) | 2 (10.5) | |
| 55–59 (n = 13) | 10 (76.9) | 3 (23.1) | |
| ≥60 (n = 22) | 20 (90.9) | 2 (9.1) | |
|
| |||
| Male (n = 107) | 98 (91.6) | 9 (8.4) | 0.003 |
| Female (n = 333) | 262 (78.7) | 71 (21.3) | |
|
| |||
| Southeast Asian region (n = 251) | 211 (84.1) | 40 (15.9) | 0.332 |
| Eastern Mediterranean region (n = 117) | 91 (77.8) | 26 (22.2) | |
| Other regions | 11 (84.6) | 2 (15.4) | |
|
| |||
| Single (n = 109) | 89 (81.7) | 20 (18.3) | 1.00 |
| Married (n = 327) | 267 (81.7) | 60 (18.3) | |
|
| |||
| 0 (n = 18) | 15 (83.3) | 3 (16.7) | 0.419 |
| 1 (n = 36) | 30 (83.3) | 6 (16.7) | |
| 2 (n = 39) | 29 (76.3) | 10 (23.7) | |
| ≥3 (n = 31) | 27 (87.1) | 4 (12.9) | |
|
| |||
| Yes (n = 113) | 74 (65.5) | 39 (34.5) | <0.001 |
| No (n = 325) | 285 (87.7) | 40 (12.3) | |
|
| |||
| Normal (18.5–24.9; n = 65) | 52 (80.0) | 13 (20.0) | 0.561 |
| Overweight (25–29.9; n = 48) | 42 (87.5) | 6 (12.5) | |
| Obese (≥30; n = 326) | 267 (81.9) | 59 (18.1) | |
| n (%) | |||
|---|---|---|---|
|
| |||
| Migraine | |||
|
| |||
| Characteristic | No | Yes | |
|
| 0.177 | ||
| Nurse (n = 308) | 247 (80.2) | 61 (19.8) | |
| Doctor (n = 132) | 113 (85.6) | 19 (14.4) | |
|
| 0.496 | ||
| General practitioner (n = 70) | 61 (87.1) | 9 (12.9) | |
| Specialist and consultant (n = 31) | 29 (93.5) | 2 (6.5) | |
|
| 0.058 | ||
| <40 (n = 9) | 8 (88.9) | 1 (11.1) | |
| 40–44 (n = 48) | 35 (72.9) | 13 (27.1) | |
| 45–49 (n = 54) | 41 (75.9) | 13 (24.1) | |
| 50–54 (n = 26) | 25 (96.2) | 1 (3.8) | |
| ≥55 (n = 17) | 16 (94.1) | 1 (5.9) | |
|
| <0.001 | ||
| Yes (n = 154) | 96 (62.3) | 58 (37.7) | |
| No (n = 286) | 264 (92.3) | 22 (7.7) | |
| n (%) | |||
|---|---|---|---|
|
| |||
| Migraine | |||
|
| |||
| Characteristic | No | Yes | |
|
| <0.001 | ||
| Yes | 69 (20.2) | 54 (67.5) | |
| No | 273 (79.8) | 26 (32.5) | |
|
| <0.001 | ||
| Not at all/very little | 306 (88.2) | 31 (38.8) | |
| Moderate/extremely high | 41 (11.8) | 49 (61.2) | |
|
| <0.001 | ||
| Poor/fair | 45 (12.8) | 25 (31.3) | |
| Good/excellent | 307 (87.2) | 55 (68.7) | |
| n (%) | |||
|---|---|---|---|
|
| |||
| Migraine | |||
|
| |||
| Characteristic | No | Yes | |
|
| 0.055 | ||
| Score 3–8 (poor social support) | 165 (46.0.) | 42 (52.5) | |
| Score 9–11 (moderate social support) | 110 (30.6) | 29 (36.3) | |
| Score 12–14 (strong social support) | 84 (23.4) | 9 (11.3) | |
|
| <0.001 | ||
| Little/no disability | 345 (96.6) | 57 (71.3) | |
| Mild/moderate/severe disability | 12 (3.4) | 23 (29.1) | |
|
| <0.001 | ||
| Little/no impact | 233 (65.4) | 23 (29.1) | |
| Some impact | 38 (10.7) | 7 (8.9) | |
| Substantial impact | 24 (6.7) | 6 (7.6) | |
| Severe impact | 61 (17.1) | 43 (54.4) | |
| Characteristic | COR | CI | AOR | CI | ||
|---|---|---|---|---|---|---|
|
| ||||||
| Male | 1 | 1 | ||||
| Female | 3.31 | 1.5–7.1 | 0.002 | 2.99 | 1.1–7.9 | 0.026 |
|
| ||||||
| Yes | 3.85 | 2.3–6.4 | <0.001 | 2.17 | 1.1–4.3 | 0.025 |
| no | 1 | 1 | ||||
|
| ||||||
| Yes | 11.13 | 6.4–19.3 | <0.001 | 5.87 | 2.9–11.8 | <0.001 |
| No | 1 | 1 | ||||
|
| ||||||
| Yes | 10.09 | 4.3–23.9 | <0.001 | 11.29 | 3.1–41.2 | <0.001 |
| No | 1 | 1 | ||||
|
| ||||||
| Yes | 9.59 | 5.5–16.7 | <0.001 | 4.38 | 1.9–9.8 | <0.001 |
| No | 1 | 1 | ||||
|
| ||||||
| Yes | 9.06 | 3.9–20.9 | <0.001 | 5.06 | 1.7–15.5 | 0.004 |
| No | 1 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies
1. Introduction
Migraine is one of the most prevalent neurological disorders, affecting approximately 12% of the global population. It ranks as the sixth leading cause of disability worldwide, reflecting its significant impact on quality of life (QoL) and productivity.^1^ Healthcare professionals (HCPs) are particularly vulnerable to migraines due to the demanding nature of their work, which often involves irregular shift rotations, prolonged working hours and high levels of emotional stress. A study by Kuo et al. in Taiwan highlighted that the risk of migraines is higher among physicians, nurses and other healthcare providers compared to the general population, with adjusted odds ratios (OR) of 1.672, 1.621 and 1.254, respectively.^2^ Similarly, research by Xie et al. revealed that 50% of medical staff reported headaches, with 25.9% experiencing migraines and 24.1% suffering from tension-type headaches.^3^ In Africa, Onwuekwe et al. found that 88% of HCPs reported experiencing headaches, further underscoring the occupational susceptibility of HCPs to this condition.^4^
Several factors have been associated with the development and exacerbation of migraines. For instance, women are more likely to experience migraines than men, a disparity linked to hormonal fluctuations that lower the migraine threshold, particularly during the premenstrual phase.^5^ Age also plays a significant role, with migraine prevalence peaking between 35 and 49 years and declining after the sixth or seventh decade of life. Early onset of migraines is strongly associated with a higher risk in first-degree relatives, particularly for migraines with aura, which exhibit a stronger hereditary predisposition than those without aura.^6^
The relationship between physical activity and migraines is complex and inconsistent. While exercise has been shown to alleviate comorbid conditions such as depression, anxiety and sleep disturbances – thereby boosting self-esteem and potentially reducing migraine symptoms – some individuals report that physical activity can trigger migraine episodes.^7^ This may explain the restricted physical activity often observed in migraine patients during interictal periods.^8^
Stress is one of the most frequently reported triggers for migraines.^9^ In a study conducted by Mollaoglu, a total of 126 migraine patients were questioned about suspected migraine triggers.^10^ Emotional stress (79%), sleep disturbances (64%) and dietary factors (44%) were identified as common triggers. Similarly, a large prospective study involving over 5,000 participants found a significant association between stress intensity and headaches in individuals with both migraine and tension-type headaches.^11^ Additionally, a systematic review has identified alcohol consumption, specific food items and fasting as common migraine triggers.^12^
Comorbid conditions, such as motion sickness, are closely linked to migraines. Both conditions exhibit similar symptoms, such as nausea and dizziness. This association is thought to arise from overlapping physiological disturbances.^13^
Despite the growing body of research on migraines globally, limited data exist regarding their prevalence among HCPs in the UAE. Understanding the prevalence, triggers and impact of migraines in this population is critical for developing targeted preventive measures and health promotion strategies to mitigate their burden. The present study aimed to assess the prevalence of migraines, identify factors associated with migraine attacks and evaluate the impact of migraines on HPCs in the UAE.
2. Methods
This cross-sectional study included doctors and nurses from 4 hospitals in the UAE. Data were collected between January and June 2022. Participants included individuals of any nationality and gender who provided informed consent. The sample size was calculated using the following formula:
Where, n represents the sample size and p denotes the estimated prevalence of migraine among HCPs, which was assumed to be 50% based on a previous study.^3^ The variable q indicates the estimated prevalence of non-migraine cases among HCPs, with a 95% confidence level and a precision level (d value) set at 5% (0.05). The calculated sample size was 400; however, to account for a potential 10% refusal rate, an additional 40 participants were included, resulting in a total target sample size of 440. Participants were recruited using convenience sampling.
A self-administered questionnaire was used to collect data on sociodemographics, lifestyle factors, self-reported weight and height and job characteristics. The questionnaire underwent content validation by 3 experts. Migraine prevalence was assessed using the Migraine Screen Questionnaire (MS-Q), a standardised tool comprising 5 yes/no questions, where a score of ≥4 indicated a possible migraine.^14^ To evaluate the impact of migraines, 3 additional standardised tools were employed: the Migraine Disability Assessment Test (MIDAS), the Oslo Social Support Scale (OSSS-3) and the Headache Impact Test (HIT-6).^151617^ The MIDAS assessed the impact of headaches, with scores categorised as follows: 0–5 (minimal or no disability, grade 1), 6–10 (mild disability, grade 2), 11–20 (moderate disability, grade 3) and 21+ (severe disability, grade 4). The HIT-6 measured the impact of headaches on job performance, home activities and social situations, with total scores ranging from 36–78, categorised as little or no impact (≤49), some impact (50–55), substantial impact (56–59) and severe impact (≥60).^17^ The OSSS-3 evaluated social support, with scores of 3–8 indicating poor support, 9–11 suggesting moderate support and 12–14 signifying strong support.^16^
Data were analysed using the Statistical Package for the Social Sciences (SPSS), Version 27 (IBM Corporation, Armonk, New York, USA), and the results were presented in tables, figures and text format. The Chi-square test was used to assess associations between variables, while both binary and multivariable regression analyses were conducted to identify predictors of migraine.
3. Results
A total of 440 participants (response rate = 96%) were included; most were female (75.7%), married (75.0%) and aged between 22 and 64 years, with the highest percentage (20.4%) in the 35–39 age group. Most participants had 1 or 2 children (60.4%) and reported no family history of migraine (74.2%). Additionally, the majority were from the World Health Organization (WHO) Southeast Asian region (65.9%), while 5.7% (n = 25) were UAE nationals and 94.3% (n = 415) were non-nationals [Table 1].
Nurses constituted 70% of the participants, with most doctors being general practitioners (GPs; 69.3%). The proportion of participants who worked over 50 hours per week was 27.9% [Table 2]. Regarding body mass index (BMI), 74.3% were classified as obese, 10.9% were overweight and 14.8% had normal BMI levels.
The prevalence of migraine, as assessed using the MS-Q, was found to be 18.2%. Among those with migraines (n = 80), 23.5% reported the onset of their condition before the age of 20, while 54.9% experienced onset between 20 and 29 years, 13.7% between 30 and 39 years and only 7.9% at or after 40 years of age. No significant associations were observed between migraines and smoking (P = 0.313), physical activity (P = 0.299) or BMI (P = 0.561). Among participants identified as likely migraineurs by the MS-Q, 35% (n = 28) reported that they had not been previously diagnosed by a doctor, while no diagnosed cases were identified in the group classified as non-migraineurs by the MS-Q.
Stress has been identified as the most common migraine trigger, while least reported sexual activity as a trigger [Fig. 1]. The results revealed that migraine prevalence was significantly higher in females and those with a family history of the condition. However, no significant associations were found between migraines and age, nationality, marital status, number of children, or BMI [Table 1]. The prevalence of migraines among UAE nationals was higher than that among non-nationals (28% versus 17.6%), but this difference was not statistically significant (P = 0.196).
Factors that triggered migraine in the current study.
There was a significant association between migraines and the perceived negative impact on work. Migraine prevalence was higher among nurses compared to doctors and among GPs compared to specialists and consultants. However, no significant association was found between migraines and job speciality or weekly working hours. A higher prevalence of migraines was observed among participants working 40–49 hours per week [Table 2].
Sleep disturbances were found to be significantly more prevalent among participants identified as having migraines. A significant association was found between migraines and a poorer QoL, with affected participants more commonly reporting their general health as poor or fair compared to the non-migraine respondents [Table 3].
Factors such as inadequate social support, varying levels of disability and a greater impact on the ability to function at work, home and in social situations were more common among participants with migraines [Table 4].
Predictors such as gender, family history, stress, certain foods, sleep deprivation and motion sickness have been shown to increase the likelihood of migraines [Table 5].
Regarding migraine treatment challenges and management, participants were asked about their strategies for relieving migraine headaches. The results showed that 41% used 1–3 medications, 32% used 4 or more medications and 26.9% relied on non-pharmacological approaches such as sleeping, massage or resting in a dark, quiet room.
4. Discussion
To the best of the authors' knowledge, there is limited data from the UAE addressing the social and work-related impacts of migraines. This study contributes to the existing literature by exploring less examined dimensions and identifying potential interventions to improve individual QoL and workforce productivity. The present study found that the migraine prevalence was 18.2%, which is significantly lower than the 50% reported by Xie et al.^3^ Additionally, 54.9% of participants reported the onset of migraines during their third decade of life, contrasting with findings from another study where migraine onset was more common in the second decade.^18^
No significant association was found between doctors' specialities and migraine prevalence, which contrasts with a German study that reported significantly higher migraine rates among headache specialists. This discrepancy may be attributed to selection bias, as doctors who experience migraines might be more likely to specialise in this field.^19^ The current study also revealed a higher prevalence of migraines among younger participants (25–29 years) compared to older participants (≥60 years), with rates of 26.6% and 9.1%, respectively; however, this difference was not statistically significant. This finding aligns with Xie et al., who observed higher migraine prevalence in the 20–29 age group compared to those aged ≥40 years (27.1% versus 11.5%).^3^
The current study revealed a significantly higher prevalence of migraines among females compared to males (21.3% versus 8.4%). This finding is consistent with Rossi et al.'s study, who reported a global prevalence of 20.7% in females and 9.7% in males.^20^ This disparity may be attributed to both biological and social factors, including the dual responsibilities of caregiving and professional work that women more frequently bear. Such findings emphasise the importance of gender-specific approaches in migraine research, prevention and management. In this study, females had a 2.99 times higher risk of experiencing migraines compared to males, which aligns with findings from a Chinese study (OR = 2.314).^3^
No significant differences in migraine prevalence were observed among participants from different WHO regions, suggesting that geographic variation may be influenced by racial and environmental factors.^21^ Similarly, no statistical differences were found in migraine prevalence between married and single participants, which is consistent with studies conducted by Alturaiki et al. and Almalki et al. in Saudi Arabia.^2223^
Migraine prevalence was significantly higher among participants with a family history of the condition (34.5% versus 12.3%), consistent with the findings of Almalki et al., which reported prevalence rates of 64% and 36% for participants with and without a family history, respectively.^23^ No associations were observed between migraine and smoking or physical activity, which aligns with findings from another study.^22^
Sleep disturbances are more prevalent among migraineurs, with sleep deprivation increasing the risk of migraine by 4.38 times. This finding aligns with Kim et al., who reported poor sleep quality in 47.6% of migraine sufferers compared to 21.0% in non-migraine populations.^24^ Although the connection between sleep disturbances and migraines remains unclear, shared anatomical regions or biochemical mediators, such as serotonin and melatonin, may contribute to this relationship.^25^
Migraine prevalence was higher among nurses compared to doctors (19.8% versus 14.4%); however, this difference was not statistically significant. The findings regarding migraine prevalence among healthcare providers are inconsistent. Kuo et al. found that nurses had a higher risk of migraines (OR = 1.693).^2^ Conversely, another study showed a non-significant difference in migraine prevalence between female doctors and nurses (32.4% versus 29.8%).^3^
Stress was the most frequently reported migraine trigger, increasing the likelihood of their occurrence by 5.87 times. This finding aligns with existing evidence that links stress to migraine development.^26^ Sleep deprivation was identified as the second most common trigger, with both stress and sleep deprivation potentially exacerbating one another due to shared pathophysiological mechanisms.^25^ Dietary factors were reported in 20% of cases and were associated with an increased risk of migraines; however, the wide confidence interval observed reflects variability in the findings. Previous systematic reviews have similarly highlighted inconsistencies, although specific food items have been more commonly linked to migraine attacks.^12^ Variability in the effects of dietary factors may explain the inconsistencies observed in this study. Motion sickness was also found to elevate the likelihood of migraines, which is consistent with previous research.^13^
The perceived burden of headaches on participants' QoL and general health was significant, aligning with studies conducted in Malaysia and Saudi Arabia.^2728^ The current study demonstrated a substantial perceived impact of migraines on work and social life, with 29.1% of migraine sufferers experiencing varying levels of disability as measured by the MIDAS scale. This figure is lower than the 57.5% reported in the USA, possibly due to differences in population demographics.^29^ Furthermore, 54.4% of participants with migraines reported severe impacts on their daily life and work, as assessed by the HIT-6, a percentage notably higher than the 23% reported in Korea.^30^
Approximately one-third of migraine sufferers in the current study were either unaware of their condition or lacked access to proper diagnostic care, which likely explains the significant impact migraines had on their work and social lives. These findings highlight the urgent need for policy initiatives aimed at improving migraine screening tools and providing workplace and social support for affected individuals.
The findings regarding migraine medications raise concerns about the increased risks of drug interactions, side effects and the overall treatment burden faced by migraine patients. Further research is needed to clarify the factors driving polypharmacy in this population and to develop targeted interventions.
This study has some limitations, including the inability to generalise the findings due to the convenience sampling method used, which involved recruiting participants from only 4 healthcare facilities. Additionally, recall bias and missing information for certain variables may have influenced the results.
5. Conclusion
This study's findings underscore the need for targeted interventions, including the development of workplace policies and support systems, to mitigate the risk and impact of migraines on HCPs. With nearly 20% of participants identified as migraine sufferers and a severe impact reported in most cases, future research should focus on examining the effectiveness of novel drugs in reducing the burden of migraines within this population.
Authors' Contribution
Syyeda Maleha Jeelani: Conceptualization, Methodology, Investigation, Formal analysis, Writing - Original Draft. Shatha Al Sharbatti: Conceptualization, Methodology, Formal analysis, Writing - Review & Editing.
Ethics Statement
The study received ethical approval from the Gulf Medical University's Institutional Review Board (IRB/COM/STD/08/Jan-2022) and the UAE Ministry of Health and Prevention Ethics Committees (MOHAP/DXB-REC/ F.M.M/No. 18/ 2022). All participants provided informed consent, and data confidentiality was ensured, with access restricted to the research team and Ethics Committee members.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Migraine and other headache disorders. From: https://www.who.int/en/news-room/fact-sheets/detail/headache-disorders Accessed: Nov 2024.
- 2Kuo WY Huang CC Weng SF Lin HJ Su SB Wang JJ. Higher migraine risk in healthcare professionals than in general population: A nationwide population-based cohort study in Taiwan. J Headache Pain 2015; 16:102. https://doi.org/10.1186/s 10194-015-0585-6.10.1186/s 10194-015-0585-626631235 PMC 4668247 · doi ↗ · pubmed ↗
- 3Xie W Li R He M Cui F Sun T Xiong J. Prevalence and risk factors associated with headache amongst medical staff in South China. J Headache Pain 2020; 21:5. https://doi.org/10.1186/s 10194-020-1075-z.10.1186/s 10194-020-1075-z 31937239 PMC 6961346 · doi ↗ · pubmed ↗
- 4Onwuekwe I Onyeka T Aguwa E Ezeala-Adikaibe B Ekenze O Onuora E. Headache prevalence and its characterization amongst hospital workers in Enugu, South East Nigeria. Head Face Med 2014; 10:48. https://doi.org/10.1186/1746-160X-10-48.10.1186/1746-160X-10-4825423879 PMC 4289241 · doi ↗ · pubmed ↗
- 5Vetvik KG Mac Gregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol 2017; 16:76–87. https://doi.org/10.1016/S 1474-4422(16)30293-9.10.1016/S 1474-4422(16)30293-927836433 · doi ↗ · pubmed ↗
- 6Eidlitz-Markus T Haimi-Cohen Y Zeharia A. Association of age-at-onset of migraine with family history of migraine in children attending a pediatric headache clinic: A retrospective cohort study. Cephalalgia 2015; 35:722–7. https://doi.org/10.1177/0333102414554114.10.1177/033310241455411425304765 · doi ↗ · pubmed ↗
- 7Daenen L Varkey E Kellmann M Nijs J. Exercise, not to exercise, or how to exercise in patients with chronic pain? Applying science to practice. Clin J Pain 2015; 31:108–14. https://doi.org/10.1097/AJP.0000000000000099.10.1097/AJP.000000000000009924662498 · doi ↗ · pubmed ↗
- 8Irby MB Bond DS Lipton RB Nicklas B Houle TT Penzien DB. Aerobic exercise for reducing migraine burden: Mechanisms, markers, and models of change processes. Headache 2016; 56:357–69. https://doi.org/10.1111/head.12738.10.1111/head.1273826643584 PMC 4813301 · doi ↗ · pubmed ↗