Schwannoma of the Appendix Mimicking a Metastatic Breast Cancer: A case report
Zaid Al-Ishaq, Alonood Al-Sulaimani, Badriya S. Al-Qassabi, Fathiya AlRahbi, Khalid Al Baimani, Jawa Z. Muhammad, Adil Aljarrah

TL;DR
A 55-year-old woman with breast cancer was found to have a benign tumor in her appendix, not cancer, highlighting the need for careful diagnosis.
Contribution
This case highlights the importance of histopathological confirmation in suspected metastatic breast cancer.
Findings
Radiological findings suggested appendix metastasis, but it was a schwannoma.
Histopathological confirmation is crucial for accurate diagnosis in breast cancer staging.
Abstract
Metastatic breast cancer (MBC) represents 5–10% of newly diagnosed breast cancer cases, referred to as de novo stage IV MBC. Distinguishing a distant lesion in breast cancer patients can be challenging. Therefore, obtaining a histopathological confirmation of a metastasis is advisable, as a suspicious metastatic lesion may be benign or exhibit different immunohistochemistry compared to the primary site. We report a 55-year-old female patient who presented to a tertiary care hospital in Muscat, Oman in 2019. The patient was undergoing staging scans for newly diagnosed breast cancer, where radiological findings suggested appendix metastasis. However, subsequent laparoscopic appendicectomy revealed an appendicular schwannoma, confirmed through immunohistochemistry. The patient received curative-intent breast cancer treatment. With the increasing use of advanced staging scans in breast…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
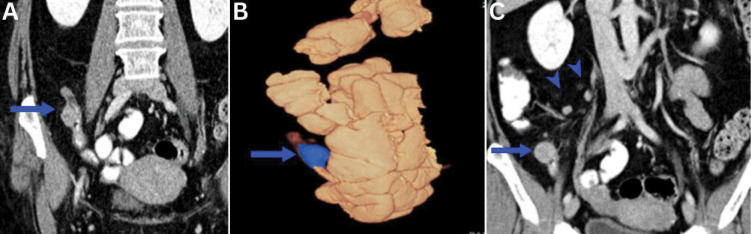 Fig. 1
Fig. 1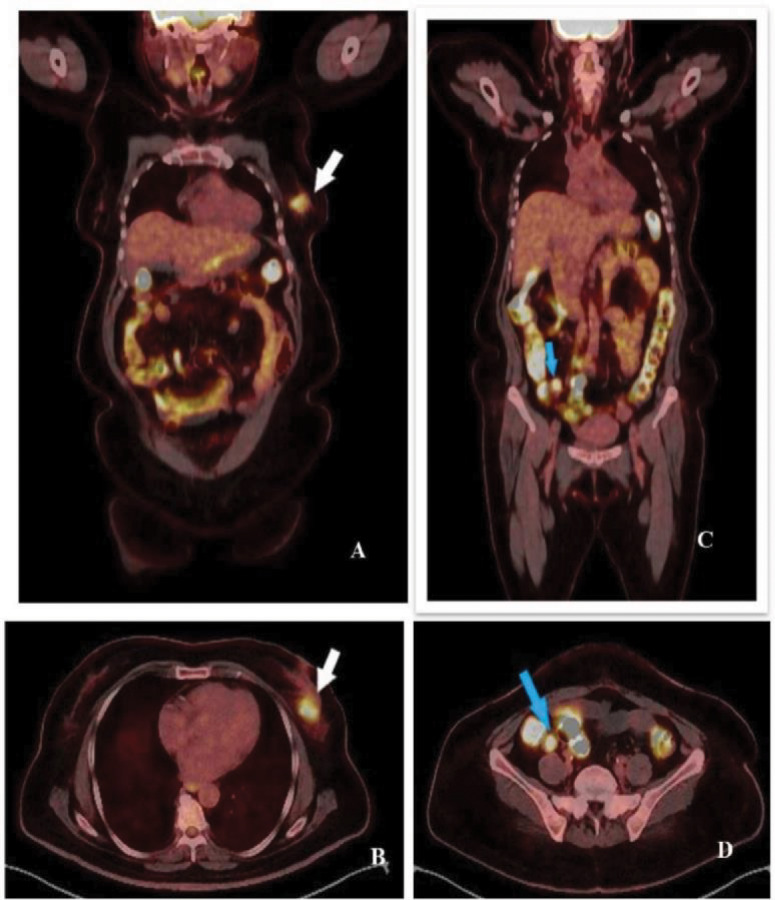 Fig. 2
Fig. 2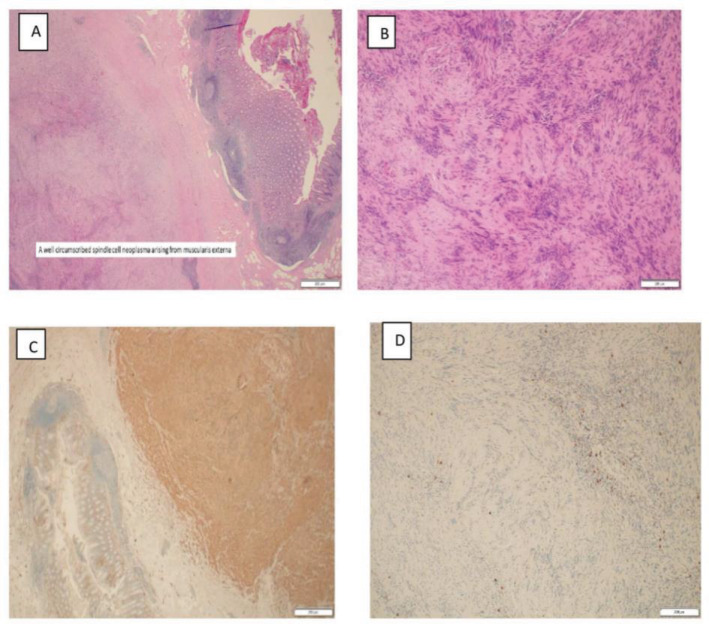 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Gastrointestinal Tumor Research and Treatment · Neuroendocrine Tumor Research Advances
1. Introduction
Metastatic breast cancer (MBC), also known as de novo stage IV MBC, represents 5–10% of newly diagnosed breast cancer (BC) cases in Western countries and 13% in Oman.^12^ Gastrointestinal (GI) tract metastases from BC are infrequent, reported in autopsy series with varying incidence (8–35%).^3^ Distinguishing distant lesions in breast cancer patients can be challenging, impacting treatment decisions reliant on disease stage.^45^ Hence, histopathological confirmation is advisable as suspicious metastatic lesions may prove benign or exhibit different immunohistochemistry compared to the primary site.^6^ This case report describes an appendicular schwannoma mimicking metastatic breast cancer. Schwannomas are the most common type of peripheral nerve tumours and rarely affect the GI system, often being diagnosed incidentally. Diagnosis is confirmed through histopathology and immunohistochemistry. Total surgical excision is the recommended treatment for GI schwannoma.
2. Case report
A 55-year-old female patient presented at a one-stop breast clinic in a tertiary care hospital in Muscat, Oman in 2019 with a one-month history of a left breast lump with no other symptoms. The patient had a history of type 2 diabetes mellitus and hypertension, managed with regular medication, with no relevant family history. On examination, a 3 cm ill-defined, hard, mobile lump was noted in the upper outer quadrant of the left breast. Breast ultrasonography revealed an irregular hypoechoic lesion measuring 2.9 × 1.7 cm in the left breast at 3 o'clock position, with microcalcifications within. Left axillary ultrasound indicated a suspicious lymph node measuring 6.6 mm. Mammogram showed asymmetric density in the left breast classified as Breast Imaging-Reporting and Data System 5. True cut biopsy confirmed invasive ductal carcinoma (IDC) with negative oestrogen and progesterone receptors, positive HER2, and a Ki67 of 45%. Fine needle aspiration cytology from the left axillary lymph node was negative for metastasis.
During staging workup, contrast-enhanced computed tomography (CE-CT) scans revealed 2 subserosal nodules in the appendix and prominent mesenteric lymph nodes in the right iliac fossa [Fig. 1]. A positron emission tomography scan (PET) indicated a hypermetabolic left breast mass (standardised uptake value [SUV] maximum 17.8) and suspicious metastatic lesion in the appendix (SUV maximum 21.5) [Fig. 2].
Selected contract enhanced computed tomography images of the abdomen of a 55-year-old female patient showing (A,B,C) contract filled appendix with 2 eccentric nodular wall thickening (arrows are pointing to the largest one). There are prominent adjacent regional mesenteric lymph nodes (arrowheads) (C).
Fluorodeoxyglucose (FDG)-18 positron emission tomography-computed tomography scan, showing (A & B) the primary left breast cancer (standardised uptake value [SUV] max 17.8) (white arrow) with (C & D) an FDG avid left appendix mass (SUV max 21.5) (blue arrow).
In a multidisciplinary meeting, consensus favoured evaluating the appendicular lesion before initiating breast cancer treatment. Diagnostic colonoscopy showed no abnormality. Subsequently, the patient underwent laparoscopic appendectomy to determine the exact nature of the appendicular lesion.
Pathological examination revealed a well-demarcated tumour at the appendix tip, composed of spindle-shaped cells proliferating in a bundle from the muscularis externa [Figure 3A]. The tumour displayed classic schwannoma features, including spindle cell morphology, nuclear palisading and Verocay bodies [Figure 3B]. Vascular invasion and lymph duct invasion were absent. Immunohistochemical studies confirmed S-100 protein positivity and negativity for CD117, DOG-1, CD34, SMA, Desmin, AE1/3, CAM5.2, B-Catenin, ALK-1, c-KIT and CD34, confirming the appendicular schwannoma diagnosis [Figure 3C and D].
Haemotoxylin and eosin stains showing (A) spindle-shaped heterotypic cells proliferating in a bundle at ×20 magnification. Tumour showing (B) features of a schwannoma including spindle cell morphology, nuclear palisading and Verocay bodies at ×10 magnification. In immunohistochemical studies, tumour cells were (C) diffusely positive S-100 protein and (D) negative for CD117 at ×20 magnification.
Following the exclusion of metastatic disease, the patient commenced neoadjuvant chemotherapy based on anthracycline, taxane and dual Her2 blockades. Subsequent left breast image-guided wide local excision and sentinel lymph node biopsy revealed a pathological complete response. Adjuvant radiotherapy and 18 cycles of trastuzumab every 3 weeks were administered. The patient also received alendronate and calcium with vitamin D for osteopenia in addition to her regular medications. It should be noted that the patient underwent comprehensive panel of gene testing, including neurofibromatosis (NF)1 and NF2, but no responsible gene was detected.
3. Discussion
In the current case, a staging CE-CT scan revealed an appendicular lesion confirmed as suspicious for metastasis on PET scan. However, differential diagnoses include gastrointestinal stromal tumours (GISTs) and solitary neuroendocrine tumours. Occasionally, lymphomas and GI adenocarcinomas may mimic mesenchymal tumors.^7^
Fluorodeoxyglucose (FDG)-positron emission tomography is effective in detecting malignant tumours. However, FDG accumulation has been noted in schwannomas, making it challenging to differentiate them from distant metastases through imaging alone.^8^ Furthermore, the discordance rates in biomarkers between primary tumours and metastatic disease emphasise the importance of histopathological assessment. Studies have reported hormone receptor discordance rates ranging from 30–40% and HER-2/neu discordance rates ranging from 10–30%.^9^ These findings highlight the importance of histopathological confirmation of suspicious appendicular lesions before starting treatment. This approach led to the consideration of laparoscopic appendectomy in the current case, resulting in the diagnosis of appendicular schwannoma, and the breast cancer was treated with curative intent.
Schwannoma is a rare mesenchymal tumour affecting the GI tract, primarily observed in the stomach and often diagnosed incidentally.^10^ Appendiceal schwannoma, an exceptionally rare variant, has been documented in only 15 cases in the existing literature; definitive characteristic findings are yet to be established.^11^ Clinical presentations vary, ranging from asymptomatic cases to appendicitis-like abdominal pain. Notably, perforation is an exceedingly rare occurrence.^12^
On histology, schwannomas are typically composed of spindle cells that stain strongly positive for S100 and focally for GFAP and CD57 on immunohistochemistry. These findings are sufficient to confirm the diagnosis in the absence of KIT positivity and smooth muscle markers.^10^ While schwannoma and GIST have similar histological findings in that they both demonstrate a spindle-like proliferation, they have distinct immunohistochemistry staining. Greater than 95% of GISTs express c-Kit (CD117), CD34 (70%) and H-caldesmon (80%).^10^
Levy et al. described the radiological features of histopathologically proven schwannomas as well-defined homogeneously attenuating mural masses on CT. They lack the poor prognostic factors seen typically in GISTs such as low attenuating haemorrhage, necrosis or degradation within the tumor.^13^ Furthermore, Suzuki et al. highlighted the radiological findings of peritumoral lymph node swelling as a potential differentiator for schwannoma compared to other appendicular tumours, serving as a valuable diagnostic clue. This lymphadenopathy may be linked to cytokine release from tumour cells, inducing chemokinesis of lymphocytes.^14^ Coincidentally, the radiological findings of the current patient align with known patterns as described by Suzuki et al. Nonetheless, additional research on the diagnostic characteristics of schwannoma is warranted.
For confirmed GI schwannomas, complete surgical excision is the recommended approach, while partial excision may be considered for large tumours posing a risk of nerve damage. It is noteworthy that even with partial excision, the occurrence of malignant transformation remains extremely rare.^10^
4. Conclusion
The current case highlights the importance of maintaining a broad spectrum of differential diagnoses and obtaining histopathological confirmation when identifying lesions during staging scans in patients with breast cancer. This approach not only confirms the diagnosis but also ascertains immunophenotypes to enable the selection of the most suitable subsequent therapy.
Ethical Statement
Patient consent was obtained for publication purposes.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
ZA, AA-S, BSA, FA and JZM contributed to writing the initial draft of the manuscript and critical review. KAB and AA contributed to the critical review All authors approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barcenas CH Song J Murthy RK Raghavendra AS Li Y Hsu L. Prognostic model for de novo and recurrent metastatic breast cancer. JCO Clin Cancer Inform 2021; 5:789–804. https://doi.org/10.1200/CCI.21.00020.10.1200/CCI.21.0002034351787 PMC 8807018 · doi ↗ · pubmed ↗
- 2Ministry of Health, Sultanate of Oman. Oman Cancer Incidence Report 2020. From: https://www.moh.gov.om/media/qqkfk 1u 4/cancer-incidence-in-oman-2020.pdf. Accessed: May 2024.
- 3Di Micco R Santurro L Gasparri ML Zuber V Fiacco E Gazzetta G. Rare sites of breast cancer metastasis: A review. Transl Cancer Res 2019; 8:S 518–52. https://doi.org/10.21037/tcr.2019.07.24.10.21037/tcr.2019.07.2435117130 PMC 8797987 · doi ↗ · pubmed ↗
- 4Paek SH Woo J Woo KJ Kim KC Lim W. Pleural Schwannoma Suspected as Metastasis of Breast Cancer. Am J Case Rep 2020; 21:e 921548. https://doi.org/10.12659/AJCR.921548.10.12659/AJCR.92154832214059 PMC 7138886 · doi ↗ · pubmed ↗
- 5Trayes KP Cokenakes SEH. Breast Cancer Treatment. Am Fam Physician 2021; 104:171–8.34383430 · pubmed ↗
- 6Simmons C Miller N Geddie W Gianfelice D Oldfield M Dranitsaris G. Does confirmatory tumor biopsy alter the management of breast cancer patients with distant metastases? Ann Oncol 2009; 20:1499–504. https://doi.org/10.1093/annonc/mdp 028.10.1093/annonc/mdp 02819299408 PMC 2731014 · doi ↗ · pubmed ↗
- 7Kang HC Menias CO Gaballah AH Shroff S Taggart MW Garg N. Beyond the GIST: Mesenchymal tumors of the stomach. Radiographics 2013; 33:1673–90. https://doi.org/10.1148/rg.336135507.10.1148/rg.33613550724108557 PMC 3794320 · doi ↗ · pubmed ↗
- 8Kumagai H Takehana K Shioi Y Tono C. Axillary schwannoma mimicking lymph node metastasis-associated breast cancer: A case report. Surg Case Rep 2022; 8:135. https://doi.org/10.1186/s 40792-022-01493-8.10.1186/s 40792-022-01493-835844031 PMC 9288938 · doi ↗ · pubmed ↗