The Relationship between Female Genital Mutilation and Infertility: A systematic review and meta-analysis
Narges S. Soltani, Farahnaz Heshmat, Mohsen Dehghani, Robab L. Roudsari, Mohadese B. Ghalibaf, Samira E. Zagami

TL;DR
This study reviews the link between female genital mutilation and infertility, finding a higher but not statistically significant risk of infertility among circumcised women.
Contribution
The study provides a systematic review and meta-analysis of FGM's association with infertility, highlighting the need for eradicating the practice.
Findings
Female circumcision was associated with a 21% higher odds of infertility, though not statistically significant.
No significant heterogeneity was found among the included studies.
The study emphasizes the importance of eliminating female genital mutilation to prevent potential infertility risks.
Abstract
This systematic review aimed to investigate the relationship between female genital mutilation (FGM) and infertility. Online databases were systematically searched up to January 2024 using MeSH keywords to retrieve relevant observational studies. The methodological quality of the analytical cross-sectional studies was assessed using the Newcastle–Ottawa Scale. Pooled odds ratios (OR) with 95% confidence intervals (CI) were calculated, and a random-effects meta-analysis was used to address any heterogeneity. Additionally, a sensitivity analysis was performed. A total of 5 analytical cross-sectional studies involving 37,146 participants, with 3 studies meeting the criteria for the meta-analysis. The results indicated that female circumcision (FC) was linked to a 21% increase in the odds of developing infertility compared to non-circumcision, although this finding was not statistically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
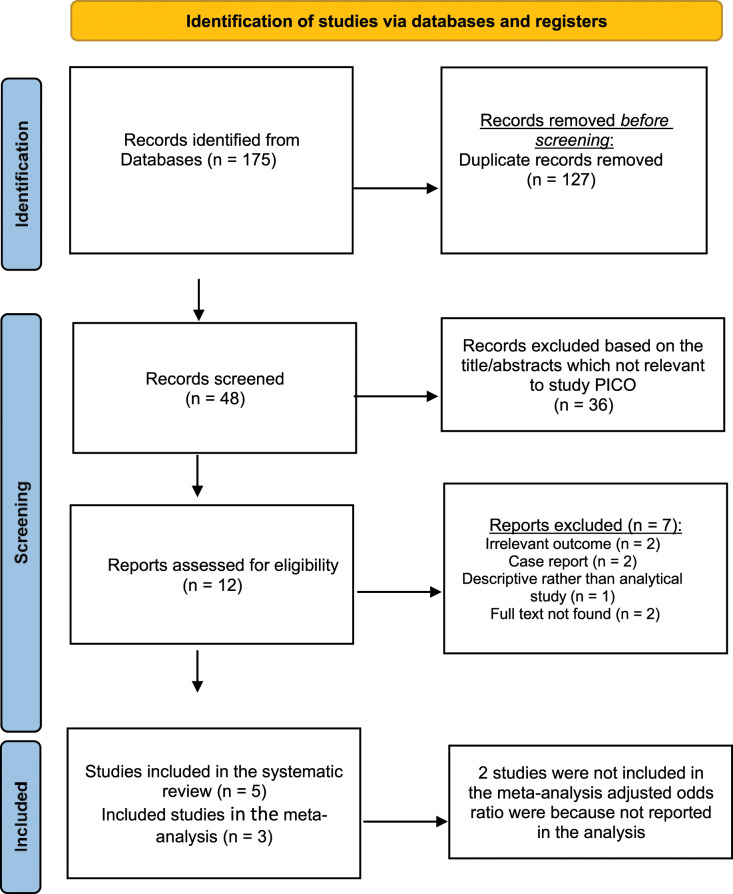 Fig. 1
Fig. 1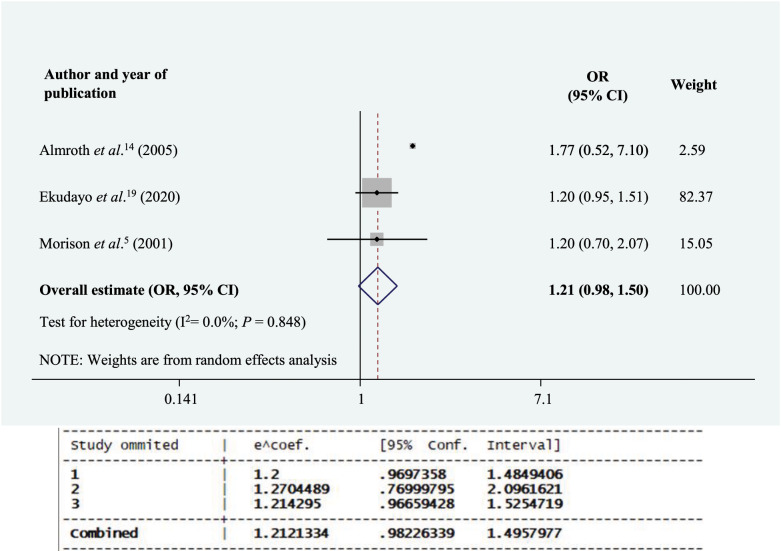 Fig. 2
Fig. 2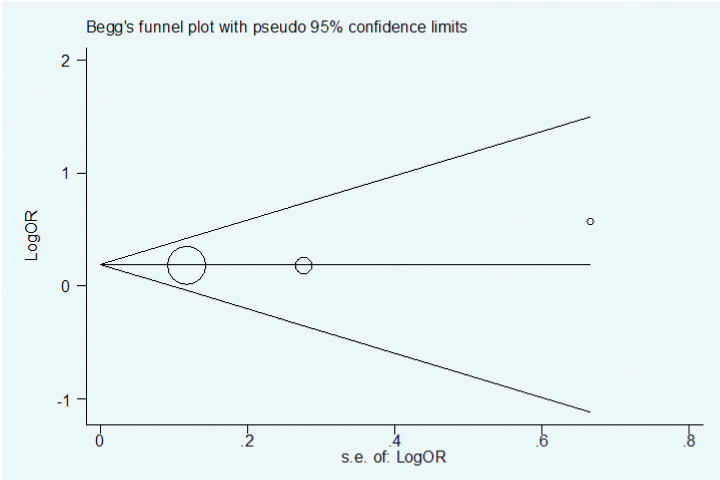 Fig. 3
Fig. 3| Author and year of publication | Country | Age in years | Type of study | Study population and no. of participants | Type of female circumcision | Results |
|---|---|---|---|---|---|---|
| Almroth | Sudan | 18–35 | Case-control | Cases: n = 99 women with primary infertility Control: n = 180 | Type I: 19 (7%) Type II: 9 (3%) Type III: 243 (87%) | FGM was not significantly associated with primary infertility. Adjusted OR = 1.77 (95% CI: 0.52–7.10) based on WHO classification of FGM ( |
| Ekudayo | Nigeria | 15–49 | Cross- sectional | N = 16,922 women of reproductive age | – | It revealed a non-significant higher (19%) likelihood of infertility occurrence among uncircumcised women than their circumcised counterparts (adjusted OR = 0.83, 95% CI: 0.65–1.05; |
| Larsen and Yan | Central Africa, Côte d’Ivoire, Tanzania | 20–44 | Longitudinal survey | N = 16,361 women | – | Female circumcision was not associated with increased infertility nor with reduced fertility in the Central African Republic, Côte d’Ivoire and Tanzania. |
| Morison | Gambia | 15–54 | Cross-sectional | N = 1,348 women | Most common form is Type II excision | Infertility was not significantly more common in cut women (Adjusted OR = 1.20, 95% CI: 0.70–2.07; |
| Yount and Carrera | Egypt | 17–55 | Longitudinal survey | N = 2,236 circumcised women | Most common form is Type II excision (73% among circumcised women) | Type of circumcision is not associated with adverse fertility outcomes among circumcised women (type 1: OR = 0.92; type 2: OR = 1.01). |
| Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
| ||||||
| Author and year of publication | Representativeness of the sample | Sample size | Non- respondents | Ascertainment of the exposure | Comparability of the subjects in outcome groups on the basis of design or analysis | Assessment of the outcome | Appropriateness of the statistical test | Study score |
| Almroth | – | + | – | + | + | + | + | 5/7 |
| Ekudayo | – | + | + | + | + | + | + | 6/7 |
| Larsen and Yan | – | – | – | + | + | + | + | 4/7 |
| Morison | – | + | – | + | + | + | + | 5/7 |
| Yount and Carrera | – | + | – | + | + | + | + | 5/7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFemale Genital Mutilation/Cutting Issues
1. Introduction
Female circumcision (FC), also known as female genital mutilation (FGM), is defined by the World Health Organization (WHO) as “all procedures that involve partial or total removal of the external female genitalia or other injury to the female genital organs”, typically for cultural or non-therapeutic reasons.^12^ The WHO has categorised this practice into 4 main types based on the extent of the cutting. FGM-I refers to the partial or total removal of the clitoris along with the prepuce; FGM-II involves the partial or total cutting of the clitoral glans along with the labia minora, with or without the removal of the labia majora; FGM-III entails the removal of both the labia minora and majora, or just the latter, with or without the clitoris; and FGM-IV includes practices such as piercing, pricking, and cauterisation of the genital area.^3^
This ancient cultural tradition, prevalent in many African and Asian societies, has recently garnered significant attention from policymakers, activists and professionals across various fields.^45^ Widely recognised as a form of violence against women and girls, FGM is considered a violation of their fundamental rights and a manifestation of gender inequality, inflicting severe harm on women's sexual health and overall well-being.^57^ FGM is associated with significant morbidity and mortality, with no documented medical benefits.^89^ The severe complications of FGM include acute pain, haemorrhage, childbirth complications, urinary incontinence, cysts, sexual dysfunction and infertility.^911^
Infertility, defined as the inability of a couple to conceive after 12 months or more of unprotected intercourse, is a critical reproductive health issue in developing countries and affects an estimated 10% to 12% of couples worldwide.^12^
The relationship between FGM and infertility is a complex and often debated topic. The tissue damage caused by FGM, combined with the risk of microbial contamination during the procedure, may increase the risk of vaginal infections. In prepubertal girls, the low oestrogen environment makes the atrophic vaginal epithelium particularly susceptible to bacterial invasion, especially since the lack of vaginal acidity before puberty allows such infections to thrive. In the absence of a protective environment, these infections may ascend to the uterus and fallopian tubes, leading to tubal damage and subsequent infertility.^14^ Additionally, FGM can result in the accumulation of menstrual blood and pelvic inflammatory disease, both of which are linked to infertility.^15^
Despite the numerous complications associated with FGM, the issue of reduced fertility and infertility has received relatively little attention.^16^ A previous study found that only 5 out of 198 studies explored infertility as a socioeconomic consequence of FGM in women. All but 1 of these studies found a link between FGM and infertility, particularly among women who had undergone infibulation or experienced FGM-III.^17^
One study estimated that 20% to 25% of infertility cases in Sudan were attributable to FGM.^15^ Despite extensive research on the physical and psychological effects of this practice, its impact on fertility remains controversial. Aziz reported that 2.2% of 7,505 Sudanese women who had undergone FGM had experienced infertility lasting 2 or more years. In 60% of these cases, the procedure had been performed in a way that prevented full penetration, making pregnancy impossible.^18^ In contrast, Ekudayo et al. found a higher likelihood of unexplained infertility among uncircumcised women compared to their circumcised counterparts.^19^ Furthermore, Morison et al. found no significant association between FGM and infertility.^5^
Given the conflicting findings in existing research and the lacuna of a comprehensive systematic review on this topic, this systematic review and meta-analysis aimed to examine the relationship between FGM and infertility. By synthesising the results of previous studies, this review provides a clearer understanding of the potential effects of FGM on female infertility.
2. Methods
The Meta-analysis of Observational Studies in Epidemiology guideline was adopted to conduct and report the present systematic review and meta-analysis of observational studies.^20^
2.1. Search strategy
A comprehensive literature search was conducted to retrieve the observational studies (viz., cohort, cross-sectional and case-control ones) on the association between FGM and infertility from database inception date to January 2024. The search was based on the PECO framework, namely, Participants (P) were circumcised women; Exposure (E)was FGM; comparison group (C) was the general population (or uncircumcised women); and Outcome (O) was infertility. The search was carried out on online databases, including PubMed, Web of Science (WoS), Scopus and Embase, using keywords such as ‘female circumcision’ or ‘female genital mutilation’ AND ‘infertility’. Articles were not restricted by publication time but were limited to English to avoid any bias. After the initial search, the duplicated articles were removed and the titles and abstracts of the remaining ones were assessed per the eligibility criteria. The authors NSS and MBG independently screened the articles based on their titles and abstracts, with full texts reviewed if necessary. If full texts were unavailable, the research team contacted the corresponding authors. The reference lists of retrieved articles were manually searched. To manage data, EndNote (Clarivate, Philadelphia, USA), the reference manager software, was used for searching, excluding duplications and reviewing titles and abstracts of selected articles based on the inclusion criteria.
2.2. Selection criteria
This review included human studies with a cohort and cross-sectional and case-control designs that investigated exposure to FGM and reported infertility outcomes. Interventional studies, case reports, letters to the editor, conference presentations and studies with insufficient data were excluded. Only articles that assessed FGM as the main independent variable and infertility as the dependent one were included in this systematic review and meta-analysis.
2.3. Data extraction
The authors NSS and FH independently identified the relevant articles, assessed their eligibility and extracted the data. Any disagreements were resolved through further discussion between the authors, with consultation from the third author (MD) and senior author (SEZ) if needed. The extracted data and the features of all studies included the author's last name, publication year, country of origin, statistical population, age, participants and sample size, type of study, FGM type and results [Table 1].
2.4. Quality assessment
Two authors (NSS and FH) independently assessed the quality of the selected articles and the certainty of their evidence, resolving conflicts through consensus. The results were verified by the third author (MD). Additionally, the Newcastle–Ottawa Scale (NOS) was utilised for the quality assessment of the analytical cross-sectional studies included in the current study, with a maximum of 7 points awarded based on the criteria of selection (2 points), comparability (2 points), and outcome/exposure (3 points).^2122^ Scores below 5 indicated low quality, while those of ≥5 indicated good quality studies [Table 2].
2.5. Statistical analysis
The data analysis was carried out using the full data extracted. The outcome variable (infertility) was treated as a dichotomous variable in all included articles. A forest plot was generated to assess the odds ratios (ORs) with a 95% confidence interval (CI) for visual inspection across the studies. The diamond in this plot represented the summary OR (or pooled OR) estimate, with its width indicating the corresponding 95% CI, using the random-effects meta-analysis. The square size and its central point further reflected the specific statistical weight (the inverse of variance) of the study and the point estimate of the OR, while the horizontal line represented its corresponding 95% CI. The I^2^ statistics and Cochran's Q test were employed to assess the statistical heterogeneity (P < 0.10) across the studies (I^2^ = 0% denoted no observed heterogeneity and I^2^ ≥50% represented substantial heterogeneity).^2324^ The visual inspection of the funnel plot as well as the Begg's and Egger's tests were not assessed for publication bias due to the limited number of studies included in the analysis. Additionally, sensitivity analysis was performed to determine which article (if any) had the greatest impact on the heterogeneity and assess the robustness of the pooled estimates. A significance level of P value <0.05 was for all analyses, except for the heterogeneity test. All statistical analyses were conducted using the Stata Software package, Version 17.0 (Stata Corp., College Station, Texas, USA).
3. Results
3.1. Search results and study characteristics
A total of 175 records were obtained through a database search. After excluding duplicates and irrelevant articles, 48 records remained, which were screened based on titles and abstracts, resulting in the exclusion of 36 records deemed irrelevant. Subsequently, 12 studies were evaluated in full text, with 7 studies being excluded for the following reasons: 2 studies lacked full text, 2 were case reports, 1 was descriptive and a further 2 had irrelevant outcomes. Ultimately, 5 studies (4 cross-sectional studies and 1 case-control study) involving 37,146 female participants were included in the present systematic review.^514161925^ Among these, only 3 studies met the inclusion criteria for the meta-analysis;^51419^ 2 cross-sectional studies were excluded due to insufficient data or incomplete and unadjusted analysis [Fig. 1].^1625^
Flow diagram of selection of published studies.
The 5 studies included in this systematic review involved 37,146 women with a mean age ranging from 15 to 55 years, conducted between 2000 and 2020 [Table 1].
3.2. Quality assessment findings
In the quality assessment, a modified version of the NOS for cross-sectional studies was used. One study (20%) was deemed to be of low quality (NOS <5),^16^ while the remaining 4 studies (80%) were classified as good quality (NOS ≥5).^5141925^ All studies achieved full scores in sections such as ‘ascertainment of the exposure’, ‘assessment of the outcome’, ‘comparability of the subjects in outcome groups on the basis of design or analysis’ and ‘appropriateness of the statistical tests’. The only area where studies fell short, gaining the lowest score, was in the ‘representativeness of the sample’ section [Table 2].
3.3. Association between female circumcision and infertility
The pooled overall OR using a random effects model was 1.21 (95% CI: 0.98–1.50). This meta-analysis indicated that FC, or FGM, was associated with a 21% increase in the odds of infertility compared to non-circumcised women, although this result was not statistically significant. There was no evidence of significant heterogeneity among the studies (P = 0.84 [Q statistics], I^2^ = 0.0%).
The study conducted by Almroth et al. exhibited heterogeneity compared to the other studies due to its case-control design.^14^ Even after excluding this study from the analysis, the non-significant association between FC and infertility remained [summary OR = 1.20, 95% CI: 0.97–1.48] with no observed heterogeneity (P = 0.98 [Q statistics], I^2^ = 0.0%) [Fig. 2].
Forest plot of the association between female circumcision and infertility.OR = odds ratio; CI = confidence interval.
A sensitivity analysis, where individual studies were sequentially removed to assess their influence on the pooled results, revealed a consistent increase in the odds of infertility (range of summary ORs: 1.20–1.27). This consistency suggests that the meta-analysis model was robust.
The assessment of publication bias was based on the assumption that smaller studies may be more susceptible to publication bias than larger ones. A visual inspection of the funnel plot suggested that publication bias was unlikely in the association between FC and infertility; however, this conclusion should be interpreted cautiously, as the analysis included a relatively small number of studies [Fig. 3].
Funnel plot for assessing the presence of publication bias in the studies on the association between female circumcision with infertility.
4. Discussion
Ultimately, 5 studies were included in this systematic review of which 3 were included in the meta-analysis. Out of these, 2 reported no significant association between FGM and infertility, though the ORs of infertility were higher in the circumcised group. In Ekudayo et al.'s study, a significant relationship between FGM and infertility was observed in the uncircumcised group. As a result, the direction of entry into the meta-analysis was reversed to compare FGM with non-FGM, as in the other 2 studies.
This meta-analysis revealed no significant relationship between FGM and infertility, but it did present a 21% increase in the odds of infertility among circumcised women compared to their uncircumcised counterparts. Thus, FGM may serve as a significant predictor of infertility. These findings are both statistically and clinically important, reinforcing efforts to combat this harmful practice.^14^ According to the WHO, reasons for FGM include the belief that it promotes health, enhances girls' development and readiness for marriage, controls women's premarital sexual desires, provides protection against illicit sexual activities, preserves purity and beauty and maintains cultural traditions passed down through generations.^26^ Since these reasons uphold cultural values, efforts to eradicate FGM have not been fully effective. However, the association with infertility challenges these traditional values, as motherhood is highly valued by all women and societies and infertility prevents women from attaining this identity.^1427^ Therefore, combating FGM should focus not only on its harmful health effects but also on women's reproductive rights as a whole.
In the context of the Islamic world, the stance of religious leaders on FGM remains unclear. While some religious leaders deny that FGM is a religious practice, others only prohibit FGM-III while allowing FGM-I and FGM-II. It is crucial to consider the potential role of religious leaders and authorities in efforts to eliminate FGM.^28^
As the WHO states, “healthcare professionals who perform FGM are violating girls' and women's rights to life, physical integrity, and health. They are also violating the fundamental ethical principle of “no harm””.^29^
The relationship between FGM and infertility is complex and controversial. FGM may provoke changes in the reproductive tract, such as altering bacterial colonisation in the vulva or vagina or causing low-grade chronic inflammation.^14^ Studies have reported an association between FGM and urinary and genital tract infections, with these recurrent infections often caused by incomplete bladder emptying and obstruction of the bladder outlet.^30313233^ Chronic inflammation may also lead to the formation of vesicovaginal and rectovaginal fistulas, which can contribute to infertility by creating a physical barrier to intercourse.^4^
Although more severe forms of excision and infibulation may affect infertility, only a small number of women in this systematic meta-analysis had undergone such procedures. Further research on infertility and fertility is necessary to enhance the understanding of the potentially debilitating effects of FGM, especially infibulation, on women's reproductive health.
A key aspect of this systematic review and meta-analysis was the assessment of bias in the included studies.^34^ Although several quality assessment tools exist, the NOS was used as the risk-of-bias assessment tool to evaluate the quality of the observational studies.^343536^ Completing the NOS was not time-consuming and covered important domains such as selection, comparability and outcomes (for cohort studies) or exposure (for case-control studies). The star system employed by the NOS provided a clear indication of the quality of the included studies.^3436^ To the best of the authors' knowledge, this is the first systematic review and meta-analysis to investigate the relationship between FGM and infertility. A notable strength of this study was the use of the NOS, which facilitated the inclusion of moderate- and high-quality studies, thereby bolstering the reliability of the results. However, there were certain limitations to this study, including the restriction to English-language studies and the limited number of published articles on this subject. Further research is required to delve deeper into the relationship between FGM and fertility or infertility.
5. Conclusion
This review found that FGM, in comparison to the absence of FC, was associated with a 21% increase in the OR of infertility. These findings are crucial in the preventive efforts against this ancient practice. It is recommended that further large-scale prospective studies be conducted to confirm these results. Additionally, healthcare professionals must be made aware of the clinical manifestations of FGM and the available management options. It is equally important for them to recognise their role in safeguarding girls from FGM and their responsibilities in reporting and documenting cases related to this harmful practice.
Authors' Contribution
Narges S. Soltani: Investigation, Formal analysis, Writing - Original Draft. Farahnaz Heshmat: Formal analysis. Mohsen Dehghani: Supervision, Formal analysis. Robab L. Roudsari: Writing - Review & Editing. Mohadese B. Ghalibaf: Investigation. Samira E. Zagami: Supervision, Writing - Review & Editing.
Ethics Statement
This project was approved by the Vice-Chancellor for Research, Mashhad University of Medical Sciences, Mashhad, Iran (ethical approval code: IR.MUMS.NURSE.REC.1402.096). The protocol was registered in PROSPERO (CRD42024507509).
Conflict of Interest
The authors declare no conflict of interest.
Funding
This study was funded by the Mashhad University of Medical Sciences (Grant number: 4021116).
Data Availability
Data is available upon reasonable request from the corresponding author.
Acknowledgements
We would like to thank the Research Vice-Chancellor of Mashhad University, Nursing and Midwifery Care Research Center for their cooperation in the execution of this project.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen G Dharia SP Steinkampf MP Callison S. Infertility from female circumcision. Fertil Steril 2004; 81:1692–4. https://doi.org/10.1016/j.fertnstert.2004.01.024.10.1016/j.fertnstert.2004.01.02415193498 · doi ↗ · pubmed ↗
- 2Okagbue HI Ijezie OA Samusenkov VO Erondu EC Eze GA. Female life expectancy, maternal mortality, fertility and birth rates of female genital mutilation high prevalence countries. Sci Afr 2020; 10:e 00647. https://doi.org/10.1016/j.sciaf.2020.e 00647.10.1016/j.sciaf.2020.e 00647 · doi ↗
- 3World Health Organization. Eliminating female genital mutilation. An interagency statement. From: https://www.who.int/publications/i/item/9789241596442 Accessed: Sep 2024.
- 4Aimen FM Monneins F Majed G Amine B. A rare cause of infertility: A late complication of female genital mutilation. Asian Pac J Reprod 2016; 5:266–8. https://doi.org/10.1016/j.apjr.2016.03.001.10.1016/j.apjr.2016.03.001 · doi ↗
- 5Morison L Scherf C Ekpo G Paine K West B Coleman R. The long-term reproductive health consequences of female genital cutting in rural Gambia: a community-based survey. Trop Med Int Health 2001; 6:643–53. https://doi.org/10.1046/j.1365-3156.2001.00749.x.10.1046/j.1365-3156.2001.00749.x 11555430 · doi ↗ · pubmed ↗
- 6Gerbaka B Richa S Tomb R. Female Genital Mutilation/Female Cutting/Female Circumcision. In: Child Sexual Abuse, Exploitation and Trafficking in the Arab Region. Cham, Switzerland:Springer, 2021. Pp. 155–82.
- 7Okonofua F. Female Circumcision/Mutilation/Cutting. In: Okonofua F Balogun JA Odunsi K Chilaka VN Eds. Contemporary Obstetrics and Gynecology for Developing Countries. Cham, Switzerland:Springer, 2021. Pp. 45–54.
- 8Young J Nour NM Macauley RC Narang SK Johnson-Agbakwu C. Diagnosis, management, and treatment of female genital mutilation or cutting in girls. Pediatrics 2020; 146:e 20201012. https://doi.org/10.1542/peds.2020-1012.10.1542/peds.2020-101232719089 · doi ↗ · pubmed ↗