A Case of Mirizzi Syndrome with Pancreatic Divisum: A rare association
Divya Muthuvel, Anita Soundarapandian

TL;DR
A rare case of Mirizzi syndrome combined with pancreatic divisum is reported, highlighting the importance of recognizing such associations for proper diagnosis and treatment.
Contribution
This paper presents a rare clinical association between Mirizzi syndrome and pancreatic divisum, contributing to the understanding of their potential interplay.
Findings
A 39-year-old female was diagnosed with Mirizzi syndrome type I and pancreatic divisum type II.
The association of pancreatic divisum may contribute to bile stasis and complications like calculous cholecystitis.
Early recognition of such rare associations can improve diagnostic accuracy and treatment outcomes.
Abstract
Mirizzi syndrome (MS), a rare complication of gallstones, refers to extrahepatic biliary compression by calculus in the cystic duct or Hartman's pouch and is usually associated with cystic duct abnormalities. Its association with pancreatic divisum (PD) is infrequent, the most common complication of PD being recurrent pancreatitis. We report a 39-year-old female patient who presented to a department of general surgery in Chennai, India, in 2022 with acute abdominal pain. Magnetic resonance cholangiopancreaticography (MRCP) showed calculous cholecystitis with a calculus indenting the cystic duct, causing luminal narrowing of the common hepatic duct (type I), which was associated with type II PD. The association of MS with PD has been rarely described. PD may be one of the factors responsible for bile stasis leading to calculous cholecystitis and its complications. Knowledge of MS and its…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
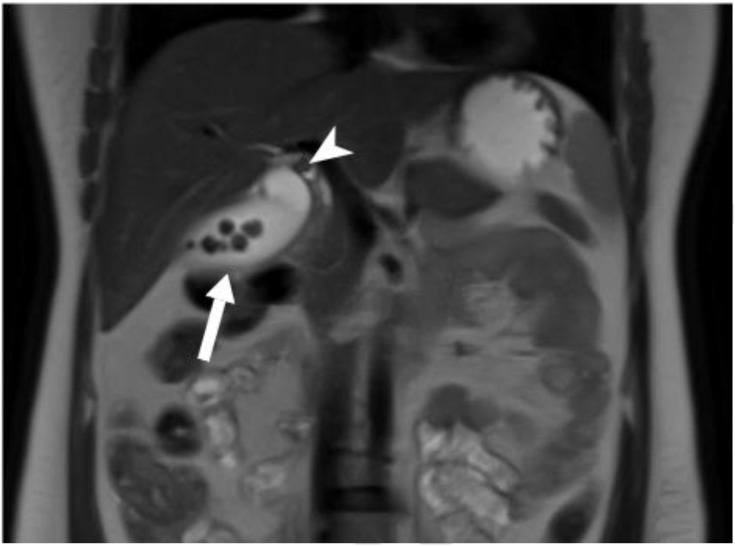 Fig. 1
Fig. 1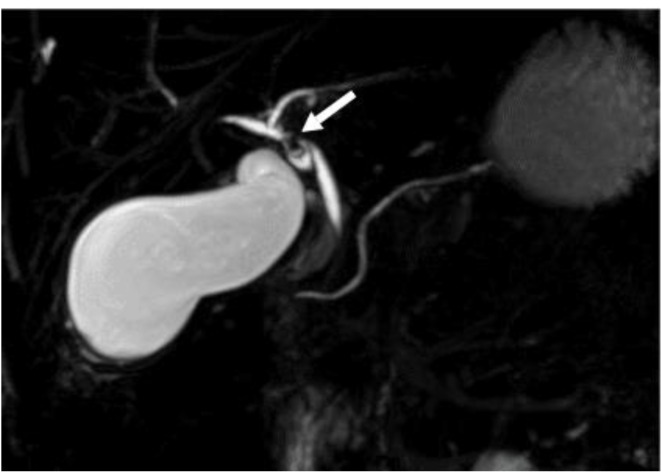 Fig. 2
Fig. 2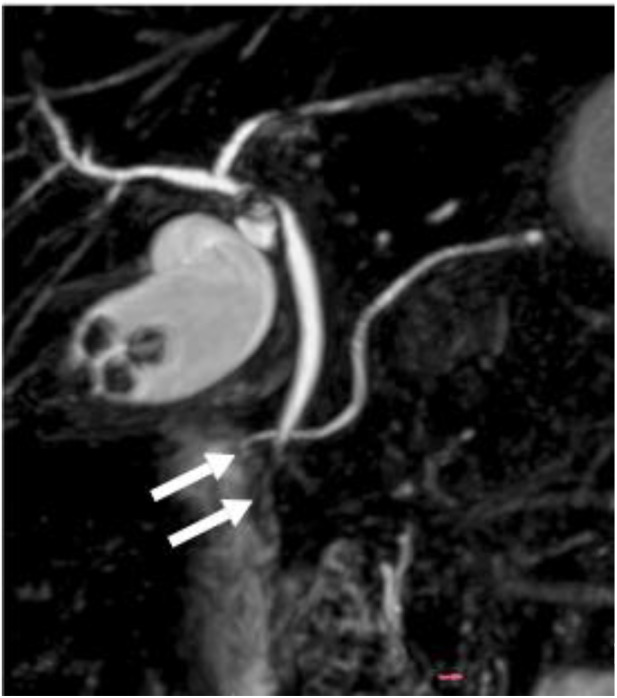 Fig. 3
Fig. 3| Type | Description |
|---|---|
| I | Extrinsic compression of CHD by impacted stone |
| a - in the cystic duct/Hartmann’s pouch. | |
| b - absence of cystic duct. | |
| II | Formation of cholecysto-choledochal fistula (<1/3rd wall circumference) |
| III | Formation of cholecysto-choledochal fistula (1/3rd - 2/3rd wall circumference) |
| IV | Formation of cholecysto-choledochal fistula (>2/3rd wall circumference) |
| V | Cholecystoenteric fistula with any other type of MS |
| a - without gallstone ileus. | |
| b - with gallstone ileus. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Hepatobiliary Diseases and Treatments · Gallbladder and Bile Duct Disorders · Biliary and Gastrointestinal Fistulas
1. Introduction
Mirizzi syndrome (MS) results from extrinsic compression of the extrahepatic biliary duct by the impacted gallstone in the Hartman's pouch or cystic duct. It is a rare complication of gallstones, with an incidence rate ranging from 0.6–5.7%.^1^ The compression can cause external obstruction, erosion, fibrosis or fistula, leading to complex complications.^2^ There is an association of cystic duct abnormalities in cases of MS; knowledge of various anatomical variations of the cystic duct is important in planning appropriate treatment strategies.^3^ The association of pancreatic divisum (PD) that occurs due to the failure of the fusion of dorsal and ventral pancreatic ducts with MS has rarely been described. However, thickened bile and cholelithiasis have shown an association with PD.^45^ This report presents a case of MS in a patient with PD.
2. Case report
A 39-year-old female patient presented to a general surgery outpatient department in Chennai, India, in 2022 with abdominal pain complaints lasting for 2 days. On examination, her vitals were stable; mild tenderness was noted in the right hypochondrium. Preliminary ultrasound evaluation showed multiple calculi in the gall bladder with mild wall thickening. The total leucocyte counts (TLC) were mildly raised ∼10,720/mm^3^ (normal TLC range: 4,500–10,500/mm^3^) but other laboratory investigations (liver function tests, serum amylase, lipase and renal function tests) were within normal limits. The patient underwent magnetic resonance cholangiopancreatography (MRCP) for further evaluation. MRCP imaging showed multiple calculi in the gall bladder lumen with features of acute calculus cholecystitis [Fig. 1]. One of the calculi was noted in the cystic duct indenting the common hepatic duct and causing luminal narrowing; however, no biliary dilatation was noted [Fig. 2].
Magnetic resonance cholangiopancreaticography T2 imaging in coronal view showing the gall bladder of a 39-year-old female patient showing multiple calculi (short arrow) within the lumen and 1 calculus in the cystic duct (arrowhead).
Magnetic resonance cholangiopancreaticography maximum intensity projection images showing calculus in cystic duct indenting the common hepatic duct (arrow).
The dorsal duct of the pancreas was seen draining into the minor papilla and the ventral duct was not well delineated. A common hepatic duct was seen draining into the major papilla [Fig. 3].
Magnetic resonance cholangiopancreaticography maximum intensity projection images showing the dorsal duct of the pancreas that drains into the minor papilla; the ventral duct is not well delineated. Common bile duct is draining into major papilla.
The diagnosis of type I MS with type II PD was made. The patient underwent cholecystectomy, and the post-procedure period was uneventful.
3. Discussion
Cholelithiasis is a relatively common disease entity with a female predilection. The formation of gallstones can be due to cholesterol supersaturation, excess bilirubin, gall bladder hypomotility, or impaired contractility.^6^ Most are asymptomatic; 1in 5 become symptomatic and presentation depends on the number, size and location of gallstones.^7^ Symptomatic cholelithiasis can lead to acute or chronic cholecystitis, empyema, obstructive jaundice, perforation of gall bladder, pericholecystic abscess, Mirizzi syndrome, gallstone ileus, etc., MS is a rare complication that needs high clinical suspicion because of non-specific symptoms and imaging plays an important role in its diagnosis. Csendes classification for MS is widely used to describe its severity [Table 1].^8^ MS has shown an association with anatomic abnormalities of the cystic duct, such as long cystic duct, tortuous course and low insertion of the cystic duct.^3^ Few cases have reported an association of pancreatic duct abnormalities with improper biliary drainage, thickened bile and cholelithiasis.^4^ PD is the most common congenital anomaly of the pancreas that results from the abnormal fusion of ventral and dorsal PD during fetal development with the incidence of 3.6–5.8%. Patients with PD were found to have gallstone disease more frequently than other conditions.^9^ Abnormal sphincter mechanism at ampulla can lead to bile stasis or could be due to dysfunction of bile excretion from the cystic duct; 85.7% of the patients with PD had demonstrated inflammation/cholesterolosis in the gall bladder.^10^ The current case is a rare association of MS type I with type II PD. Familiarity with the imaging appearance, anatomic variants, related associations and disease processes helps in accurate diagnosis and treatment planning, which prevents iatrogenic biliary injuries and complications.
4. Conclusion
MS is a rare complication of cholelithiasis and its association with PD is unusual. PD may be an additional factor, along with other associated risk factors for calculous cholecystitis and its complications. Management strategies mainly depend on patient symptoms and the presence of complications.
Ethics Statement
The patient provided informed consent for the publication of this case.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contribution
DM contributed to the clinical data collection, drafting of the manuscript and manuscript review. AS contributed to the collection of radiological data and manuscript editing. Bothauthors approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jesani S Romero AL Bozkurt SB Abu Samak AA Romero J Sookdeo J. Mirizzi syndrome: An unusual complication of cholelithiasis. J Community Hosp Intern Med Perspect 2022; 12:79–82. https://doi.org/10.55729/2000-9666.1114.10.55729/2000-9666.1114 PMC 992465136816165 · doi ↗ · pubmed ↗
- 2Klekowski J Piekarska AGóral M Kozula M Chabowski M. The current approach to the diagnosis and classification of Mirizzi syndrome. Diagnostics (Basel) 2021; 11:1660. https://doi.org/10.3390/diagnostics 11091660.10.3390/diagnostics 1109166034574001 PMC 8465817 · doi ↗ · pubmed ↗
- 3Shafiq S Patil M Philip M. Mirizzi syndrome: A retrospective analysis of 84 patients from a single center. Int J Gastrointest Interv 2022; 11:24–28. https://doi.org/10.18528/ijgii 210018.10.18528/ijgii 210018 · doi ↗
- 4Zhang R Li Z Hu X Liang H Yan G Xie D. Correlation between pancreatic duct variation and related diseases: An effective method observing the dual-energy CT with Low-ke V monoenergetic images. Diagnostics (Basel) 2023; 13:520. https://doi.org/10.3390/diagnostics 13030520.10.3390/diagnostics 1303052036766625 PMC 9914045 · doi ↗ · pubmed ↗
- 5Izzo P Di Cello P Pugliese F Izzo S Grande R Biancucci F. Pancreas divisum: Correlation between anatomical abnormalities and bile precipitation in the gall bladder in seven patients. G Chir 2016; 37:155–7. https://doi.org/10.11138/gchir/2016.37.4.155.10.11138/gchir/2016.37.4.15527938531 PMC 5161217 · doi ↗ · pubmed ↗
- 6Won MN Collins DP Bouchard S Finley C. Mirizzi syndrome type I: A case presentation. Cureus 2023; 15:e 37029. https://doi.org/10.7759/cureus.37029.10.7759/cureus.3702937143632 PMC 10153761 · doi ↗ · pubmed ↗
- 7Clemente G Tringali A De Rose AM Panettieri E Murazio M Nuzzo G. Mirizzi syndrome: Diagnosis and management of a challenging biliary disease. Can J Gastroenterol Hepatol 2018; 2018:6962090. https://doi.org/10.1155/2018/696209010.1155/2018/696209030159303 PMC 6109484 · doi ↗ · pubmed ↗
- 8Khokhar I Adourian M Delia E Mohan G Mathew M. Mirizzi syndrome: A case report and review of the literature. Cureus 2022; 14:e 24375. https://doi.org/10.7759/cureus.24375.10.7759/cureus.2437535619848 PMC 9126480 · doi ↗ · pubmed ↗