Anomalous Origin of the Posterior Descending Artery Causing Inferolateral Myocardial Ischaemia in an Octogenarian
Ahmad R. Bagheri, Madan M. Maddali, Adil A. Al-Jabri

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
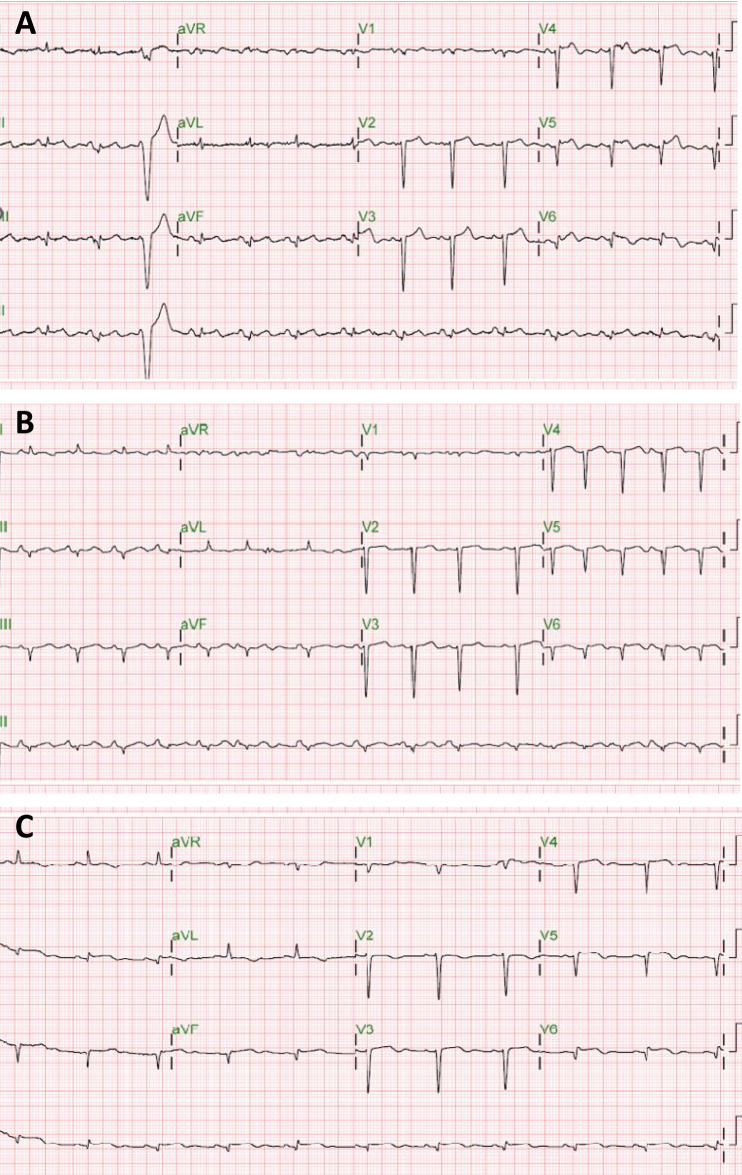 Figure 1
Figure 1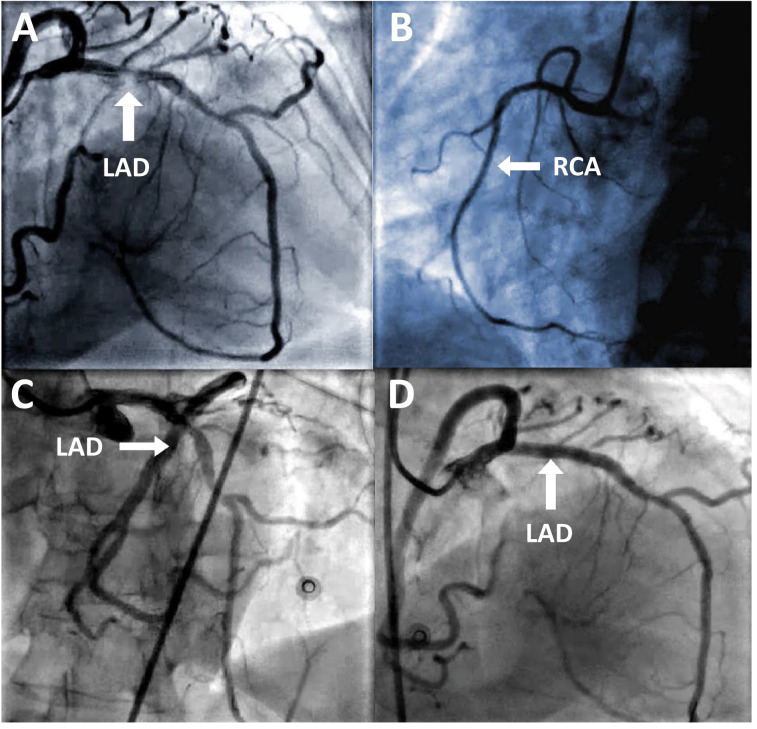 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Cardiovascular Issues in Pregnancy
Coronary artery anomalies can affect the origin, path and supply of the vessels either alone or in combination with other inherent defects, with a prevalence of less than 1.5%.^1^ Normally, the posterior descending artery (PDA) arises from the right coronary artery (in a right dominance or co-dominance pattern) or the left circumflex artery (in a left dominance pattern).^2^ Rarely, the posteroinferior septum is supplied by a hyperdominant left anterior descending artery (LAD), continuing as the PDA.^3^ The unique feature of this report is that an octogenarian sustained an inferolateral ST-segment elevation myocardial infarction (STEMI) that was not due to an occlusion of the left circumflex artery, but due to a lesion in a hyperdominant LAD continuing as the PDA. The patient underwent a successful percutaneous intervention.
An 81-year-old female patient presented to a tertiary care unit in Muscat, Oman, with a history of exertional angina, chest pain and dyspnoea of 1 week's duration in 2023. She was known to have diabetes and hypertension and was receiving medical treatment for these conditions. She mentioned that the chest pain was central and not radiating. However, at the time of indexed admission, she was dyspnoeic and hypertensive (systolic/diastolic blood pressure = 200/80 mmHg) but had no angina. The electrocardiogram showed ST segment elevation with q waves in the limb, augmented vector and chest leads (LII, III, aVF and V4-6) [Fig. 1A]. High-sensitivity cardiac troponin was 30 pg/mL. The patient presented late with a missed inferior lateral ST-elevation myocardial infarction. The transthoracic echocardiographic assessment revealed a normal left ventricle size with preserved systolic function (left ventricular ejection fraction: approximately 45–50%). There was evidence of Grade II diastolic dysfunction, indicated by an E/A ratio of 0.5 and an E/E' value of 15. An aneurysmal apex, characterised by an akinetic apical cap, was also observed. The right ventricle appeared normal in size with preserved systolic function, as demonstrated by a tricuspid annular plane systolic excursion of 20 mm and an S' velocity of 10 cm/s. Trace tricuspid regurgitation was noted, but no signs of pulmonary hypertension were present, with a right ventricular systolic pressure estimated at approximately 25 mmHg. An urgent coronary angiogram revealed that the right coronary artery was diminutive in size. The left main coronary artery appeared normal. The proximal segment of the LAD was normal. The LAD wrapped around the apex and continued as the PDA with no lesion [Fig. 2A–C and Supplementary Video 1–3]. In the LAD, there was a 70–80% stenosis after the first diagonal branch and a 30–40% stenosis just before the third diagonal branch. The third diagonal branch was large and normal. The left circumflex artery (LCX) was co-dominant and normal, with both the obtuse marginal branch and the left posterior lateral branch (LPLB) also appearing normal. The LPLB originated from the LCX, while the left posterior descending artery (LPDA) arose from the LAD, indicating a rare coronary anomaly. These findings suggested significant stenosis in the LAD and highlighted an unusual anatomical configuration. The left main coronary artery was accessed using a 6F JL4 guiding catheter. A 0.014-inch BMW wire was used to cross the vessel, followed by predilation with an NC TREK 3.0 × 15 mm balloon [Supplementary Video 4]. A drug-eluting stent with a biodegradable polymer measuring 4.00 mm in diameter and 18 mm in length was deployed, and post-dilation was performed with an NC TREK 4.5 × 12 mm balloon. A repeat coronary angiogram showed satisfactory results [Fig. 2D and Supplementary Video 5]. The patient was discharged on the third day after the procedure. The electrocardiograms were taken immediately after stent placement and at discharge; both showed improvement in the ST-segment changes [Fig. 1B and C].
1. Comment
In this report, we present an octogenarian who suffered a type-1 inferolateral STEMI caused by a plaque in the mid-LAD artery, which was hyper-dominant and continued as the PDA. There have been several reported unusual variations in the origin of PDA.^4^ It is uncommon for the PDA to originate from the LAD artery. However, it is common to observe a continuation of the LAD artery around the apex, typically referred to as the ‘wrap around’ LAD artery.^5^ Javangula and Kaul described the LAD continuing as the PDA up to the crux of the heart across the left ventricular apex for the first time.^6^ Musselman and Tate described a PDA originating from the LAD, extending beyond the crux, and branching into 2, with each branch traveling on either side of the posterior interventricular sulcus.^7^ In the current case, the LAD was hyperdominant in the true sense that it did travel for a considerable distance into the posterior interventricular sulcus beyond the crux as the PDA. The right coronary artery in the patient was non-dominant. To the best of the Authors' knowledge, this is an extremely rare case in which the hyperdominant LAD artery continued as PDA beyond the crux into the posterior interventricular sulcus.
The conservative management of a middle-aged man who presented with chest discomfort and in whom a coronary angiography showed a lesion-free LAD looping around the left ventricular apex and running through the posterior interventricular groove as a PDA beyond the crux, by adjustment of the patient's diabetic and hypertensive medications was reported recently.^8^ Similar to the current patient's management, a case of acute inferior wall myocardial ischaemia due to occlusion of LAD continuing as PDA, which was successfully managed by stent deployment, was also reported earlier.^9^
The clinical significance of this anomaly is profound, as occlusion of a hyperdominant LAD artery can jeopardise a significant portion of the myocardium. Clinicians must maintain a vigilant approach, particularly in cases presenting with combined ST elevation in both anterior and inferior leads, absence of reciprocal changes in inferior leads during anterior lead ST elevation, or concurrent anterior and inferior ischemia during stress testing. The shift in coronary dominance to the LAD from either the right coronary or left circumflex artery can dramatically alter the clinical presentation, necessitating careful assessment and timely intervention. Patient consent and institutional ethical committee approval were obtained for publication purposes.
Ethics Statement
A written informed consent from the patient and the ethical committee of the Ministry of Health, Muscat, Oman, provided approval (MOH/CSR/CR/ 24/10) to publish this report.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contribution
ARB conceptualised and designed the work. ARB and AAJ acquired the data. All authors analysed and interpreted the data, drafted and edited the manuscript. All authors approved the final version of the manuscript.
Supplementary material
Supplementary Video 1: Coronary angiogram showing the left anterior descending artery continuing as the posterior descending artery in the right anterior oblique cranial view.
Supplementary Video 2: Coronary angiogram showing the left anterior descending artery continuing as the posterior descending artery in the left anterior oblique cranial view.
Supplementary Video 3: Coronary angiogram showing the left anterior descending artery continuing as the posterior descending artery in the anteroposterior cranial view.
Supplementary Video 4: Coronary angiogram showing the balloon angioplasty of the left anterior descending artery.
Supplementary Video 5: Left coronary angiogram showing the successful outcome after deployment of the drug-eluting stent.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yamanaka O Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990; 21:28–40. https://doi.org/10.1002/ccd.1810210110.10.1002/ccd.18102101102208265 · doi ↗ · pubmed ↗
- 2Shaikh SSA Munde K Patil V Phutane M Singla R Khan Z. “Superdominant” left anterior descending artery continuing as posterior descending artery: Extremely rare coronary artery anomaly. Cardiol Res 2018; 9:253–7. https://doi.org/10.14740/cr 738w.10.14740/cr 738w 30116455 PMC 6089472 · doi ↗ · pubmed ↗
- 3Clark VL Brymer JF Lakier JB. Posterior descending artery origin from the left anterior descending: An unusual coronary artery variant. Cathet Cardiovasc Diagn 1985; 11:167–71. https://doi.org/10.1002/ccd.1810110208.10.1002/ccd.18101102083872720 · doi ↗ · pubmed ↗
- 4Kim JH Cha KS Park SY Park TH Kim MH Kim YD. Anomalous origins of the right and posterior descending coronary arteries from the left anterior descending coronary artery: Unusual pattern of single coronary artery. J Cardiol Cases 2011; 3:e 26–8. https://doi.org/10.1016/j.jccase.2010.07.003.10.1016/j.jccase.2010.07.00330532828 PMC 6265224 · doi ↗ · pubmed ↗
- 5Ilia R Weinstein JM Wolak A Gilutz H Cafri C. Length of left anterior descending coronary artery determines prognosis in acute anterior wall myocardial infarction. Catheter Cardiovasc Interv 2014; 84:316–20. https://doi.org/10.1002/ccd.24979.10.1002/ccd.2497923625458 · doi ↗ · pubmed ↗
- 6Javangula K Kaul P. Hyperdominant left anterior descending artery continuing across left ventricular apex as posterior descending artery coexistent with aortic stenosis. J Cardiothorac Surg 2007; 2:42. https://doi.org/10.1186/1749-8090-2-42.10.1186/1749-8090-2-4217949510 PMC 2104526 · doi ↗ · pubmed ↗
- 7Musselman DR Tate DA. Left coronary dominance due to direct continuation of the left anterior descending to form the posterior descending coronary artery. Chest 1992; 102:319–20. https://doi.org/10.1378/chest.102.1.319.10.1378/chest.102.1.3191623784 · doi ↗ · pubmed ↗
- 8Lalani K Rao MS Padmakumar R Parikh P. Rare coronary anomaly of posterior descending artery arising from superdominant left anterior descending artery. Methodist Debakey Cardiovasc J 2023; 19:88–91. https://doi.org/10.14797/mdcvj.1310.10.14797/mdcvj.131038161507 PMC 10756155 · doi ↗ · pubmed ↗