Prevalence of Viruses in Odontogenic Cysts and Tumours: A systematic review of literature and meta-analysis
Deepak Pandiar, Divya Gopinath, Pinky Pavithran, Reshma Poothakulath Krishnan, Jishnu Krishna Kumar, Sajesh K. Veettil

TL;DR
This study reviews and analyzes the presence of viruses in dental cysts and tumors, finding a low prevalence of viruses like HPV and Epstein-Barr virus.
Contribution
The study provides a systematic review and meta-analysis of virus prevalence in odontogenic cysts and tumors, highlighting their limited role in their development.
Findings
HPV prevalence in ameloblastomas was 18.21% (95% CI: 6.36–33.73).
HPV prevalence in odontogenic cysts was 1.51% (95% CI: 0.00–9.46).
Epstein-Barr virus prevalence in odontogenic tumors was 17.19% (95% CI: 4.62–34.49).
Abstract
This review aimed to assess the prevalence of oncogenic and non-oncogenic viruses in odontogenic cysts and tumours. A comprehensive database search was performed for published articles regarding the presence of viruses in all odontogenic cysts and tumours, following guidelines without date constraints, and was registered with PROSPERO. After screening 164 articles, 24 studies were included for systematic evaluation. A meta-analysis was performed to determine the prevalence of human papillomavirus (HPV), revealing an overall pooled prevalence of HPV in ameloblastomas of 18.21% (95% confidence interval [CI]: 6.36–33.73) while the prevalence of HPV in odontogenic cysts was found to be 1.51% (95% CI: 0.00–9.46). The prevalence of Epstein-Barr virus in odontogenic tumours was 17.19% (95% CI: 4.62–34.49). Other viruses yielded varied results. Human carcinogenesis has previously been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
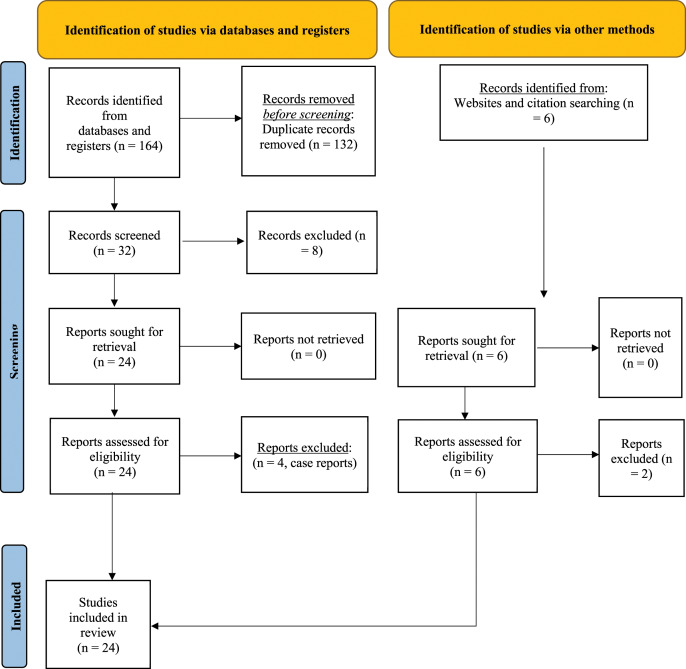 Fig. 1
Fig. 1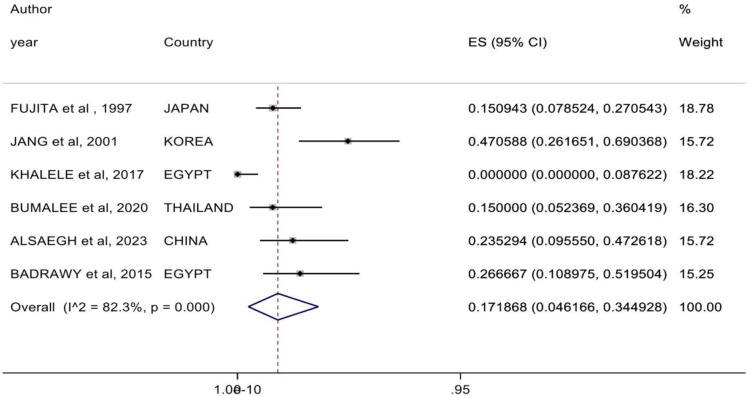 Fig. 2
Fig. 2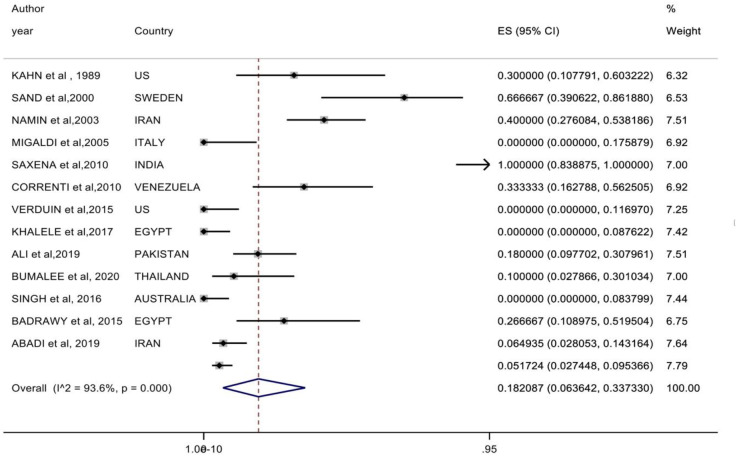 Fig. 3
Fig. 3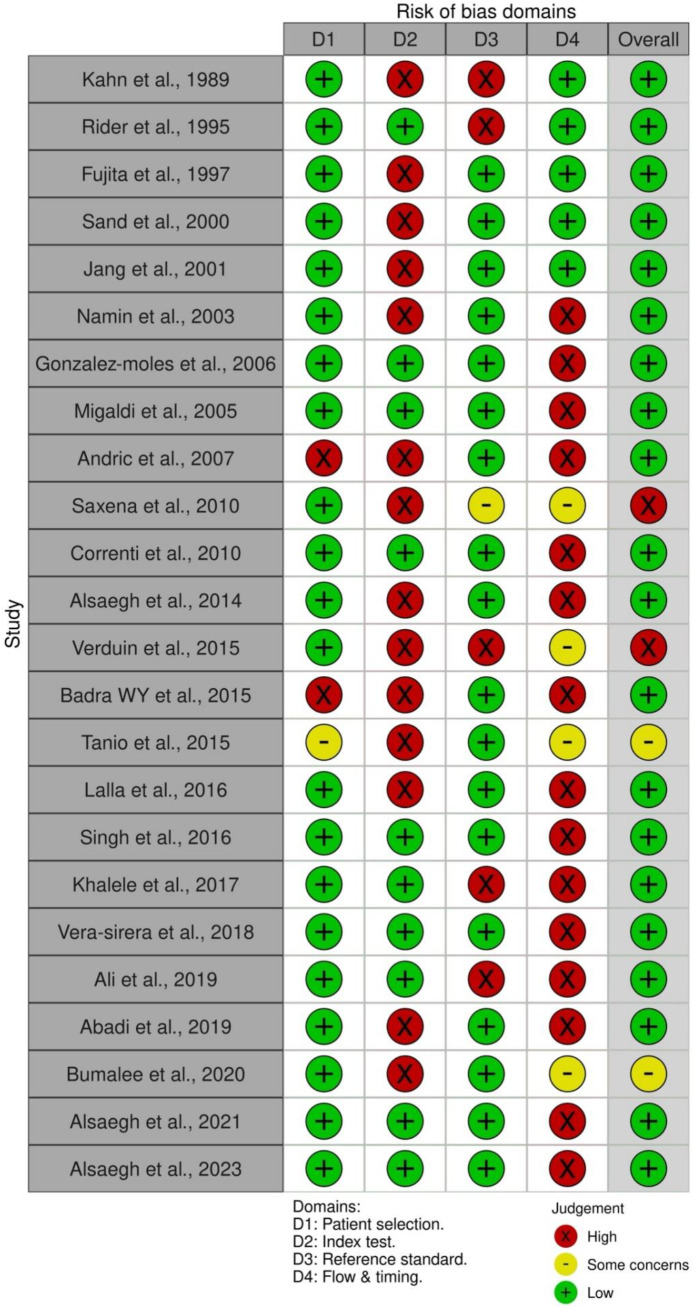 Fig. 4
Fig. 4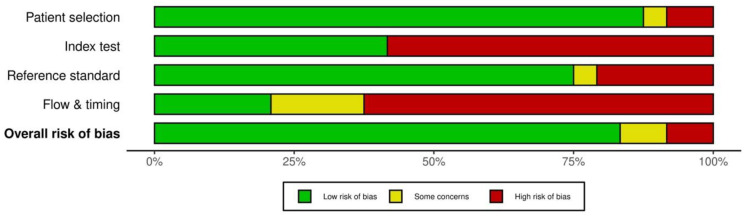 Fig. 5
Fig. 5| Author and year of publication | Type of study | Age in years | Sex | Country | No. of Cases | Number of controls | Lesion studied | Method of analysis | Virus type (if any) |
|---|---|---|---|---|---|---|---|---|---|
| Rider | Cross-sectional | NA | NA | NA | 20 | Radicular cyst | IHC | HPV, HSV1 and HSV2 negative | |
| Fujita | Cross-sectional | Average: 33 | 27 M 26 F | Japan | 53 ameloblastoma | 30 DC and 46 OKC | Ameloblastoma, DC and OKC | ISH | EBER 8/53 (15%) (FA > PA), DC and OKC negative |
| Sand | Cross-sectional | Average: 49.7 | 9 M 3 F | Sweden | 12 | Ameloblastoma | PCR | 8/12 positive for HPV (67%), 7/8 (HPV18) and 4/7 (HPV6/11) | |
| Jang | Case-control | 11–79 | 26 M 23 F | Korea | 32 non-odontogenic; 17 ameloblastoma | 12 normal tissue | Non-odontogenic (16 OSCC, 11 salivary gland neoplasms, 1 lymphoma, 1 MFH, 1 spindle cell Ca, 1 VC and 1 osteosarcoma) and 17 ameloblastoma | PCR | 17/32 (53%) non-od EBV DNA positive (bmlf1); 8/17 (48%) ameloblastoma EBV DNA positive (BamC); 11/12 (92%) normal |
| Kahn | Cross-sectional | Average: 10.4 | 18 M 20 F | USA (19 white and 14 black [available for 33]) | 38 (10) | 10 random adult ameloblastoma | Ameloblastoma of young | IHC | HPV positive in 3/10 in <19 years; 0/10 in adults |
| Namin | Case-control | Average: 31.8 | 26 M 23 F | Iran | 50 | 50 normal tissue | Ameloblastoma | PCR | 20/50 ameloblastoma positive (8 HPV6, 12 unidentified); 9/50 normal positive (unidentified strains) |
| Gonzalez-moles | Cross-sectional | Average: 26 | 47 M 36 F | NA | 83 | NA | OKC | PCR | 83/83 negative for HPV |
| Migaldi | Cross-sectional | Average: 41 | 8 M 10 F | Italy | 18 | NA | Ameloblastoma | IHC, ISH, laser capture microdissection and PCR | 18/18 negative for HPV |
| Andric | Cross-sectional | Average: 43.3 | 18 M 25 F | NA | 43 | NA | 33 periapical cysts and 10 OKC | PCR | 18/33 PC (54.50%) and 6/10 (60.0%) OKC positive for CMV |
| Saxena | Cross-sectional | Average: 27.5 | 1:0.43 | India | 20 | NA | Ameloblastoma | NM | 20/20 positive for HPV (95.0% HPV16) |
| Correnti | Cross-sectional | Average: 37.24 | 11 M 7 F | Venezuela | 18 | NA | 7 solid multicystic ameloblastoma and 11 unicystic ameloblastoma | IHC, CISH and nested PCR | All negative by IHC and CISH; 6/18 positive for HPV by nested PCR (66.0%) |
| Alsaegh | Cross-sectional | Average: 39 | 11 M 8 F | NA | 19 | NA | OKC | IHC, PCR | IHC (HPV-l1 13/19-68.40% positive) PCR (HPV DNA 7/19-36.80% positive) |
| Verduin | Cross-sectional | 52.34 | 21 M 8 F | USA | 29 | NA | 14 peripheral, l ameloblastoma and 15 intraosseous ameloblastoma | ISH | 29/29 negative for high-risk HPV; 1/29 focal and moderate positivity for low-risk HPV |
| Badrawy | Case-control | NA | 7 M 8 F | Egypt | 15 | 15 OSCC | Ameloblastoma | PCR | 2/15 (13.30%) OSCC positive for HPV and 4/15 (26.60%) ameloblastoma positive for HPV 3/15 (20.0%) OSCC positive for EBV and 4/15 (26.60%) ameloblastoma positive for EBV |
| Tanio | Cross-sectional | NA | NA | Japan | - | 14 radicular cysts, 10 dentigerous cysts, 10 OKC and 12 ameloblastoma | PCR | 1/14 RC, 1/12 ameloblastoma positive for Merkel cell; polyomavirus 10/10 DC and 10/10 OKC negative for Merkel cell polyomavirus | |
| Lalla | Cross-sectional | Average: 31.1 | 2.2:1 | NA | 29 | NA | OOC | PCR | 29/29 negative for HPV |
| Singh | Cross-sectional | NA | 1.703:1 | Australia | 42 | NA | Ameloblastoma | IHC (P16) and PCR | 42/42 negative for HPV by PCR |
| Khalele | Cross-sectional | NA | NA | Egypt | 80 | NA | 40 OKC and 40 ameloblastoma | IHC | 40/40 OKC and 40/40 ameloblastoma negative for HPV and EBV |
| Vera-sirera | Cross-sectional | Average: 36.06 | 10 M 6 F | Spain | 16 (2 excluded) | NA | OOC | PCR | 14/14 negative for high-risk and low-risk HPV |
| Ali | Cross-sectional | Average: 38.6 | 2.84: 1 | Pakistan | 50 | NA | Ameloblastoma | IHC | 9/50 (18.0%) positive for HPV; 41/50 (81.0%) negative for HPV |
| Abadi | Cross-sectional | Follicular 71.21; Acantho- matous 11.12; Basal cell 11.35 Desmo- plastic: 31.11; Cystic: 31.7; Plexiform: 25.17 | NA | Iran | 77 | NA | Ameloblastoma | Real-time PCR | 6.50% (5/77) ameloblastoma positive for HPV |
| Bumalee | Cross-sectional | Median: 48.5 | 12 M 8 F | Thailand | 20 | NA | Ameloblastoma | PCR | 2/20 (10.0%) positive for HPV; 3/20 (15%) for EBV |
| Alsaegh | Cross-sectional | Average: 40 (DC); Average: 39.42 (OKC); Average: 33.38 (amelo- blastoma) | DC (10 M and 3 F); OKC (5 M and 7 F); amelo- blastoma (8 M and 8 F) | Wuhan, China | 41 | NA | 13 DC, 12 OKC and 16 ameloblastoma | IHC and PCR | IHC: 12/16 (75.0%) in ameloblastoma; 2/13 (15.40%) in DC; 0/12 (0%) in OKC for CMV PCR: 10/16 (62.50%) in ameloblastoma; 4/13 (30.80%) in DC; 3/12 (25.0%) in OKC CMV |
| Alsaegh | Cross-sectional | Average: 39.53 (PC); Average: 39.69 (DC); Average: 37.39 (OKC); Average: 32.82 (amelo- blastoma) | PC (11 M and 4 F); DC (13 M and 3 F); OKC (11 M and 7 F); amelo- blastoma (9 M and 8 F) | Wuhan, China | 66 | NA | 15 PC, 16 DC, 18 OKC and 17 ameloblastoma | PCR | 4/17 (23.50%) in ameloblastoma; 6/15 (40.0%) in PC; 4/16 (25.0%) in DC; 10/18 (55.60%) in OKC for EBV 1/17 (5.90%) in ameloblastoma; 1/15 (6.70%) in PC; 6/16 (37.50%) in DC; 8/18 (44.40%) in OKC for KSHV |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral and Maxillofacial Pathology · Parvovirus B19 Infection Studies · Head and Neck Surgical Oncology
1. Introduction
Viruses are submicroscopic pathogens that contain either DNA or RNA as their genetic material. While most viruses cause self-limiting conditions, some can lead to lethal infectious diseases and malignant neoplasms with grave outcomes.^12^ Among head and neck malignancies, the role of viruses in oropharyngeal squamous cell carcinoma (human papillomavirus [HPV]) and nasopharyngeal carcinoma (Epstein-Barr virus [EBV]) has been widely studied and established.^234^ Recently, HPV-associated oral epithelial dysplasia has gained significant attention and has been included in the latest edition of the World Health Organization of head and neck tumours in 2024.^5^
Affecting a wide age range, odontogenic tumours (OTs) comprise a heterogeneous and enigmatic group of lesions, which can be intraosseous or peripheral. These tumours are derived from remnants of the odontogenic apparatus and may comprise odontogenic epithelium, ectomesenchyme and/or mesenchymal elements.^6^ Excluding odontomas, ameloblastoma is the most common odontogenic neoplasm. Although benign, it exhibits significant local destructive properties and has a propensity to metastasise to the lungs and lymph nodes. Conversely, the adenomatoid OT rarely grows to a grotesque size, emphasising the varied clinical behaviour and outcomes of tumours within the same class. This variability may be attributed to a complex interplay of various gene mutations and pathways.^78^
Uncountable mutations have been observed in odontogenic cysts and tumours, which contribute to their pathogenesis. Notable mutations include BRAF V600E, mitogen-activated protein kinase (MAPK)/Non-MAPK pathways and PTCH1 (via the SHH signalling pathway). Additionally, mutations in the EWSR1, CTNNB1 (Wnt molecular pathway), PTEN, CDKN2A, PTCH1, Janus kinase 3 (JAK3), MET and GDD1 genes, among others, have been identified.^910^ Furthermore, the role of viruses in the pathogenesis of OTs and cysts has been studied, yielding conflicting results worldwide. In an earlier study, ameloblastoma was induced in newborn mice using the polyomavirus.^11^ Gnathic tumours resembling ameloblastoma have also been experimentally induced in rats and mice in previous research. However, these earlier studies primarily utilised the polyomavirus to instigate the role of viruses in the pathogenesis of OTs.^121314^ Subsequently, most experimental data focused on other viruses, such as HPV and EBV, with limited studies on polyomavirus.^12131415161718^ This systematic review of the literature and meta-analysis aimed to assess the prevalence of oncogenic and non-oncogenic viruses in odontogenic cysts and tumours and to clarify whether these viruses, irrespective of order, family, subfamily, genus or species, play a role in the aetiopathogenesis of these enigmatic lesions based on prevalence estimates.
2. Methods
The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.^19^
This study posed the following 2 research questions: (1) what is the prevalence of specific viruses in odontogenic cysts and tumours; and (2) do viruses play a role in the etiopathogenesis of these conditions?
2.1. Strategy for identifying studies and keywords
A systematic literature review was performed using electronic databases, namely PubMed, Scopus, the Cochrane Library and Web of Science, without any date/period constraints. An extensive literature search was done under the umbrella term of ‘virus’ in ‘odontogenic cysts and tumors’ and singularly for individual viruses. The following keywords were used either singly or in combination: ‘virus odontogenic cyst’, ‘virus odontogenic tumor’, ‘human papilloma virus odontogenic tumor’, ‘HPV odontogenic tumor’, ‘human papilloma virus odontogenic cyst’, ‘HPV odontogenic cyst’, ‘polyoma virus odontogenic cyst’, ‘polyoma virus odontogenic tumor’, ‘arena virus odontogenic cyst’, ‘arena virus odontogenic tumor’, ‘herpes simplex/HSV virus odontogenic cyst’, ‘herpes simplex/HSV virus odontogenic tumor’, ‘Epstein Barr virus/EBV virus odontogenic cyst’, ‘Epstein Barr virus/EBV virus odontogenic tumor’, ‘cytomegalovirus/CMV virus odontogenic cyst’, ‘cytomegalovirus/CMV virus odontogenic tumor’, ‘Kaposi sarcoma-associated herpesvirus/KSHV odontogenic tumor’ and ‘Kaposi sarcoma-associated herpesvirus/KSHV odontogenic cyst’.
2.2. Inclusion and exclusion criteria
All original research papers that assessed the prevalence of any virus in odontogenic cysts and tumours were included in the current review; however, editorials, letters, commentaries, case reports and case series were excluded. All original studies were included irrespective of the language, with Google Translate employed to extract data from non-English papers. Subsequently, the titles and abstracts were screened for final data extraction. Any duplicates were removed and eligible papers were manually retrieved by checking the cross-references. Studies that utilised p16 immunohistochemistry (IHC) to detect HPV were also excluded. p16 serves as a surrogate marker for detecting HPV in cervical and oropharyngeal squamous cell carcinoma. Its role in detecting HPV in other anatomical sites is questionable, and more specific and sensitive tests, such as polymerase chain reaction (PCR) and in situ hybridisation (ISH), are preferred for identifying HPV in sites other than the oropharynx. Consequently, studies that relied on p16 for HPV detection were not included.^20^ Only studies that detected HPV through molecular techniques (PCR/ISH) or HPV-specific antibodies for IHC were included in the review.
2.3. Selection of studies
All articles were independently screened by two authors (DP and DG) to extract the following information: country of origin, author(s) and year of publication, type of study, mean age, gender, number and subtype of cases (controls, if any), method of virus detection and specific viruses identified in all odontogenic cysts and tumours. Any discordance was resolved through discussion with a third author (RPK). The data were presented in a Microsoft Excel spreadsheet, Version 2021 (Microsoft, Redmond, Washington, USA). For the final evaluation and meta-analysis, Statistical Package for the Social Sciences (SPSS), Version 26.0 (IBM Corp., Armonk, New York, USA) and Stata, Version 15.0 (StataCorp, College Station, Texas, USA) were used. The 95% confidence interval (CI) accompanying the results was used to measure the outcomes. To determine whether a fixed (I^2^ <50%) or random (I^2^ ≥50%) effects model should be used, statistical heterogeneity was calculated using the I^2^ test. If the ascertainment method revealed heterogeneity, subgroup analysis was carried out. In cases where the number of studies within subgroups was insufficient, subgroup analysis was not performed. A P value of ≤0.05 was considered statistically significant.
2.4. Quality assessment
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool was used to assess the risk of bias for each study. The checklist items for the QUADAS-2 tool include patient selection, index test, reference standard and flow and timing; 2 authors (DP and PP) independently assessed the risk of bias for each domain of the tool, categorising it as high/moderate/low risk. Statistical analyses were performed using Review Manager (RevMan v5.3, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark).
3. Results
A total of 164 articles were retrieved from various databases, of which 132 were duplicates and were therefore excluded. From the remaining 32 articles, 12 were further excluded for not meeting the inclusion criteria of which 4 were case reports. Additionally, 6 relevant papers were retrieved through cross-referencing, resulting in 4 more articles for inclusion. Finally, 24 articles were included in the systematic review and meta-analysis [Fig. 1].
Flowchart of study selection adapted from preferred reporting items for systematic reviews and meta-analyses.
3.1. Study characteristics
A total of 24 studies were included in the present systematic review.^1516171821–40^ Of these, 6 studies were used for meta-analysis to detect HPV in OTs,^161829303640^ while 13 studies were employed to detect EBV in OTs.^17212224262729303334363738^ The studies were published in English and Arabic between 1989 and 2023. In terms of country of origin, 2 studies originated from Japan,^330^ the USA,^2129^ Egypt,^3034^ Iran,^2237^ and China.^3940^ Countries that reported 1 study each were Sweden,^19^ India,^26^ Spain,^35^ Pakistan,^36^ Thailand,^38^ Italy,^24^ Venezuela,^27^ Korea^18^ and Australia.^33^ No details were available for the remaining 5 articles.^1523252832^ PCR was the most commonly employed detection method, followed by IHC and ISH [Table 1].
3.2. Detection of HPV in odontogenic cysts and tumours
A total of 13 studies evaluated the presence or absence of HPV in OTs,^17212224262729303334363738^ while 6 studies investigated HPV in odontogenic cysts.^152328323435^ Surprisingly, HPV was exclusively studied in ameloblastoma. The findings varied across studies; the earliest research conducted by Kahn reported positivity in 3/10 cases of ameloblastoma in individuals younger than 19 years of age.^21^ Other studies detected HPV through PCR in ameloblastoma, albeit in only a few cases. However, most studies reported negative expression.^1722262730363738^ Additionally, no virus was detected in 4 studies.^24293334^
Regarding odontogenic cysts, HPV has been studied in different varieties of inflammatory and developmental cysts, including radicular cysts (RCs), odontogenic keratocysts (OKCs) and orthokeratinised odontogenic cysts (OOCs).^152328333435^ All but 1 study demonstrated no presence of HPV in any of the cysts, resulting in an overall prevalence of 1.5%. However, most studies recorded 0 events, leading to a very low CI. Alsaegh et al. demonstrated HPV L1 in 13/19 (68.4%) cases using IHC; however, only 7/19 cases tested positive for HPV DNA (36.8%) via PCR.^28^ The other 2 articles that examined HPV in OKC found negative expression in all cases (0/123, total of both).^2233^ Similarly, the virus was not detected in RC and OOC.^153235^
A meta-analysis was performed to assess the prevalence of HPV in OTs, specifically focusing on ameloblastoma. Using random-effects estimation, the overall pooled prevalence of HPV in ameloblastomas, including peripheral variants, based on 13 studies (174 cases), was found to be 18.21% (95% CI: 6.36–33.73) [Fig. 2]. This analysis revealed substantial interstudy heterogeneity (I^2^ = 93.6%; P <0.001). Additionally, the meta-analysis regarding the prevalence of HPV in odontogenic cysts yielded an overall percentage of 1.51% (95% CI: 0.00–9.46%, I^2^ = 79.5%; P <0.001).
Forest plot showing meta-analysis results for the prevalence of human papillomavirus in odontogenic tumours.
3.3. Detection of EBV in odontogenic cysts and tumours
In 6 articles, the EBV was evaluated in OTs.^161830343840^ Among these studies, Fujita et al., Khalele and Alsaegh et al. also included RCs, OKCs and dentigerous cysts (DC).^163440^ Concerning OTs, ameloblastoma was the only neoplasm studied in all the included research. Overall, 162 cases of ameloblastoma were evaluated across the 6 studies, with 27 cases showing detectable EBV. Khalele's study from Egypt reported negative results (0/40); interestingly, none of the 40 cases of OKC from the same region and study group tested positive for EBV.^34^ Regarding odontogenic cysts, there were 15 cases of RC, 104 cases of OKCs and 46 cases of DC (N = 165). Out of these, only 20 cases (6/15 RC, 4/16 DC and 10/18 OKC; overall 20/165 or 12.12%) were positive for the presence of EBV and all these positive cases were from Korea. Cases from Japan and Egypt were negative for EBV in DCs and OKCs.^1833^ A meta-analysis using a random effects model (I^2^ = 82.3%; P <0.001) of the 6 included studies (n = 162) yielded a prevalence of 17.19% for EBV in OTs (95% CI: 4.62–34.49%) [Fig. 3].
Forest plot showing meta-analysis results for the prevalence of Epstein-Barr virus in odontogenic tumours.
3.4. Detection of cytomegalovirus in odontogenic cysts and tumours
In two studies, cytomegalovirus (CMV) was analysed in odontogenic cysts, with 1 study also examining CMV in ameloblastoma. Andric et al. found that 18/33 RC (54.54%) and 6/10 (60%) OKC cases exhibited the presence of CMV.^25^ Alsaegh et al. reported CMV in 4/13 DC (30.77%), 2/12 OKC (16.67%) and 10/16 ameloblastoma (62.5%).^39^ Overall, the prevalence of CMV was 43.7% (3.19–55.9%) in odontogenic cysts and 62.5% in ameloblastoma.
3.5. Detection of other viruses
Other less commonly studied viruses belong to the human herpesvirus family and include Merkel cell polyomavirus, which was detected employing PCR and IHC. Two specific viruses, herpes simplex virus (HSV) and Kaposi sarcoma-associated herpesvirus (KSHV), were analysed. Regarding KSHV, Alsaegh et al. estimated an overall prevalence of 30.61% in odontogenic cysts (including RC, DC and OKC) and 5.88% in ameloblastoma (1/17, 5.88%).^40^ Individually, KSHV was identified in 1/15 RC (6.67%), 6/16 DC (37.5%) and 8/18 OKC (44.44%). The presence of HSV Types 1 and 2 was examined in 20 cases of RC in one of the earlier studies, and no viruses were detected (0/20).
Tanio et al. evaluated the presence of Merkel cell polyomavirus in odontogenic cysts (RC, DC and OKC) and ameloblastomas. The study found that 1/14 RC and 1/12 ameloblastomas tested positive for Merkel cell polyomavirus. In contrast, 10/10 DC and 10/10 OKC were negative for the virus.^31^
3.6. Quality assessment: Risk of bias and applicability concerns
According to the QUADAS-2 tool, an overall low risk of bias was noted in 20/24 studies; 2 studies were classified as high risk,^2629^ while the remaining 2 raised some concerns in 1 or 2 of the domains studied [Fig. 4, Fig. 5].^3138^
Summary of bias risks and applicability concerns for each study, based on the quality assessment of diagnostic accuracy studies tool 2.
Risk of bias and applicability concerns based on the quality assessment of diagnostic accuracy studies tool 2.
4. Discussion
Viruses are enigmatic submicroscopic pathogenic structures that play established roles in various human malignancies, such as oropharyngeal squamous cell carcinoma, HPV-related oral epithelial dysplasia, nasopharyngeal carcinoma, Burkitt lymphoma, cervical squamous cell carcinoma and variants of leukaemia.^34^ Many earlier studies have attempted to induce ameloblastoma-like tumours in rodents, demonstrating the role of polyomavirus in the pathogenesis of OTs.^11121314^ However, there remains ambiguity regarding the plausible role of these pathogens in odontogenic cysts and tumours. Subsequently, further studies have been conducted on a plethora of viruses from different genera and families in variegated odontogenic pathologies. Thus, this systematic review of the literature aimed to consolidate information regarding the plausible role of viruses in the etiopathogenesis of odontogenic lesions.
It was noted that amongst all OTs, ameloblastoma was the only neoplasm exclusively studied. Regarding odontogenic cysts, RCs (periapical), DCs, OKCs and OOCs were the most frequently investigated. Overall, HPV was the most commonly studied virus. The presence of HPV in odontogenic cysts and tumours varied; 4 research articles reported no HPV detection in any of the investigated cases of ameloblastoma, while another group of investigators detected the virus in a few cases.^24293334^ Overall, the pooled prevalence of HPV-DNA in ameloblastoma was found to be only 18.21% (95% CI: 6.36–33.73). This review found that molecular detection methods yielded a significantly lower prevalence of HPV in odontogenic cysts compared to immunohistochemical detection. However, for odontogenic lesions, IHC may not yet be considered the ideal method for HPV detection.
In some studies, p16 has been used for detection; however, it is not a reliable surrogate marker for HPV detection in odontogenic lesions. Furthermore, p16 staining varies widely based on the type of clone used. HPV is a known oncogenic DNA virus with an established role in oropharyngeal and cervical squamous cell carcinomas, which also display contrasting demographic variegations. Previous studies have shown that HPV-DNA can be detected in the placenta, amniotic fluid and umbilical cord. Additionally, the placenta and chorionic tissue may become infected through the haematogenous route; thus, transplacental transmission may happen when the infection spreads to amniotic cells and finally to the fetus.^4142^ At the time of development, the virus is likely to infect the dental apparatus; however, as the meta-analysis indicated that the prevalence of HPV in ameloblastoma is too low, the likelihood of HPV acting as the sole oncogenic factor seems improbable. Furthermore, there are many confounding factors that need consideration. First, the testing methods employed vary across different studies. Second, maternal HPV status, particularly regarding vaccination, is not available in all reports. A low prevalence of HPV could also be attributed to its dependence on differentiating epithelial cells for replication, such as oral epithelial cells,^4344^ and the lack of well-differentiated epithelia in most OTs. The presence of HPV in keratinising cysts or cysts with verrucous histomorphology supports this hypothesis.
The role of EBV has been well-established, mainly in B-/T-cell lymphomas and/or lymphoproliferative disorders and malignancies of epithelial origin, such as nasopharyngeal and gastric carcinomas.^445^ Activation of various signalling pathways has been postulated in EBV-induced oncogenesis within host cells, regulated by both coded proteins and non-coded RNA. These pathways include MAPK, phosphoinositide-3-kinase/protein kinase B (PI3K/AKT), nuclear factor-κB (NF-κB), JAK/signal transducer and transcription activator (STAT), transforming growth factor-β (TGF-β) and Wnt/β-catenin pathways. Interestingly, many of these pathways also regulate odontogenesis, suggesting a plausible role for EBV in odontogenic pathologies.^464748^ However, the prevalence of EBV in ameloblastoma was even lower (17.19%, 95% CI: 4.61–34.50%). In one study, the BamC gene was the most frequently detected among the EBV-DNA regions in OTs, in contrast to the BMLF1 gene, which was more prevalent in non-OTs.^18^ The authors further observed that the BamC gene was frequently found in benign lesions, while malignancies demonstrated the BMLF1 gene. This distinction led the authors to opine that BamC is an epitheliotropic gene, while BMLF1 is lymphotropic, as evidenced by its association with inflammation in non-OTs.^18^
It was noted that amongst the cysts, EBV was detected in 12.12% (20/165) of cases, with all positive cases originating from Wuhan, China, as confirmed by PCR. Conversely, the Japanese (ISH) and Egyptian samples (IHC) showed complete negativity.^1634^ The observed discordance may be attributed to demographic variations or differences in methodology across 3 studies.^163440^ Comparatively, CMV was identified at a higher percentage; however, data regarding the prevalence of CMV were limited, with only two studies available.^2438^ Although research on the detection of CMV in cysts and tumours is scarce, few authors have suggested that PCR is more sensitive for detecting CMV in cysts, while IHC appears to be more sensitive for ameloblastoma. Nonetheless, a confirmatory role remains unelucidated. Other viruses showed similar variegated results.
The present systematic review is subject to certain limitations. Heterogeneity was observed among the included studies, which may be attributed to variations in study design, differing protocols and discrepancies in detection techniques. Furthermore, the sample size for sub-group analysis was limited, and there is a scarcity of studies analysing viruses in tumours other than ameloblastoma.
5. Conclusion
Although the role of viruses in human carcinogenesis is well established, with a definitive temporal effect and causal relationship, the present systematic review's results demonstrate a limited role in OTs and cysts.
Authors' Contributions
Deepak Pandiar: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing- original draft. Divya Gopinath: Data curation, Formal analysis, Methodology, Validation, Writing – review & editing. Pinky Pavithran: Formal analysis, Methodology, Validation, Writing – review & editing. Reshma P. Krishnan: Supervision, Methodology, Validation, Writing – review & editing. Jishnu K. Kumar: Supervision, Validation, Writing – review & editing. Sajesh K. Veettil: Formal analysis, Writing – review & editing.
Ethics Statement
The review was first registered in the International Prospective Register of Systematic Reviews database (PROSPERO #: CRD42023424259).
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ryu WS. Discovery and classification. Molecular Virology of Human Pathogenic Viruses 2017; 3–20. https://doi.org/10.1016/B 978-0-12-800838-6.00001-1.10.1016/B 978-0-12-800838-6.00001-1 · doi ↗
- 2Pandiar D Nayanar SK Babu S Babu S. Expression of p 16INK 4a in oropharyngeal squamous cell carcinoma from a tertiary cancer centre of South India: A preliminary study. Indian J Med Res 2021; 154:497–503. https://doi.org/10.4103/ijmr.IJMR_386_19.10.4103/ijmr.IJMR_386_1935345076 PMC 9131790 · doi ↗ · pubmed ↗
- 3Sri S Ramani P Premkumar P Ramshankar V Ramasubramanian A Krishnan RP. Prevalence of human papillomavirus (HPV) 16 and 18 in oral malignant and potentially malignant disorders: A polymerase chain reaction analysis – A comparative study. Ann Maxillofac Surg 2021; 11:6–11. https://doi.org/10.4103/ams.ams_376_20.10.4103/ams.ams_376_2034522646 PMC 8407623 · doi ↗ · pubmed ↗
- 4Zhang J Luo X Huang Q Huang Y. Clinicopathological and prognostic features of nasopharyngeal carcinoma in children and adolescents: A retrospective study of 196 cases in South China. Int J Cancer 2021; 148:1087–96. https://doi.org/10.1002/ijc.33293.10.1002/ijc.3329332930415 · doi ↗ · pubmed ↗
- 5World Health Organization. WHO Classification of Tumours Editorial Board. Head and Neck Tumours, 5th ed. Lyon, France:International Agency for Research on Cancer, 2024.
- 6Pandiar D Shameena PM Sudha S Varma S Manjusha P Banyal VS. Odontogenic tumors: A 13-year retrospective study of 395 cases in a South Indian Teaching Institute of Kerala. Oral Maxillofac Pathol J 2015; 6.
- 7Boffano P Cavarra F Brucoli M Ruslin M Forouzanfar T Ridwan-Pramana A. The epidemiology and management of odontomas: A European multicenter study. Oral Maxillofac Surg 2023; 27:479–87. https://doi.org/10.1007/s 10006-022-01091-w.10.1007/s 10006-022-01091-w 35715707 · doi ↗ · pubmed ↗
- 8Pandiar D Anand R Kamboj M Narwal A Shameena PM Devi A. Metastasizing ameloblastoma: A 10 year clinicopathological review with an insight into pathogenesis. Head Neck Pathol 2021; 15:967–74. https://doi.org/10.1007/s 12105-020-01258-5.10.1007/s 12105-020-01258-533394372 PMC 8384989 · doi ↗ · pubmed ↗