Efficacy of Hormonal and Non-Hormonal Vaginal Gel Preparations on the Female Sexual Satisfaction Index in Postmenopausal Women with Sexual Dysfunction Syndrome: A PRISMA-compliant meta-analysis
Ahmed Soliman, Hanaa Alrashidi, Mohamed A. Mohamed, Reem Ghorab, Nihal Al Riyami, Ahmed S. A. Ashour, Yasmine A. Mohammed, Ahmed H. Saad

TL;DR
This study found that non-hormonal vaginal gels, like chamomile and fennel, improved sexual satisfaction more than hormonal gels in postmenopausal women.
Contribution
The study is the first to compare non-hormonal and hormonal vaginal gels in postmenopausal women using a meta-analysis of sexual satisfaction scores.
Findings
Non-hormonal gels showed a significantly higher total FSFI score than hormonal gels.
Vaginal gels improved all domains of the Female Sexual Function Index compared to placebo.
Chamomile and fennel gels positively impacted sexual satisfaction in postmenopausal women.
Abstract
This meta-analysis aimed to compare the efficacy of vaginal gel preparations versus placebo in postmenopausal women with sexual dysfunction syndrome. Searches of electronic databases from inception to January 2023 identified 8 trials (N = 672) that reported the Female Sexual Function Index (FSFI) and compared hormonal (oestrogen, oxytocin) and/or non-hormonal (chamomile, fennel) interventions against placebo. The Cochrane Risk of Bias tool was used to assess studies’ quality. The vaginal gel group had a significantly higher total FSFI endpoint score (mean difference [MD] = 6.67, 95% confidence interval [CI]: 3.79–9.55; P < 0.001) than placebo. Non-hormonal gels exhibited a greater FSFI total score (MD = 6.73, 95% CI: 4.7–8.76; P < 0.001) than hormonal gels (MD = 2.75, 95% CI: 1.87–3.64; P < 0.001), positively impacting all FSFI domains. These findings indicate that chamomile and fennel…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
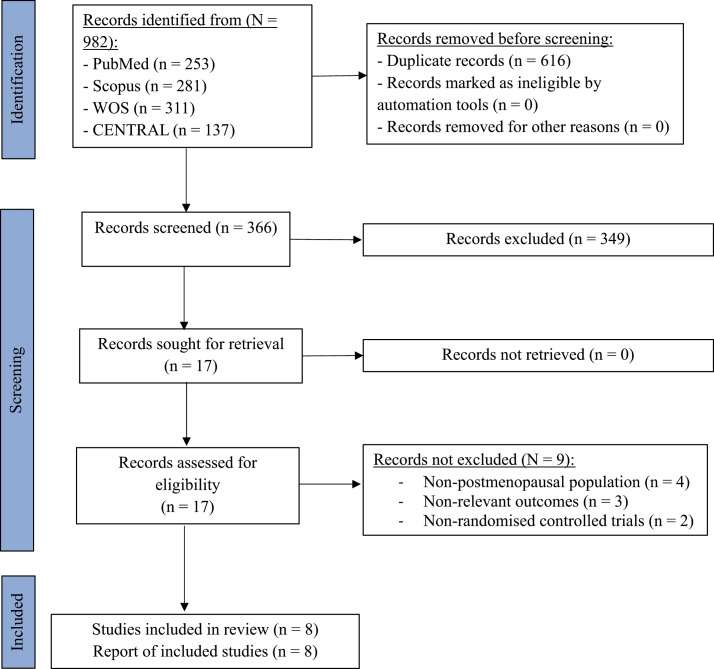 Fig. 1
Fig. 1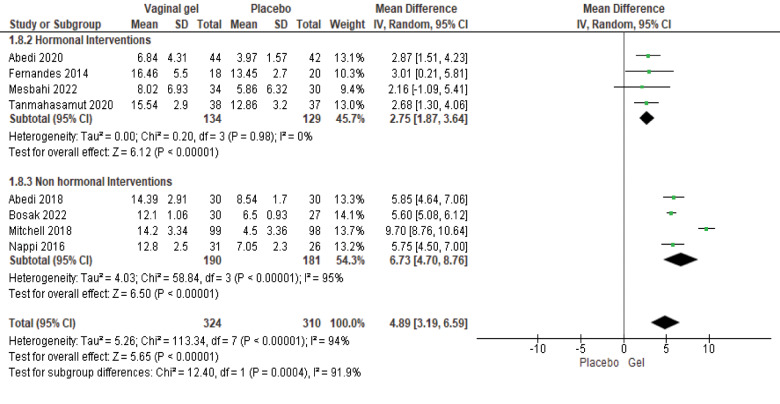 Fig. 2
Fig. 2| Study arms | |||||
|---|---|---|---|---|---|
|
| |||||
| Author and year of publication | Country | Trial duration in weeks | Total sample size | Intervention | Control |
| Abedi | Iran | 8 | 60 | Fennel gel | Placebo gel |
| Abedi | Iran | 8 | 6 | Oxytocin gel | Placebo gel |
| Bosak | Iran | 12 | 57 | Chamomile gel | Placebo gel |
| Fernandes | Brazil | 12 | 38 | Oestrogen gel | Oil lubricant |
| Mesbahi | Iran | 8 | 64 | Oxytocin gel | Placebo gel |
| Mitchell | USA | 12 | 197 | Moisturiser gel + placebo | Dual placebo |
| Nappi | Italy | 8 | 95 | Monurelle Biogel gel | Placebo gel |
| Tanmahasamut | Thailand | 8 | 75 | Oestradiol gel | Placebo gel |
| Author and year of publication | Group | Number of participants | Mean age ± SD in years | Mean age of menopause ± SD in years | Economic status, n | Mean coitus frequency ± SD per week | ||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Weak | Good | High | ||||||
| Abedi | Fennel gel | 30 | 53.7 ± 3.6 | 49.5 ± 2.0 | 9 | 14 | 7 | 2.07 ± 1.3 |
| Placebo gel | 30 | 52.9 ± 3.4 | 49.3 ± 1.9 | 11 | 12 | 7 | 1.77 ± 0.47 | |
| Abedi | Oxytocin gel | 44 | 54.2 ± 3.3 | 50.0 ± 2.2 | 17 | 21 | 6 | 2.75 ± 1.34 |
| Placebo gel | 42 | 54.1 ± 3.7 | 50.4 ± 2.6 | 16 | 19 | 7 | 2.38 ± 0.88 | |
| Bosak | Chamomile gel | 30 | 53.5 ± 5.7 | 49.0 ± 2.3 | 5 | 21 | 4 | 1.5 ± 0.94 |
| Placebo gel | 27 | 54.3 ± 5.5 | 50.0 ± 1.8 | 5 | 20 | 2 | 1.69 ± 1.32 | |
| Fernandes | Oestrogen gel | 18 | 56.4 ± 4.8 | 51.1 ± 1.5 | NR | NR | NR | NR |
| Oil lubricant | 20 | 57.7 ± 4.7 | 50.3 ± 1.1 | NR | NR | NR | NR | |
| Mesbahi | Oxytocin gel | 34 | 31.2 ± 5.1 | NR | 7 | 25 | 2 | 2.56 ± 2.1 |
| Placebo gel | 30 | 27.8 ± 5.9 | NR | 7 | 21 | 2 | 1.78 ± 1.6 | |
| Mitchell | Moisturiser gel + placebo | 99 | 61.0 ± 4.0 | NR | NR | NR | NR | NR |
| Dual placebo | 98 | 61.0 ± 4.0 | NR | NR | NR | NR | NR | |
| Nappi | Monurelle Biogel gel | 48 | 55.8 ± 4.6 | NR | NR | NR | NR | NR |
| Placebo gel | 47 | 56.5 ± 5.9 | NR | NR | NR | NR | NR | |
| Tanmahasamut | Oestradiol gel | 38 | 54.9 ± 9.8 | NR | NR | NR | NR | NR |
| Placebo gel | 37 | 56.4 ± 4.5 | NR | NR | NR | NR | NR | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual function and dysfunction studies · Pelvic floor disorders treatments · Menstrual Health and Disorders
1. Introduction
Menopause is defined as the permanent cessation of menstruation for a minimum of 1 year.^1^ Postmenopausal women experience different physiological and psychological changes that can affect their daily life activities.^2^ The decline in oestrogen levels and hormonal fluctuations are associated with many postmenopausal changes, including vasomotor symptoms (such as hot flashes and night sweats), osteoporosis, vulvovaginal atrophy, sexual dysfunction and various psychological symptoms.^3^ Vaginal atrophy and dryness significantly contribute to sexual dysfunction and strongly impact sexual intimacy after menopause.^4^
Female sexual dysfunction (FSD) can arise from the disruption of any component of the sexual response cycle, including sexual physiology, emotions, experiences, beliefs, lifestyle and/or relationships.^5^ Women experiencing FSD are vulnerable to frequent genital infections, bleeding and chronic pain, all of which negatively impact their quality of life.^6^ After menopause, FSD may result from oestrogen deficiency and hormonal instability.^78^ A global study examining sexual attitudes and behaviours among 13,882 women aged 40 to 69 showed that one-third of the participants reported experiencing 1 or more problems related to their sexual function.^9^ The prevalence of vaginal dryness and dyspareunia in postmenopausal women was estimated to be 85% and 75%, respectively.^10^
Several treatment modalities are available to manage FSD and improve sexual satisfaction among postmenopausal women. Therapeutic options are classified into 2 groups: (1) topical hormonal replacement therapies (e.g. oestrogen and oxytocin preparations) and (2) natural herbs and non-hormonal therapies (e.g. chamomile and fennel preparations).^11^ Local vaginal preparations are preferred over systemic treatments due to their specific characteristics that promote efficacy and tolerability. This preference is especially crucial post-menopause for alleviating vaginal dryness. Achieving an optimally balanced osmolality and pH is essential for the effectiveness of these preparations.^12^
FSD affects one-third of women, especially younger women or those who are sexually active and is associated with various troublesome symptoms.^13^ The treatment of FSD syndrome depends on the safety profile and effectiveness of available therapies, as well as patient preferences.^14^ The term genitourinary syndrome of menopause (GSM) describes various complications associated with decreased levels of sex hormones, which lead to changes to the labia minora/majora, clitoris, vestibule/introitus, vagina, urethra and bladder.^15^ GSM is primarily characterised by genital symptoms (such as dryness, irritation and burning), sexual symptoms (including dyspareunia, dysfunction and lack of lubrication) and urinary symptoms (such as urgency, dysuria and recurrent urinary tract infections).^16^ Treatment options for GSM include hormonal therapies (both systemic and topical) and non-hormonal approaches (such as laser therapy and complementary and alternative medicine).^17^ The North American Menopause Society recommends the use of non-hormonal lubricants during sexual intercourse and long-acting vaginal moisturisers as needed.^18^ For symptomatic women with moderate to severe vulvovaginal atrophy or those who do not respond sufficiently to lubricants or moisturisers, oestrogen therapy – whether administered vaginally in low doses or systemically – is considered the therapeutic standard.^1819^
Hormonal therapy is a widely used treatment for the menopausal effects on the genitourinary tract.^420^ Oestrogen can be administered either orally or vaginally and is linked to a reduction in vaginal dryness, decreased vaginal atrophy and improved sexual function.^21^ Additionally, oxytocin is another effective hormonal treatment associated with enhanced sexual well-being and satisfaction.^2223^
On the other hand, several natural treatments may be effective for addressing sexual dysfunction. These include the herb Maca (Lepidium meyenii), fennel (Foeniculum vulgare), chamomile, aloe vera, 18β-glycyrrhizic acid, hyaluronic acid, liquorice and flaxseed.^24^ Additionally, non-hormonal treatment options, including the use of inactive lubricants – specifically water-, silicone- or oil-based lubricants – can be beneficial in reducing friction during sexual activity.^25^
Despite the abundance of studies focusing on postmenopausal women and sexual dysfunction, a notable literature gap persists in terms of a comprehensive comparison between hormonal (such as oestrogen and oxytocin) and non-hormonal (including fennel and chamomile) treatments.^2627^ Existing research tends to explore individual interventions, and there is a lack of direct head-to-head comparisons assessing their efficacy using a standardised and widely accepted measure, such as the Female Sexual Function Index (FSFI). Additionally, most studies often focus on either hormonal or non-hormonal treatments, making it challenging for clinicians and researchers to make informed decisions regarding the most effective approach for addressing sexual dysfunction in postmenopausal women.^2829303132^ A synthesis of the available evidence on these specific interventions and their direct comparison is essential for bridging this literature gap and providing valuable insights into the optimal management of postmenopausal sexual dysfunction.
This study aims to contribute significantly to the body of knowledge by conducting a systematic and comparative analysis of the most effective hormonal (oestrogen and oxytocin) and non-hormonal (fennel and chamomile) treatments for addressing sexual dysfunction in postmenopausal women. The inclusion of a well-established and reliable measure, such as the FSFI, will provide a standardised framework for evaluating the efficacy of these interventions, allowing for a more nuanced understanding of their impact on sexual satisfaction.^33^
By directly comparing these treatments, this study seeks to offer evidence-based recommendations for clinicians and healthcare providers, thereby facilitating informed decision-making when tailoring treatment plans for postmenopausal women experiencing sexual dysfunction. This research is anticipated to fill the existing literature gap by providing a comprehensive overview of both hormonal and non-hormonal options, ultimately guiding future research endeavours and clinical practices in the realm of postmenopausal sexual health. Consequently, this study has the potential to enhance the overall quality of care for postmenopausal women, addressing a critical aspect of their well-being and quality of life. Thus, the most effective hormonal (oestrogen and oxytocin) and non-hormonal (fennel and chamomile) preparations will be selected and compared in terms of efficacy, as measured by the FSFI, a widely recognised and reliable scale.
2. Methods
2.1. Review protocol
This meta-analysis was guided by the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.^3435^
2.2. Search strategy
This study systematically searched electronic databases, including PubMed, Scopus, Web of Science (WOS) and the Cochrane Central Register of Controlled Trials (CENTRAL), from their inception until January 2023. Search terms “vaginal gel”, “hormonal”, “estrogen”, “oxytocin”, “chamomile”, “fennel”, “female sexual dysfunction” and “postmenopausal” were included [Supplementary File]. All references for the included studies were screened to ensure that no relevant studies were overlooked and to guarantee a high-quality review process. Furthermore, Clinicaltrials.gov and the World Health Organization Clinical Trials Registry were consulted to identify unpublished and ongoing trials.
2.3. Eligibility criteria
Studies that met all of the following preselected criteria were included: (i) the studies must enrol a postmenopausal population with FSD; (ii) the intervention must be a gel-based hormonal or non-hormonal preparation; (iii) only placebo-controlled trials were eligible, and all other trials with active interventions were excluded; (iv) studies must report all domains and the total score of FSFI to be included in the meta-analysis; (v) to generate stronger evidence, only randomised controlled trials (RCTs) were included. Conversely, non-human studies, conference abstracts, non-RCTs, cohorts, case-control studies, case series and non-English studies were excluded.
2.4. Screening and study selection
Different records from various databases were collected using Endnote software; duplicates were removed. The retrieved references were screened to assess their relevance through a 2-step process: first, title and abstract screening, followed by full-text screening for final eligibility; 2 independent authors (AS and RG) completed the task and resolved any conflicts with the assistance of a senior author (HA).
2.5. Quality assessment
Using the Cochrane Risk of Bias (ROB) assessment tool, 2 authors (MM and AS) independently evaluated each included study.^36^ The following domains were assessed: the randomisation process, deviations from the intended interventions, missing outcome data, measurement of the outcomes and selection of the reported results. Each domain, as well as the overall quality of the included studies, was classified as having a ‘low’, ‘some concerns’ or ‘high’ risk of bias. A low risk of bias indicates adequate randomisation, minimal or no evidence of systematic differences between groups, a small amount of missing data, the use of objective, reliable and valid measurement methods and the reporting of pre-specified outcomes. Some concerns suggest an unclear description of the randomisation process, differences in care between groups that do not lead to bias, some missing data, minor issues with measurement methods and discrepancies between pre-specified and reported outcomes. Conversely, a high risk of bias indicates inadequate randomisation, the presence of systematic differences in care between groups, a high amount of missing data, measurement methods likely to introduce bias and post hoc changes in outcomes. Generally, the presence of one high-risk domain results in an overall high risk of bias for the study. Conversely, if there are concerns in any domain, the overall quality is classified as having some concerns.^37^ Disagreements were resolved through group discussion. According to Egger et al., publication bias is unreliable when fewer than 10 studies are pooled.^38^ Therefore, this review could not assess the existence of publication bias using Egger's test for funnel plot asymmetry.
2.6. Data extraction and outcomes
The following data were extracted by 2 independent authors (DL and AS): (i) study-relevant data, including location, year of publication, sample size, study design and follow-up duration; (ii) data related to enrolled study participants, such as mean age, mean age at menopause, body mass index (BMI), economic status and coitus frequency; (iii) data regarding the intervention, including preparation base, category (hormonal/non-hormonal), active ingredients, treatment period and application schedule; and (iv) FSFI-reported data encompassing all six domains (sexual desire, arousal, lubrication, orgasm, satisfaction and pain) as well as the overall total score collected at both baseline and endpoint.
2.7. Statistical analysis
A meta-analysis was performed using ReviewManager software (RevMan, Version 5.3 for Windows), provided by the Cochrane Collaboration in 2014, Nordic Cochrane Centre, Copenhagen, Denmark.^39^ All extracted data were continuous and pooled as mean differences (MD) with a 95% confidence interval (CI). The analyses utilised the inverse variance method and the random-effects model. Heterogeneity was assessed by examining the graphs on forest plots and measured using Chi-square and I^2^ tests to determine the degree of heterogeneity. Significant heterogeneity was defined as a Chi-square test with P < 0.1 and an I^2^ test >50. Endpoints with a P value <0.05 were considered statistically significant.^40^ This review subgrouped the included studies according to the nature of their interventions into hormonal (oestrogen and oxytocin) and non-hormonal (chamomile and fennel) preparations.
3. Results
3.1. Literature search
The comprehensive search strategy yielded 982 search results. After removing duplicates, 366 unique results were eligible for the first screening. Based on a review of the titles and abstracts, 349 articles were excluded. Ultimately, 17 full-text articles were retrieved to assess their adherence to the predetermined selection criteria. Finally, the authors agreed on including 8 RCTs. After manually checking the included studies’ reference lists, no missed publications were found [Fig. 1].
Flow chart showing using the preferred reporting items for systematic reviews and meta-analyses to show study selection.
3.2. Characteristics of the included trials
In 8 RCTs conducted with a total of 672 postmenopausal women, 341 participants were allocated to the intervention group (gel group), whereas 331 women were placed in the placebo group.^2841424344454647^ Hormonal preparations were used in 4 trials, specifically oestrogen or oxytocin gel interventions, while the remaining 4 RCTs employed non-hormonal preparations, such as chamomile and fennel [Table 1].
All interventions were administered for 12 weeks, except for 3 trials, which applied their preparations for 8 weeks.^284345^ The average age of the participating women was 52.6 years, and the average age at menopause was 49.9 years. Among the enrolled participants, 57% reported their economic status as ‘good’, while 29% and 14% classified their status as ‘weak’ and ‘high’, respectively. The average frequency of coitus among participants was 2 times per week [Table 2].
3.3. Quality assessment
A total of 4 RCTs were evaluated as having a ‘low’ risk of bias.^43444547^ Conversely, 2 RCTs were classified as having an ‘unclear’ risk of bias due to concerns regarding the lack of information about study personnel blinding.^2842^ Additionally, 2 funded RCTs were rated as having a ‘high’ risk of bias;^4146^ one was attributed to missing data and insufficient information regarding blinding, while the other trial failed to provide details about the randomisation process and allocation concealment [Supplementary Figures 1 and 2].
3.4. Meta-analysis of the overall female sexual function index score
The study results indicated a statistically significant difference between the vaginal gel and placebo groups. Both the total FSFI endpoint score (MD = 6.67, 95% CI: 3.79–9.55; P < 0.001) and the change from baseline (MD = 4.89, 95% CI: 3.19–6.59; P < 0.001) were significantly increased in the vaginal gel group. A subgroup analysis based on the nature of the interventions revealed that non-hormonal gel preparations resulted in a significant increase in FSFI scores, with a higher MD (MD = 6.73, 95% CI: 4.7–8.76; P < 0.001) compared to hormonal gel preparations (MD = 2.75, 95% CI: 1.87–3.64; P < 0.001) [Fig. 2]. While both hormonal and non-hormonal preparations were effective in enhancing the total FSFI score, studies using hormonal gel products showed no significant heterogeneity. In contrast, studies involving non-hormonal interventions, which incorporated various chemical and herbal active ingredients such as fennel and chamomile, exhibited notable diversity.
Meta-analysis of change (pre-/post-interventional) in the total score of the female sexual function index.SD = standard deviation; CI = confidence interval.
3.5. Changes in the desire domain
Results for the sexual desire domain indicated a statistically significant difference between the vaginal gel and placebo groups. The total change from baseline was notably greater in the vaginal gel group (MD = 0.92, 95% CI: 0.34–1.51; P = 0.002) [Supplementary Figure 3]. The subgroup analysis displayed that non-hormonal gel preparations substantially increased female sexual desire (MD = 1.32, 95% CI: 0.54–2.11; P = 0.001) compared to oestrogen and oxytocin gel preparations (MD = 0.53, 95% CI: 0.22–0.84; P < 0.001). Both hormonal and non-hormonal preparations were effective in achieving higher sexual desire scores; however, there was homogeneity among studies using hormonal gel preparations, unlike the studies with different non-hormonal products.
3.6. Changes in the arousal domain
The sexual arousal domain of the FSFI revealed a notable statistical difference between the vaginal gel and placebo groups. The difference from baseline was considerably higher in the vaginal gel group (MD = 1.41, 95% CI: 0.67–2.15; P < 0.001) [Supplementary Figure 4]. The subgroup analysis indicated that hormonal gel products improved sexual arousal (MD = 1.45, 95% CI: 0.31–2.48; P = 0.02) more effectively than their non-hormonal counterparts (MD = 1.40, 95% CI: 0.21–2.68; P = 0.01). Both the hormonal and non-hormonal preparations were effective in achieving higher levels of sexual arousal, and there was no notable heterogeneity among studies (I^2^ = 24%; P < 0.001).
3.7. Changes in the lubrication domain
Results in the sexual lubrication domain demonstrated a statistically significant difference between the vaginal gel and placebo groups. The change from baseline was greater in the vaginal gel group (MD = 1.36, 95% CI: 0.45–2.27; P = 0.003) [Supplementary Figure 5]. However, the subgroup analysis demonstrated that hormonal preparations did not have a statistically significant effect on lubrication (MD = 0.78, 95% CI: -0.11–1.67; P = 0.08). Conversely, non-hormonal products were found to be highly effective (MD = 1.76, 95% CI: 0.23–3.28; P = 0.02). Additionally, both hormonal and non-hormonal studies exhibited considerable within-group heterogeneity (I^2^ = 97%; P < 0.001).
3.8. Changes in the orgasm domain
Results indicated a significant statistical difference between the vaginal gel and placebo groups. The change from baseline in the orgasm domain was greater in the vaginal gel group than in the placebo group (MD = 0.87, 95% CI: 0.29–1.46; P = 0.003) [Supplementary Figure 6]. Nevertheless, the subgroup analysis showed that non-hormonal products were more effective (MD = 1.16, 95% CI: 0.44–1.89; P = 0.002) than hormonal gel interventions (MD = 0.45, 95% CI: -0.53–1.43; P = 0.37). However, there was significant heterogeneity among the studies in both the hormonal and non-hormonal groups (I^2^ = 92%; P < 0.001).
3.9. Changes in the satisfaction domain
Results in the sexual satisfaction domain showed a statistically significant variation between the vaginal gel and the placebo, as the change from baseline was greater in the placebo group (MD = 1.10, 95% CI: 0.63–1.57; P < 0.001) [Supplementary Figure 7]. Further subgroup analysis indicated that women who used non-hormonal preparations reported higher satisfaction (MD = 1.34, 95% CI: 0.78–1.90; P < 0.001) than those who used hormonal ones (MD = 0.68, 95% CI: 0.32–1.05; P < 0.001). Although both types of preparations were effective in improving sexual satisfaction, there was no remarkable heterogeneity among studies that used hormonal gel products, unlike studies that employed non-hormonal interventions (I^2^ = 91%; P < 0.001).
3.10. Changes in the pain domain
The results of the sexual pain domain indicated a substantial difference between the vaginal gel and the placebo. The change from baseline was greater in the vaginal gel group than in the placebo (MD = 1.60, 95% CI: 1.27–1.94; P < 0.001) [Supplementary Figure 8]. Subgroup analysis showed that both hormonal (MD = 1.17, 95% CI: 0.19–2.14; P = 0.02) and non-hormonal (MD = 1.68, 95% CI: 1.28–2.08; P < 0.001) treatments were effective in reducing pain among postmenopausal women with sexual satisfaction. Hormonal studies exhibited no notable heterogeneity, while non-hormonal studies demonstrated significant within-group heterogeneity (I^2^ = 66%; P = 0.004).
3.11. Leave-one-out sensitivity analysis
By visualising all the forest plots, this review identified Nappi et al.^46^ and Abedi et al.^42^ as outliers in most forest plots. Consequently, a leave-one-out sensitivity analysis was performed for all outcomes by excluding both studies. After their removal, the results remained stable across all outcomes except in the lubrication and pain domains.
In the total score of FSFI (MD = 5.06, 95% CI: 2.94–7.18; P < 0.00001) and the sexual desire domain (MD = 1.12, 95% CI: 0.47–1.77; P = 0.0007), the overall results remained significant. However, heterogeneity was not resolved (I^2^ = 95%; P < 0.00001 and I^2^ = 90%; P < 0.00001, respectively) [Supplementary Figures 9 and 10].
The same pattern was observed in the overall results of sexual arousal (MD = 1.74, 95% CI: 0.85–2.64; P = 0.0001), sexual orgasm (MD = 1.01, 95% CI: 0.25–1.77; P = 0.009) and sexual satisfaction (MD = 1.4, 95% CI: 0.95–1.86; P < 0.00001) domains, which were statistically significant. However, the issue of heterogeneity remained unresolved (I^2^ = 98%; P < 0.00001, I^2^ = 93%; P < 0.00001 and I^2^ = 88%; P < 0.00001, respectively) [Supplementary Figures 11–13].
In the domains of sexual lubrication (MD = 1.5, 95% CI: 0.2–2.8; P = 0.02) and pain (MD = 1.7, 95% CI: 1.32–2.08; P < 0.00001), the overall results were significant. The results also exhibited heterogeneity (I^2^ = 98%; P < 0.00001 and I^2^ = 69%; P = 0.007, respectively). However, the heterogeneity disappeared from the hormonal gel subgroup for both outcomes (I^2^ = 0%; P = 0.42 and I^2^ = 0%; P = 0.45, respectively) [Supplementary Figures 14 and 15].
4. Discussion
This meta-analysis aimed to systematically review the published literature on the efficacy of vaginal gel preparations compared to placebo in the treatment of sexual dysfunction syndrome. A total of 982 articles were identified and 8 were selected that contained data pertaining to the use of vaginal gel in postmenopausal women. The findings indicated a significant difference between the vaginal gel and placebo groups, with the vaginal gel group showing an increased FSFI endpoint score and a notable change from baseline.
The observed statistically significant improvements in overall FSFI scores, including sexual desire, arousal, lubrication, orgasm, satisfaction and pain domains, following vaginal gel interventions, suggest a potential avenue for addressing sexual dysfunction in postmenopausal women. These findings align with existing literature that highlights the physiological changes associated with menopause, which can adversely affect sexual function.^4849^ The positive effects demonstrated by both hormonal and non-hormonal gel preparations indicate a promising range of options to meet the diverse needs and preferences of postmenopausal women.
Fernandes et al. assessed the effectiveness of topical oestrogen as a vaginal lubricant in improving the sexual function of the included females.^28^ They noticed a positive trend in improved sexual function among women using oestrogen-conjugated cream. Oestrogen is well-absorbed in the vagina due to its highly vascularised nature, which also allows absorbed oestrogen to bypass enterohepatic circulation, leading to fewer adverse effects. Similar results are reported in the literature. Tanmahasamut et al. evaluated the efficacy and safety of oestradiol gel on postmenopausal vaginal tissue.^47^ They found that postmenopausal women treated with oestradiol vaginal gel were able to reverse vaginal atrophy. Oestradiol administered vaginally also demonstrated a high safety profile with low systemic absorption. Palacios et al. evaluated the effects of combined therapy using vaginal oestriol with transdermal 17-beta-oestradiol plus medroxyprogesterone acetate.^50^ They found that incorporating vaginal oestriol into hormone replacement therapy may lead to a shorter latency for urinary symptoms associated with vulvovaginal atrophy. Similarly, Nachtigall found that menopausal women treated with vaginal oestrogen cream exhibited significantly increased vaginal moisture, fluid volume and elasticity, in addition to returning to the premenopausal pH state.^51^
Another hormone that has been recently studied to treat sexual dysfunction is oxytocin. Despite some adverse effects, oxytocin offers many benefits, including natural cell growth stimulation and accelerating healing processes. Additionally, it has been shown to improve sexual satisfaction in women when administered intranasally.^52535455^ However, Mesbahi et al. found no significant difference between oxytocin gel and placebo regarding FSFI total score.^44^ Nevertheless, an improvement in the sexual satisfaction domain was observed, along with enhanced symptoms of depression compared to the placebo group. Abedi et al. reported improved sexual function in postmenopausal women using vaginal oxytocin gel compared to a placebo.^41^
Another method that has been gaining popularity is using complementary and alternative medicine, particularly herbal medicine.^56^ Multiple studies have examined the use of medicinal plants to treat menopausal symptoms. These plants include soybean, red clover, chamomile, fennel, black cohosh, Pueraria mirifica, flaxseed and liquorice, among others.^575859^ For instance, Bosak et al. investigated the effect of chamomile vaginal gel on the sexual function of postmenopausal women.^43^ Chamomile has been used in both traditional and modern medicine due to its phyto-oestrogen/oestrogenic properties. The chamomile flower is widely recognised for its benefits in alleviating various pathological disorders, including inflammation, cardiovascular and gastrointestinal diseases, cancer, the common cold, abdominal pain, diarrhoea, haemorrhoids, mucositis, osteoporosis, insomnia, anxiety, seizures, diabetes, sore throat, vaginitis and premenopausal syndrome, among others.^5860^
Phyto-oestrogens can bind to oestrogen receptors in the body, exerting their oestrogenic effects more potently. In postmenopausal women, this may lead to a reduction in menopausal symptoms, including hot flashes and vaginal dryness.^61^
Yaralizadeh et al. investigated the effects of fennel vaginal cream on sexual function in postmenopausal women.^57^ F. vulgare, commonly known as fennel, is a plant belonging to the carrot family and is widely found along the shores of the Mediterranean Sea. The main chemical compounds in fennel are trans-anethole and dianethole, both of which exhibit oestrogenic properties.^62^ These compounds are recognised for their potential to influence the hormonal environment in postmenopausal women. The inclusion of fennel in vaginal cream formulations represents a novel approach, leveraging its natural properties to address sexual function concerns within this specific population.^41^ The geographical prevalence of fennel in the Mediterranean region adds a contextual layer to the study, considering the potential influence of regional dietary and lifestyle factors on the outcomes.^63^ This geographical connection may also have implications for the generalisability of the findings, prompting future research to explore the cultural and environmental factors that could impact the efficacy of fennel-based interventions in diverse populations. Moreover, the choice of fennel as a therapeutic agent aligns with the growing interest in botanical remedies for menopausal symptoms.^64^ Understanding the oestrogenic effects of trans-anethole and dianethole in fennel elucidates the potential mechanisms through which fennel vaginal cream may influence sexual function, providing a scientific basis for its application.
The subgroup analysis emphasising the differential impact of hormonal and non-hormonal gel preparations on various domains of sexual function is a critical aspect of this discussion. Non-hormonal preparations, which incorporate ingredients such as chamomile and fennel, showed greater efficacy in enhancing sexual desire, lubrication, orgasm and overall satisfaction. Conversely, hormonal gel products appeared to be more effective in improving sexual arousal. This distinction is noteworthy, suggesting that tailoring interventions to address specific aspects of sexual function may optimise treatment outcomes. Understanding the underlying mechanisms and interactions of these different compositions could guide future research and clinical practice.
Nearly all the outcomes exhibited some degree of heterogeneity that was not resolved by either a leave-one-out test or subgroup analysis. This heterogeneity may be related to several factors: (1) the baseline characteristics of the included patients, as all studies included postmenopausal women except for Nappi et al.,^46^ which included women over 18 years with the potential for childbearing, and Mesbahi et al.,^44^ which included breastfeeding healthy women; (2) variations in active ingredients among the studies; (3) differences in formulations, as all studies used a gel formulation except for Abedi et al.^41^ and Fernandes et al.,^28^ which employed a cream formulation, and Mitchell et al.,^45^ which used a vaginal tablet; and (4) application frequency where some studies instructed participants to apply their interventions once daily, while recommended application is 2–3 times per week.
The findings of this meta-analysis have significant implications for healthcare providers involved in the care of postmenopausal women experiencing sexual dysfunction. The identification of effective interventions, particularly the observed benefits of non-hormonal gel preparations, opens avenues for personalised and patient-centred care. By recognising the diversity in women's needs and preferences, clinicians can engage in informed discussions with patients to select interventions that align with individual circumstances, potentially improving treatment adherence and satisfaction. In future, researchers should consider conducting long-term follow-up studies to assess the sustained effects of vaginal gel interventions on postmenopausal women's sexual function. Additionally, investigating the safety profile of these interventions, especially hormonal preparations, is crucial for providing a comprehensive understanding of the associated risks and benefits.
4.1. Strengths and limitations
To the best of the Authors' knowledge, this is the first meta-analysis that compiles pooled evidence about hormonal and non-hormonal vaginal gel products. This article emphasises the real-world efficacy of these topical preparations in assisting postmenopausal women with FSD syndrome resulting from different types of pathology. However, due to the diverse nature of these interventions, nearly all the pooled analyses exhibited heterogeneity. In addition, 4 of the included studies were conducted in the same location (Iran), which may affect the generalisability of this study's findings.
5. Conclusion
Chamomile and fennel vaginal gel preparations can significantly enhance the overall score of FSFI and its 6 domains. Except for the lubrication and orgasm domains, oestrogen and oxytocin hormonal gel preparations can also improve the total FSFI score and its respective domains. Based on these findings, this review suggests offering both hormonal and non-hormonal gel products to boost sexual function and activity in postmenopausal women with FSD syndrome.
Ethics Statement
Ethical approval was not required due to the nature of the study, and the study protocol was registered in the Open Science Framework (registration code: zbwu3).
Authors' Contributions
AS led the team, performed data collection, resolved conflicts during the screening process and quality assessment, performed the meta-analysis and contributed to writing and editing the final manuscript. HA participated in the screening process, quality assessment and draft writing. MAM took part in the quality assessment and draft writing. RG contributed to the screening process, data extraction and draft writing. ASAA edited the manuscript. NAR revised the article. YAM critically revised and edited the manuscript and assessed the quality of evidence using the GRADE system. AHS supervised the authors throughout all steps and performed the final revision. All authors approved the final version of the manuscript.
Data Availability
Data is available upon reasonable request from the corresponding author.
Supplementary Data
Supplementary data to this article can be found online at https://doi.org/10.18295/squmj.6.2024.00.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Butler L Santoro N. The reproductive endocrinology of the menopausal transition. Steroids 2011; 76:627–35. https://doi.org/10.1016/j.steroids.2011.02.026.10.1016/j.steroids.2011.02.02621419147 PMC 3100375 · doi ↗ · pubmed ↗
- 2Mc Kinlay SM Brambilla DJ Posner JG. The normal menopause transition. Am J Hum Biol 1992; 4:37–46. https://doi.org/10.1002/ajhb.1310040107.10.1002/ajhb.131004010728524413 · doi ↗ · pubmed ↗
- 3Dalal P Agarwal M. Postmenopausal syndrome. Indian J Psychiatry 2015; 57:S 222–32. https://doi.org/10.4103/0019-5545.161483.10.4103/0019-5545.16148326330639 PMC 4539866 · doi ↗ · pubmed ↗
- 4Sturdee DW Panay N. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric 2010; 13:509–22. https://doi.org/10.3109/13697137.2010.522875.10.3109/13697137.2010.52287520883118 · doi ↗ · pubmed ↗
- 5Lee A Kim TH Lee HH Kim YS Enkhbold T Lee B. Therapeutic approaches to atrophic vaginitis in postmenopausal women: A systematic review with a network meta-analysis of randomized controlled trials. J Menopausal Med 2018; 24:1–10. https://doi.org/10.6118/jmm.2018.24.1.1.10.6118/jmm.2018.24.1.129765921 PMC 5949302 · doi ↗ · pubmed ↗
- 6Nazarpour S Simbar M Ramezani Tehrani F Alavi Majd H. Quality of life and sexual function in postmenopausal women. J Women Aging 2018; 30:299–309. https://doi.org/10.1080/08952841.2017.1395539.10.1080/08952841.2017.139553929077541 · doi ↗ · pubmed ↗
- 7Morali G Polatti F Metelitsa E Mascarucci P Magnani P Brunenghi Marrè G. Open, non-controlled clinical studies to assess the efficacy and safety of a medical device in form of gel topically and intravaginally used in postmenopausal women with genital atrophy. Arzneimittelforschung 2011; 56:230–38. https://doi.org/10.1055/s-0031-1296715.10.1055/s-0031-129671516618016 · doi ↗ · pubmed ↗
- 8Cotreau MM Chennathukuzhi VM Harris HA Han L Dorner AJ Apseloff G. A study of 17β-estradiol-regulated genes in the vagina of postmenopausal women with vaginal atrophy. Maturitas 2007; 58:366–76. https://doi.org/10.1016/j.maturitas.2007.09.009.10.1016/j.maturitas.2007.09.00917997058 · doi ↗ · pubmed ↗