Urinary Tract Infections Among Patients in Primary Healthcare Centres in Bahrain: A cross-sectional study
Mahmood Alawainati, Zahra Ayoob, Eman Almajed, Safaa Alkhawaja, Noof Abdulaal, Rehab Alkhnaizi, Hanin Shaheen, Fatema Hubail, Nermin Kamal Saeed

TL;DR
This study analyzed urinary tract infections in Bahrain's primary healthcare centers, finding high rates of antibiotic-resistant bacteria, especially in older patients and those with certain risk factors.
Contribution
The study provides new insights into the prevalence of resistant uropathogens in primary care settings in Bahrain and identifies key risk factors for resistance.
Findings
Escherichia coli and Klebsiella were the most common uropathogens in UTIs.
About 20.8% of patients had resistant uropathogens, with ESBL being the most prevalent.
Older patients, those with antibiotic use, hospitalization, or ESBL history had higher resistance rates.
Abstract
This study aimed to determine the clinical and microbiological profiles of patients with urinary tract infections (UTIs) in primary healthcare centres in Bahrain. This retrospective cross-sectional study was conducted at 27 primary care centres in Bahrain between January and December 2022. All patients with positive urine cultures, defined as the presence of ≥100,000 colony-forming units/mL were included. Participants' sociodemographic characteristics, comorbidities, risk factors for resistant uropathogens, uropathogen types and antibiotic sensitivity outcomes were assessed. Descriptive and inferential statistics were analysed. A total of 1,985 patients were included, with an average age of 40.57 ± 20.18 years. Most participants were female (n = 1,802, 90.8%) and Bahraini (n = 1,699, 85.6%). Diabetes mellitus (20.1%) and hypertension (17.9%) were the most prevalent comorbidities among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
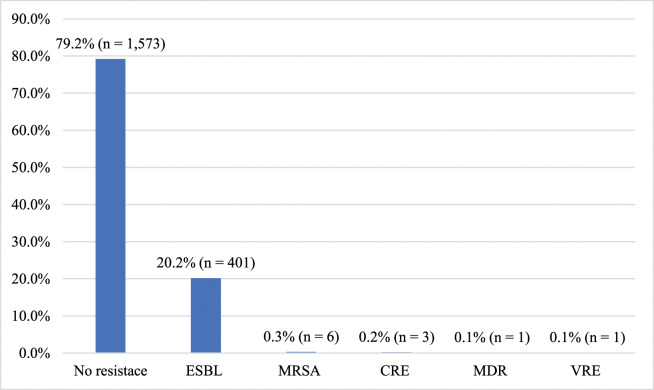 Fig. 1
Fig. 1| Characteristic | n (%) |
|---|---|
|
| 40.57 ± 20.18 |
|
| |
| <18 | 159 (8.0) |
| 18–64 | 1,492 (75.2) |
| ≥65 | 332 (16.7) |
|
| |
| Male | 183 (9.2) |
| Female | 1,802 (90.8) |
|
| |
| Bahraini | 1,699 (85.6) |
| Non-Bahraini | 286 (14.4 |
|
| |
| Diabetes mellitus | 399 (20.1) |
| Hypertension | 356 (17.9) |
| Renal stone | 61 (3.1) |
| Sickle cell disease | 28 (1.4) |
| Genitourinary anomalies | 28 (1.4) |
| Cancer | 22 (1.1) |
|
| |
| Antibiotic use in last 3 months | 645 (32.5) |
| History of extended-spectrum β-lactamase | 224 (11.3) |
| Hospitalisation in last 3 months | 93 (4.7) |
| History of other resistant bacteria | 23 (1.2) |
| On Foley's catheter | 3 (0.2) |
| n (%) | ||||
|---|---|---|---|---|
|
| ||||
| Age group in years | ||||
|
| ||||
| Organism | Total | <18 | 18–64 | ≥65 |
|
| 1,220 (61.5) | 111 (69.8) | 901 (60.4) | 206 (62) |
|
| 342 (17.2) | 28 (17.6) | 250 (16.8) | 64 (19.3) |
|
| 154 (7.8) | 3 (1.9) | 138 (9.2) | 13 (3.9) |
|
| 75 (3.8) | 4 (2.5) | 55 (3.7) | 16 (4.8) |
|
| 59 (3.0) | 3 (1.9) | 44 (2.9) | 12 (3.6) |
|
| 45 (2.3) | 4 (2.5) | 39 (2.6) | 2 (0.6) |
|
| 37 (1.9) | 3 (1.9) | 33 (2.2) | 1 (0.3) |
|
| 17 (0.9) | 1 (0.6) | 8 (0.5) | 8 (2.4) |
| n (%) | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Amoxicillin/ | Trimethoprim/ | |||||
| Organism | Nitrofurantoin | clavulanate | Cephalothin | Cefuroxime | sulfamethoxazole | Ciprofloxacin |
|
| ||||||
| Sensitive | 1,199 (98.3) | 827 (67.8) | 754 (61.8) | 841 (68.9) | 865 (70.9) | 972 (79.7) |
| Resistant | 21 (1.7) | 392 (32.1) | 463 (38) | 377 (30.9) | 354 (29) | 245 (20.1) |
| Not done | 0 (0) | 1 (0.1) | 3 (0.2) | 2 (0.2) | 1 (0.1) | 3 (0.2) |
|
| ||||||
| Sensitive | 228 (66.7) | 267 (78.1) | 264 (77.2) | 273 (79.8) | 269 (78.7) | 314 (91.8) |
| Resistant | 113 (33) | 74 (21.6) | 77 (22.5) | 68 (19.9) | 72 (21.1) | 27 (7.9) |
| Not done | 1 (0.3) | 1 (0.3) | 1 (0.3) | 1 (0.3) | 1 (0.3) | 1 (0.3) |
|
| ||||||
| Sensitive | NA | NA | NA | NA | NA | 60 (80) |
| Resistant | 12 (16) | |||||
| Not done | 3 (4) | |||||
|
| ||||||
| Sensitive | NA | NA | NA | NA | NA | 16 (94.1) |
| Resistant | 1 (5.9) | |||||
| Not done | 0 (0) | |||||
|
| ||||||
| Sensitive | 375 (91) | 8 (1.9) | 8 (1.9) | 9 (2.2) | 190 (46.1) | 248 (60.2) |
| Resistant | 35 (8.5) | 396 (96.1) | 396 (96.1) | 394 (95.6) | 219 (53.2) | 162 (39.3) |
| Not done | 2 (0.5) | 8 (1.9) | 8 (1.9) | 9 (2.2) | 3 (0.7) | 2 (0.5) |
| n (%) | |||
|---|---|---|---|
|
| |||
| Non-resistant | Resistant | ||
| Characteristic | uropathogens (n = 1,573) | uropathogens (n = 412) | |
|
| 39.15 ± 19.62 | 46.00 ± 21.33 | <0.001 |
|
| 0.085 | ||
| Male (n = 183) | 136 (74.3) | 47 (25.7) | |
| Female (n = 1,802) | 1,437 (79.7) | 365 (20.3) | |
|
| 0.710 | ||
| Bahraini (n = 1,699) | 1,344 (79.1) | 355 (20.9) | |
| Non-Bahraini (n = 286) | 229 (80.1) | 57 (19.9) | |
|
| <0.001 | ||
| Yes (n = 399) | 288 (72.2) | 111 (27.8) | |
| No (n = 1,586) | 1,285 (81.0) | 301 (19) | |
|
| <0.001 | ||
| Yes (n = 356) | 251 (70.5) | 105 (29.5) | |
| No (n = 1,629) | 1,322 (81.2) | 307 (18.8) | |
|
| 0.577 | ||
| Yes (n = 28) | 21 (75.0) | 7 (25.0) | |
| No (n = 1,957) | 1,552 (79.3) | 405 (20.7) | |
|
| 0.287 | ||
| Yes (n = 22) | 20 (90.9) | 2 (9.1) | |
| No (n = 1,963) | 1,553 (79.1) | 410 (20.9) | |
|
| 0.157 | ||
| Yes (n = 28) | 19 (67.9) | 9 (32.1) | |
| No (n = 1,957) | 1,554 (79.4) | 403 (20.6) | |
|
| 0.832 | ||
| Yes (n = 61) | 49 (80.3) | 12 (19.7) | |
| No (n = 1,924) | 1,524 (79.2) | 400 (20.8) | |
|
| 0.503 | ||
| Yes (n = 3) | 2 (66.7) | 1 (33.3) | |
| No (n = 1,982) | 1,571 (79.3) | 411 (20.7) | |
|
| <0.001 | ||
| Yes (n = 645) | 459 (71.2) | 186 (28.8) | |
| No (n = 1,339) | 1,113 (83.1) | 226 (16.9) | |
|
| <0.001 | ||
| Yes (n = 93) | 54 (58.1) | 39 (41.9) | |
| No (n = 1,892) | 1,519 (80.3) | 373 (19.7) | |
|
| <0.001 | ||
| Yes (n = 224) | 118 (52.7) | 106 (47.3) | |
| No (n = 1,761) | 1,455 (82.6) | 306 (17.4) | |
| History of carbapenem-resistant | 0.019 | ||
| Yes (n = 6) | 2 (33.3) | 4 (66.7) | |
| No (n = 1,979) | 1,571 (79.4) | 408 (20.6) | |
| Characteristic | OR (95% CI) | |
|---|---|---|
| Age | 0.989 (0.982–0.996) | 0.002 |
| Diabetes mellitus | 0.936 (0.665–1.316) | 0.702 |
| Hypertension | 1.069 (0.734–1.558) | 0.726 |
| Antibiotic use in the last 3 months | 1.470 (1.156–1.871) | 0.002 |
| Hospitalisation in the last 3 months | 1.762 (1.106–2.807) | 0.017 |
| History of extended-spectrum β-lactamase uropathogens | 3.347 (2.468–4.540) | <0.001 |
| History of carbapenem-resistant | 4.571 (0.789–26.491) | 0.090 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Global Health Care Issues
1. Introduction
Urinary tract infections (UTIs) are prevalent and important infections commonly encountered in primary healthcare settings. UTIs affect females more frequently than males; nearly two-thirds of women will experience a UTI at some point in their lives. These infections can range from uncomplicated cystitis to complicated pyelonephritis. The disparity in UTI rates between sexes is attributed to anatomical differences, such as a shorter urethra and the proximity of the anus, as well as hormonal changes between males and females.^12^
Although the causative organisms of UTIs, known as uropathogens, vary based on patient characteristics, Escherichia coli remains the most common causative agent, followed by Klebsiella, Proteus, Enterobacter and Enterococcus.^3^ The pathogenesis of UTIs begins with the colonisation of uropathogens in the periurethral area. This is followed by the ascension of these pathogens through the urethra to the bladder, where they bind to bladder epithelial cells and manifest clinically.^4^ While most cases of UTIs are uncomplicated and involve only the lower urinary tract (bladder and urethra), diabetes mellitus, structural genitourinary abnormalities, recent antibiotic use, hospitalisation and urinary catheterisation increase the risk of resistant infections and upper UTIs.^5^
There has been a global increase in the number of resistant uropathogens. The literature indicates that the rates of extended-spectrum β-lactamase (ESBL) Enterobacterales and carbapenem-resistant Enterobacterales (CRE) have been increasing over the past few decades. A review found that the prevalence of ESBL ranges from 2% to 45%.^6^ ESBL and CRE are the main resistant uropathogens, as noted in many studies. Other resistant uropathogens include methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococci.^78^
Risk factors for resistant uropathogens include advanced age, recent antibiotic use (within the past 3–6 months), male sex, a history of UTIs and urinary catheterisation.^910^ Additionally, patients who have been hospitalised recently (within the past month), those with diabetes mellitus, cardiac diseases and genitourinary anomalies are at a higher risk of developing resistant uropathogens.^1112^
Antibiotics remain the cornerstone of treating UTIs, with nitrofurantoin, trimethoprim-sulfamethoxazole and fosfomycin being the preferred choices in most cases. However, due to the increasing prevalence of antibiotic resistance, the Infectious Diseases Society of America recommends periodically assessing local sensitivity patterns to determine the most effective antibiotic regimens for UTIs. Resistant uropathogens, including ESBL, CRE and multidrug-resistant organisms, exhibit varying antibiotic sensitivity profiles.^1314^
In Bahrain, several studies have been conducted to assess the most common uropathogens and their sensitivity profiles in secondary care settings.^151617^ According to these studies, E. coli and Klebsiella were identified as the most common uropathogens. Additionally, resistant uropathogens were prevalent among affected patients, with ESBL uropathogens being the most common type (27.4%). The MRSA was detected in nearly 10% of the isolates in these studies.^1516^ However, none of these studies assessed patients' demographic characteristics, risk factors, comorbidities or sensitivity profiles in primary healthcare facilities.^17^ The current study aimed to determine the characteristics of patients with UTIs, identify the most common organisms causing UTIs and analyse their antibiotic sensitivity outcomes, along with the prevalence, risk factors and sensitivity outcomes of patients with resistant uropathogens.
2. Methods
This retrospective cross-sectional study was conducted across 27 primary care centres distributed among 4 governorates in Bahrain. All centres were included in this study. Data collection occurred between January and December 2022.
All patients in the primary care centres with positive urine cultures were included in the study. For patients with recurrent UTIs, details of the first episode were collected. Since all positive cases were included, a sample size calculation was not necessary. The data on positive cultures were obtained from the central laboratory.
A positive culture was defined as the presence of ≥100,000 colony-forming units/mL. All diagnoses were based on the International Classification of Diseases, 10th Revision. To assess antibiotic sensitivity, the matrix-assisted laser desorption/ionisation mass spectrometry method was used for identification and disc diffusion testing. ESBL-producing organisms were detected using double-disc synergy testing.
The researchers reviewed the medical records of positive cases and documented the information for each case using a specialised data collection form created by the researchers. Participants' sociodemographic characteristics, comorbidities, risk factors for resistant uropathogens, uropathogens and antibiotic sensitivity outcomes were retrieved anonymously from the electronic medical records.
Frequencies and percentages were used to illustrate qualitative variables, while means and standard deviations were used to present quantitative variables. Chi-square tests or Fisher's exact tests were applied as appropriate to compare categorical variables across different groups, while t-tests were used to compare continuous variables. Binary logistic regression analysis was performed. All data were analysed using Statistical Package for the Social Sciences (SPSS) software, Version 23.0 (IBM Corp., Armonk, New York, USA).
3. Results
A total of 1,985 patients were included in the study, with an average age of 40.57 ± 20.18 years. Most of the cohort were females (n = 1,802, 90.8%) and Bahraini (n = 1,699, 85.6%). The most common comorbidities among patients with UTIs were diabetes mellitus (n = 399, 20.1%), hypertension (n = 356, 17.9%) and recurrent renal stones (n = 61, 3.1%) [Table 1].
E. coli (n = 1,220, 61.5%), Klebsiella (n = 342, 17.2%) and Streptococcus agalactiae (n = 154, 7.8%) were the most prevalent uropathogens across all age groups [Table 2].
Most cases of E. coli were sensitive to nitrofurantoin (n = 1,199, 98.3%), ciprofloxacin (n = 972, 79.7%) and trimethoprim/sulfamethoxazole (n = 865, 70.9%). For Klebsiella, sensitivity was observed for ciprofloxacin (n = 314, 91.8%) and trimethoprim/sulfamethoxazole (n = 269, 78.7%). In the case of Enterococcus and Pseudomonas aeruginosa, sensitivity testing was performed only for ciprofloxacin, which showed a high sensitivity profile (80.0% and 94.1%, respectively). Additionally, nitrofurantoin and ciprofloxacin exhibited the highest sensitivity rates for resistant organisms (91.0% and 60.2%, respectively) [Table 3].
Of all urine cultures, 20.8% (n = 412) were attributed to resistant uropathogens, with ESBL organisms being the most prevalent (n = 401, 20.2%). Higher rates of resistant uropathogens were noted in patients with diabetes mellitus (P <0.001), hypertension (P <0.001), those who had used antibiotic agents in the past 3 months (P <0.001), individuals who were hospitalised in the last three months (P <0.001) and patients with a history of ESBL (P <0.001) or CRE (P = 0.019). Additionally, patients with resistant uropathogens were older than their counterparts (P <0.001) [Fig. 1 and Table 4].
Distribution of uropathogens according to the presence and type of resistant uropathogens. ESBL = extended-spectrum β-lactamase Enterobacterales; MRSA = methicillin-resistant Staphylococcus aureus; CRE = carbapenem-resistant Enterobacterales; MDR = multidrug-resistant organism; VRE = vancomycin-resistant Enterococci.
Logistic regression analysis showed that participants who had used antibiotics in the past 3 months (odds ratio [OR] = 1.470; P = 0.002) and those who had been hospitalised (OR = 1.762; P = 0.017) exhibited a nearly twofold increase in the resistant UTI rate. A personal history of ESBL was associated with a threefold increase in the risk of harbouring resistant uropathogens (OR = 3.347; P < 0.001). Furthermore, patients with UTIs caused by resistant uropathogens were older than their non-resistant counterparts (P = 0.002) [Table 5].
4. Discussion
This study aimed to determine the clinical and microbiological profiles of patients with UTIs in primary healthcare centres in Bahrain, as well as the prevalence and predictors of resistant uropathogens. In line with published data, this study found that females constituted the majority of UTI cases in primary care settings.^1810^ Furthermore, the results revealed that elderly patients had a higher rate of UTIs compared to the paediatric population. Similarly, many studies have reported that UTI rates increase with age.
The predominance of E. coli (61.5%), Klebsiella and Streptococcus as the most common uropathogens across all age groups aligns with findings from other research.^19^ Additionally, most of these uropathogens were found to be sensitive to nitrofurantoin, ciprofloxacin and trimethoprim/sulfamethoxazole. Specifically, E. coli exhibited high sensitivity to nitrofurantoin and high resistance to cephalothin (38.0%), while Klebsiella showed high sensitivity to ciprofloxacin (91.8%) and relatively high resistance to nitrofurantoin (33.0%). Most E. coli and Klebsiella cases were sensitive to trimethoprim/sulfamethoxazole. These findings are consistent with a previous study in Bahrain.^9^ Additionally, they support the guidelines recommending nitrofurantoin and trimethoprim/sulfamethoxazole as first-line agents. This is further substantiated by the higher sensitivity rates of resistant organisms to nitrofurantoin compared to other antibiotics. Although E. coli and Klebsiella showed high sensitivity to fluoroquinolones, including ciprofloxacin, these agents should not be recommended as first-line empiric therapy, as they are considered drivers of resistance and collateral damage.^13^ Consistent with previous studies, the current study showed that most E. coli and Klebsiella species were sensitive to amoxicillin-clavulanic acid. In contrast, most resistant uropathogens exhibited resistance to amoxicillin-clavulanic acid, cephalothin and cefuroxime.^151617^
Furthermore, the prevalence of resistant uropathogens varies across studies. In this study, almost 1 in 5 patients with UTIs had a resistant organism. In the literature, the rates of resistant uropathogens reached as high as 50% in some studies, while in others, they did not exceed 5%.^6^ The variation in prevalence may be due to differences in settings, selection criteria, populations and patients' risk factors. In the current study, ESBL-producing organisms were the most common resistant uropathogens (20.2%), which aligns with global trends in antibiotic resistance. A previous study conducted in Bahrain showed comparable results.^10^
The impact of patient age on the risk of resistant uropathogen has been studied in the literature. The current study found that an increase in participants' age correlates with a heightened risk of resistant uropathogen. Some studies have reported a higher prevalence of resistant microorganisms among older patients with UTIs.^115^ Additionally, elevated rates of resistant uropathogens were noted in participants who had used antibiotic agents within the past 3 months. Similar findings have been reported in a few other studies, which observed comparable increases in antibiotic resistance among patients with recent antibiotic exposure.^9101112^ In line with the existing literature, this study found that previous infections with resistant uropathogens, such as ESBL producers, increase the risk of having subsequent resistant uropathogens.^18^
Although the univariate analysis showed higher rates of resistant uropathogens among patients with diabetes and hypertension, logistic regression results showed no significant difference. Many studies have reported higher rates of resistant microorganisms in patients with UTIs and diabetes compared to non-diabetic patients.^1112^ The link between hypertension and the risk of resistant uropathogens has not been established in the literature.^1920^
The high prevalence of resistant uropathogens discussed in this paper highlights the urgency of addressing this challenge. Primary healthcare physicians should use appropriate antibiotic therapies to treat UTIs based on sensitivity profiles and implement effective infection control measures to mitigate the spread of resistant organisms. Additionally, establishing surveillance programmes for resistant organisms is essential to control the spread of such infections in primary care settings.
This study has several strengths. It is the first study to analyse the clinical characteristics of patients with UTIs and the resistance patterns in the primary healthcare setting in Bahrain. All cases with positive urine cultures were included in the study, and multiple variables were collected, thereby eliminating the risk of sampling bias. Both univariate and logistic regression analyses were performed. Nonetheless, this study also has some limitations. A retrospective cross-sectional design was adopted, which limits the ability to establish causality or temporality between variables. Furthermore, the study included only culture-positive cases, while a significant number of UTI patients were treated empirically without a urine culture as per local practices and guidelines. This limitation may explain the high rate of resistance found in the study and may not fully represent the true burden of UTIs and the resistance situation within the population.
5. Conclusion
A substantial proportion of UTI cases in primary care settings in Bahrain were caused by resistant uropathogens, particularly ESBL organisms. Risk factors such as advanced age, recent antibiotic use, previous hospitalisation and a personal history of ESBL infections were associated with higher rates of resistant uropathogens. These findings underscore the urgent need for proactive measures to address antibiotic resistance in the management of UTIs. This includes the development of tailored antibiotic regimens based on local sensitivity patterns and targeted interventions to mitigate the risk factors associated with resistant uropathogens. Further research and surveillance are warranted to monitor and address the evolving landscape of antibiotic resistance in UTIs, ultimately contributing to more effective management and control of these infections in primary healthcare settings in Bahrain.
Authors' Contribution
Mahmood Alawainati: Conceptualization, Methodology, Formal analysis, Writing - Original Draft, Writing - Review & Editing. Zahra Ayoob: Investigation, Writing - Review & Editing.
Eman Almajed: Investigation, Writing - Review & Editing. Safaa Alkhawaja: Conceptualization, Methodology, Writing - Original Draft, Writing - Review & Editing. Noof Abdulaal: Investigation, Writing - Review & Editing. Rehab Alkhnaizi: Investigation, Writing - Review & Editing. Hanin Shaheen: Investigation, Writing - Review & Editing. Fatema Hubail: Investigation, Writing - Review & Editing. Nermin Kamal Saeed: Writing - Original Draft, Writing - Review & Editing.
Ethics Statement
Ethical approval was obtained from the Ethics Committee of Primary Healthcare on 7/3/2024.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sula I Alreshidi MA Alnasr N Hassaneen AM Saquib N. Urinary tract infections in the Kingdom of Saudi Arabia, a review. Microorganisms 2023; 11:952. https://doi.org/10.3390/microorganisms 11040952.10.3390/microorganisms 1104095237110375 PMC 10145783 · doi ↗ · pubmed ↗
- 2Medina M Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol 2019; 11:1756287219832172. https://doi.org/10.1177/1756287219832172.10.1177/175628721983217231105774 PMC 6502976 · doi ↗ · pubmed ↗
- 3Mancuso G Midiri A Gerace E Marra M Zummo S Biondo C. Urinary tract infections: The current scenario and future prospects. Pathogens 2023; 12:623. https://doi.org/10.3390/pathogens 12040623.10.3390/pathogens 1204062337111509 PMC 10145414 · doi ↗ · pubmed ↗
- 4Flores-Mireles AL Walker JN Caparon M Hultgren SJ. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol 2015; 13:269–84. https://doi.org/10.1038/nrmicro 3432.10.1038/nrmicro 343225853778 PMC 4457377 · doi ↗ · pubmed ↗
- 5Tenney J Hudson N Alnifaidy H Li JTC Fung KH. Risk factors for aquiring multidrug-resistant organisms in urinary tract infections: A systematic literature review. Saudi Pharm J 2018; 26:678–84. https://doi.org/10.1016/j.jsps.2018.02.023.10.1016/j.jsps.2018.02.02329991911 PMC 6035314 · doi ↗ · pubmed ↗
- 6Sula I Alreshidi MA Alnasr N Hassaneen AM Saquib N. Urinary tract infections in the Kingdom of Saudi Arabia, a review. Microorganisms 2023; 11:952. https://doi.org/10.3390/microorganisms 11040952.10.3390/microorganisms 1104095237110375 PMC 10145783 · doi ↗ · pubmed ↗
- 7Alhazmi AH Alameer KM Abuageelah BM Alharbi RH Mobarki M Musawi S. Epidemiology and antimicrobial resistance patterns of urinary tract infections: A cross-sectional study from Southwestern Saudi Arabia. Medicina (Kaunas) 2023; 59:1411. https://doi.org/10.3390/medicina 59081411.10.3390/medicina 5908141137629701 PMC 10456825 · doi ↗ · pubmed ↗
- 8Mohapatra S Panigrahy R Tak V Shwetha JV Sneha KC Chaudhuri S. Prevalence and resistance pattern of uropathogens from community settings of different regions: An experience from India. Access Microbiol 2022; 4:000321. https://doi.org/10.1099/acmi.0.000321.10.1099/acmi.0.00032135355869 PMC 8941965 · doi ↗ · pubmed ↗