The Rac sign: a transthoracic echocardiography sign that should prompt thorough evaluation of the coronary arteries
Panagioula Niarchou, George Michas, Efstathia Prappa, Athanasios Trikas

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
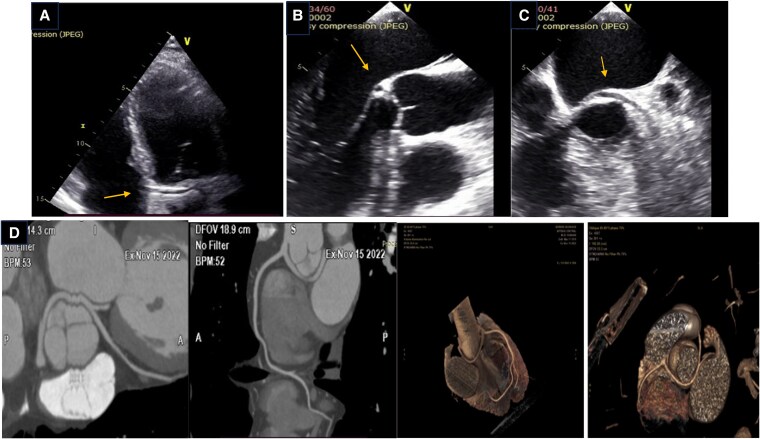 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Cardiac Arrhythmias and Treatments · Pericarditis and Cardiac Tamponade
Case description
A 56-year-old man was referred for routine checkup. He had medical history of arterial hypertension and engaged in intense sports activity. He was asymptomatic, with no history of syncope or angina. His ECG showed slight left axis deviation and sinus bradycardia. Transthoracic echocardiography revealed normal left ventricular volumes and global systolic function. Apical 5-chamber view revealed a vascular structure in the atrioventricular groove above the mitral annulus plane, crossing the aorta perpendicularly—consistent with the ‘retroaortic course’ (RAC) sign (Figure 1A; see Supplementary material online, Video S1).^1^ Detailed evaluation of the coronary artery (CA) origin in the short-axis view illustrated right CA origin, but left main origin failed to be identified. Moderate mitral regurgitation of unclear aetiology was also noted, prompting a transoesophageal study (TEE), before patient referral for Coronary Computed Tomography Angiography (CCTA). TEE confirmed the ‘RAC’ sign, and, in the long-axis view of the aorta below the non-coronary cusp, revealed a circular structure likely corresponding to the ‘bleb’ sign.^2^ (Figure 1B,C; see Supplementary material online, Video S2). Mitral valve appeared structurally normal. CCTA that followed revealed an anomalous origin of the left main from the proximal part of the right CA with a subsequent retroaortic course (Figure 1D; see Supplementary material online, Video S3), an extremely rare and potentially malignant anatomy since all three coronary branches originated from the RCA. Following ESC guidelines, the patient underwent a nuclear stress test on stationary bicycle, with no signs of ischaemia. Since there were no other high-risk features on CCTA, the patient was managed conservatively with strict cardiovascular risk control.
(A) Transthoracic echocardiography. Apical 5-chamber view. ‘RAC’ sign—a linear structure with vascular characteristics crossing transversely to the aorta (arrow). (B) Transoesophageal echocardiography. Mid-esophageal view at 120°: a circular structure below the non-coronary cusp, corresponding to the ‘bleb’ sign. (C) Transoesophageal echocardiography. Mid-esophageal view at 50°; the aorta is shown in short axis. A vascular structure with a retroaortic course is observed (arrow). (D) Coronary Computed Tomography Angiography. 2D slices and 3D reconstruction of the retroaortic course of the left main (LM) and the left coronary artery originating from the proximal right coronary artery.
Coronary artery anomalies (CAAs) refer to a group of congenital conditions including either an abnormal origin or course of any of the three main epicardial coronary arteries. While CCTA remains the gold standard for the diagnosis,^3^ routine echocardiography, particularly the RAC sign, can raise suspicion of a CAA, with reported high specificity (93.9%) compared with other echocardiographic markers.^1^
Supplementary Material
ytaf300_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Witt CM, Elvert LA, Konik EA, Ammash NM, Foley DA, Foley TA. The RAC sign: retroaortic anomalous coronary artery visualization by transthoracic echocardiography. JACC Cardiovasc Imaging 2018;11:648–649.28917682 10.1016/j.jcmg.2017.06.011 · doi ↗ · pubmed ↗
- 2Mancinelli A, Golino M, Miglierina E, My I, Crippa M, De Ponti R. Three echocardiographic signs to identify anomalous origin of the circumflex coronary artery from the right sinus of Valsalva: a case report. CASE (Phila) 2020;4:324–327.33117920 10.1016/j.case.2020.07.008PMC 7581641 · doi ↗ · pubmed ↗
- 3Frommelt P, Lopez L, Dimas VV, Eidem B, Han BK, Ko HH, et al Recommendations for multimodality assessment of congenital coronary anomalies: a guide from the American Society of Echocardiography: developed in collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 2020;33:259–294.32143778 10.1016/j.echo.2019.10.011 · doi ↗ · pubmed ↗